


Doris Hexsel1; Fernanda Oliveira Camozzato2; Aline Flor Silva3; Carolina Siega3
Introduction: Acoustic wave therapy stimulates tissue regeneration and healing processes. Therefore, it is expected that this treatment modality might have effects on scars.
Objective: To evaluate the efficacy and safety of acoustic wave therapy in the improvement of keloids.
Methods: An open, prospective, monocentric study was carried out with 20 participants with clinical diagnosis of keloid. Weekly sessions of acoustic wave therapy were performed, for eight weeks. Participants were assessed at baseline and at 1 and 12 weeks after the end of the treatment. The investigators took measurements of elasticity and performed clinical evaluations based on the Vancouver Scars Scale. At the end of the treatment the participants’ satisfaction with the treatment was evaluated.
Results: After the treatment, the percentage of participants with keloid thickness between 2mm and 5mm decreased to 47% (from 71%), increasing the percentage of participants with reduced keloid thickness in the total sample (<2mm, to 41% from 24%). Some participants also had improvement in the keloids’ vascularization and pliability. No treatment-related adverse events have been reported.
Conclusions: Acoustic wave treatment is safe and can be effective in the improvement of the keloid’s functionality and some clinical aspects.
Keywords: KELOID; CICATRIX; SCALES
Acoustic wave therapy (AWT®) is a non-invasive technique that relies on the mechanical stimulation of tissues by acoustic waves. This method originated from extracorporeal shock wave lithotripsy used in urology. For cosmetic purposes, much lower intensity is applied, thus it stimulates the healing and regeneration processes while avoiding tissue destruction.1
Acoustic waves stimulate cells, increase microcirculation and local metabolism, and trigger the release of signaling substances.1 When applied over the scar tissue, they seem to promote scar remodeling through the rupture of collagen fibers. The AWT® has been used in the treatment of connective tissue fibrosis, such as Peyronie's disease, burns and hypertrophic scars.2,3 The results obtained in the treatment of fibrosis and scarring suggest that this technique may also be effective in the treatment of keloids.
Hypertrophic scars and keloids result from the excessive growth of dense fibrous tissue, which may take place after surgical incision or injuries caused by trauma.4 Whereas hypertrophic scars are characterized by remaining restricted to the borders of the original injury, presenting its shape, keloids grow beyond the borders of the original wound, and are usually symptomatic, associated with pruritus, pain and pulling sensation. In general, they do not resolve spontaneously.5
Different treatment modalities have already been tested for keloids, such as surgical resection, radiation, lasers,6 radiofrequency,7 superficial or intralesional cryotherapy,8,9 application of pressure,4 and intralesional injections.10 Several actives have been used in intralesional treatment as monotherapy or in combination with other treatments or actives. Triamcinolone aceto-nide,11 5-fluoracil,12-14 bleomycin sulphate,15,16 and verapamil17,18 are some of the most studied treatments. Despite this range of therapeutic modalities, there is no consensus on which is the best approach for the treatment of keloids.4
The present study evaluated the efficacy and safety of AWT® for the improvement of keloids.
An open, prospective, monocentric study was conducted from 2013 to 2016 at the Brazilian Center for Studies in Dermatology, in Porto Alegre, Brazil. The study was approved by the Ethics Committee of Moinhos de Vento Hospital Association. All the subjects signed an Informed Consent prior to their inclusion in the study.
Subjects
Twenty healthy subjects aged between 18 and 60 years and with keloid were included in the study.
The main inclusion criterion was to have at least one keloid lesion measuring at least 2 cm2 in any part of the body, except for the face and areas of bone prominence. The main exclusion criteria were: pregnancy, lactation or intention to become pregnant during the study period, inflammation or active infection in the study area, and having undergone any treatment for keloids in the six weeks previous the study start.
Treatment protocol
All the subjects followed the same protocol, composed by 1 session per week for 8 weeks, totaling 8 sessions. The minimum interval between sessions was 5 days.
The AWT® was performed with C-Actor® handpiece of Cellactor SC1 (Storz Medical AG, Switzerland), which is a high--intensity electromagnetic system that generates planar acoustic waves. The treatment was applied to one keloid per subject, with back and forth movements and slight pressure. Each treatment session consisted of 250 (± 10%) pulses per cm2, with energy varying from 0.56 to 0.88mJ / cm2, as recommended by the manufacturer. A long standoff made of silicone was used to concentrate the energy of the equipment, and a layer of ultrasound gel was applied after cleansing the skin for better contact and transmission of energy. All treatment sessions were performed by trained professionals.
Evaluations
Each subject attended to 3 evaluation visits: baseline (T0), 1 week after the end of the 8-session treatment (T1) and 12 weeks after (T2). At the baseline visit (T0), the investigators carried out a clinical and physical evaluation, verified the inclusion and exclusion criteria, reviewed the patient’s medical history and medications use, and assessed the keloid elasticity and its classification according to the Vancouver Scars Scale.19 Women of childbearing potential underwent a urinary pregnancy test.
Clinical and keloid evaluation, in addition to the verification of possible adverse events, were performed in all visits after the treatment. All evaluations were performed by a dermatologist.
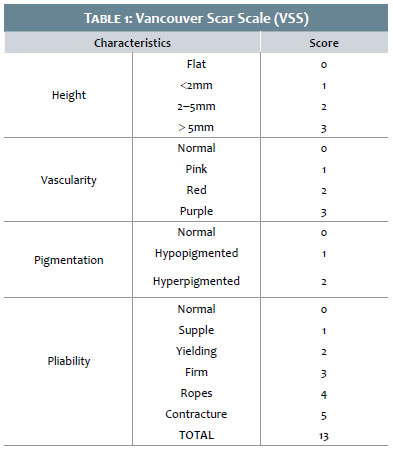
The Vancouver Scar Scale (VSS)
The primary outcome was defined as the clinical improvement of keloid lesions assessed by the Vancouver Scars Scale,19 -a validated scale to evaluate scars (Table 1).
Elasticity measurements
The elasticity of the keloid lesion was evaluated at all visits with the assistance of the Cutometer® MPA 580 device (Courage-Khazaka, Germany). The R5 parameter — which indicates the variation of skin elasticity — was defined as the evaluation parameter. It varies between 0 and 1 (the closer to 1, the more elastic is the skin).
Measurements were taken at the midpoint of each lesion (treated area), and on the internal part of the right forearm, at the midpoint between the wrist and the antecubital fossa medial line, on the ventral surface (control-area).
Patient satisfaction questionnaire
In all follow up visits after the end of the last session, the subjects answered a satisfaction questionnaire. They were asked to describe their perception about the improvement of pain and discomfort when moving the treated region, and about the improvement in the appearance of the scar using the following ratings: significantly improved, improved, slightly improved, unchanged, slightly worsened, worsened, significantly worsened, or not applicable (when no pain or discomfort was perceived in the keloid area). In addition, subjects answered whether they were satisfied with the treatment and whether they would undergo it again.
Statistical analysis
Demographic data were presented descriptively for the intention-to-treat population. The outcomes of the evaluations considered the population per protocol. Categorical variables were presented as percentages and quantitative variables as mean values ± standard deviation. Differences in the elasticity and in the final mean value of the scars scale were tested with ANOVA for repeated measures.
Twenty-two subjects were evaluated, but two did not start the treatment, and were therefore excluded from data evaluation. Of the 20 enrolled subjects , 17 completed the study, and three were unavailable to complete the study: 2 withdrew during the treatment period, and 1 after the follow-up visit at the end of the last session.
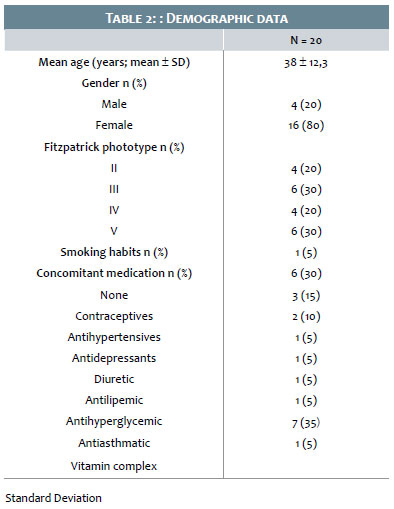
The mean age of the subjects was 37.8 ± 12.4 years (range: 19-61), and most were women. Half of the subjects were Fitzpatrick phototypes II and III, while the other half were phototypes IV and V. The demographic data of the 20 subjects who started the treatment are described in Table 2.
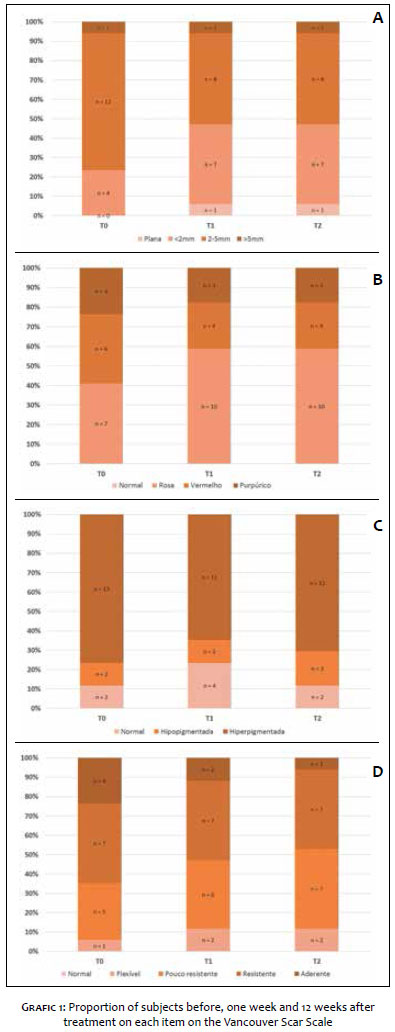
Graphs 1a-d show the proportion of subjects at each visit, for each Vancouver Scar Scale scoring item. Keloid height varied from 2mm to 5mm for most of the subjects (71%, n = 12) at baseline. After 8 treatment sessions, less than half of the subjects (47%, n = 8) still presented keloids height between 2mm and 5mm, and the proportion of subjects presenting keloid height less than 2mm increased from 24% (n = 4) at baseline to 41% (n = 7) after the end of the treatment. One subject who had a keloid height of less than 2mm at the baseline presented a flat lesion after treatment.
Vascularization did not normalize in any case, either before or after the end of the treatment. Pink coloration was observed in 41% of the subjects at baseline, increasing to 59% in the post-treatment follow-up evaluations. The proportion of subjects who presented reddish coloration decreased from 35% at baseline to 24% in the post-treatment follow-up evaluations, and purpuric coloration decreased from 24% to 18%. Present in most subjects at baseline (76%; n = 13), hyperpigmentation decreased to 65% (n = 11) and 71% (n = 12) in subsequent evaluations.
The pliability of the keloid was graded as contracture in 24% (n = 4) of the subjects at baseline, in 12% (n = 2) one week after treatment and in 6% (n = 1) 12 weeks after treatment. The proportion of keloid lesions considered yielding and supple increased from 29% and 6%, respectively, to 35% and 12% one week after treatment, and to 41% and 12% 12 weeks after treatment.
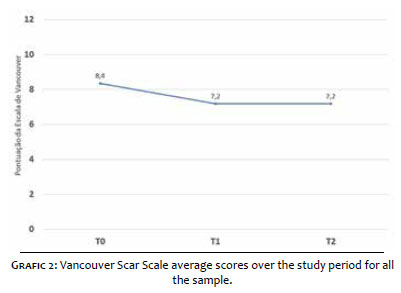
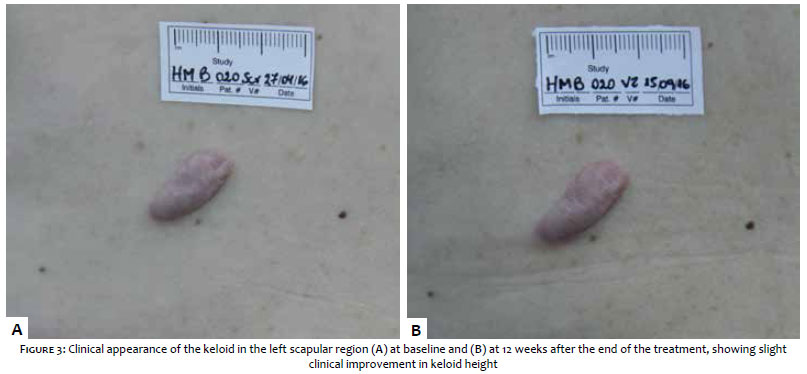
The mean total VSS score presented a statistically significant reduction in the follow up evaluations when compared to the baseline value (Graph 2). Nevertheless, only a slight improvement could be perceived by visual observation (Figure 3A and B).
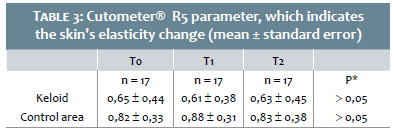
The skin elasticity values in the keloid lesion and in the control-area, assessed with Cutometer®, are described in Table 3.
No statistically significant difference was observed in the results obtained before and after treatment in both areas.
Among the subjects who completed the study, 76.5% considered the treatment protocol improved the keloid’s appearance. The same proportion of subjects was satisfied with the treatment, and 82.4% would undergo the procedure again. At the beginning of the study, 14 subjects had discomfort when moving the area affected by the keloid, and 11 subjects had pain. After treatment, 12 (85.7%) reported improvement in discomfort and 9 (81.8%) reported improvement in pain.
No treatment-related adverse events have been reported. Two subjects presented adverse events, both not related to their participation in the study.
The treatment of keloid is challenging, with limited therapeutic options capable to reach positive outcomes in the aesthetical appearance of the lesion. In the present study, the authors evaluated the effects of a protocol comprising eight sessions of acoustic wave therapy to improve the clinical appearance of keloid lesions in different areas of the body.
The proportion of patients presenting with more severe degrees of keloid height, vascularity, and pliability decreased after treatment, as did the mean of the overall VSS score. However, the clinical improvement was poor from the aesthetic point of view. The photographic and visual evaluations did not show clearly clinical improvement in the appearance of the treated lesions (Figure 3A and B).
Even though no significant aesthetic improvement was obtained in the treated lesions, it was possible to observe a high proportion of subjects satisfied with the treatment. Studies evaluating the efficacy of other treatment modalities for keloid, such as bleomycin sulphate and intralesional corticosteroid injections, have also showed a high percentage of satisfied patien-ts.20,21 Improvement in discomfort and pain due to movement was observed in more than 80% of the subjects who reported these symptoms at baseline. Manca et al. observed pain reduction in up to 94% of the patients evaluated in their study.20 They considered that satisfaction is mainly linked to the improvement in the clinical symptoms of pain and discomfort under movement. Another hypothesis is that the high satisfaction of the subjects was linked to the low expectations regarding the effectiveness of the treatments for this condition.
The evaluation of skin elasticity using an elastometer did not indicate significant changes in the keloid area after the treatment as compared to pre-treatment conditions. Draaijers et al.22 described the validity of this methodology for the evaluation of elasticity in scars. Van Leeuwen et al.9 reported a 57% improvement in the elasticity of successfully treated lesions. However, they observed worsening of 50% in recurrent lesions.
The present study showed that AWT® is safe and effective in the functional improvement of keloids. The treatment did not significantly change keloid scars, since no lesion completely disappeared or changed types (for example, from keloid to hypertrophic scar). Improvements in keloid height, vascularity and pliability were observed in a proportion of patients after the 8-week session protocol. Comparative studies with larger samples or even in association with other procedures may provide additional data on the effectiveness of this treatment, also for other types of scars.
1. Novak P. Acoustic Wave Therapy for Treating Cosmetic Disorders. IPRAS: Proceedings of the 15th World Congress of the International Confederation for Plastic Reconstructive and Aesthetic Surgery; 2009 Nov-29-Dez03; New Delhi, India. Bologna: MEDIMOND International Proceedings; 2009. p. 83-8.
2. Fiaramonti P, Cigna E, Onesti MG, Fino P, Fallico N, Scuderi N. Extracorporeal shock wave therapy for the management of burn scars. Dermatol Surg. 2012;38(5):778-82.
3. Christ C, Brenke R, Sattler G, Siems W, Novak P, Daser A. Improvement in skin elasticity in the treatment of cellulite and connective tissue weakness by means of extracorporeal pulse activation therapy. Aesthet Surg J. 2008;28(5):538-44.
4. Leventhal D, Furr M, Reiter D. Treatment of keloids and hypertrophic scars: a meta-analysis and review of the literature. Arch Facial Plast Surg. 2006;8(6):362-8.
5. Carroll W, Patel K. Steroids and fluorouracil for keloids and hypertrophic scars. JAMA Facial Plast Surg. 2015;17(2):77-9.
6. Rossi A, Lu R, Frey MK, Kubota T, Smith LA, Perez M. The use of the 300 microsecond 1064 nm Nd:YAG laser in the treatment of keloids. J Drugs Dermatol. 2013;12(11):1256-62.
7. Weshay AH, Abdel Hay RM, Sayed K, El Hawary MS, Nour-Edin F. Combination of radiofrequency and intralesional steroids in the treatment of keloids: a pilot study. Dermatol Surg. 2015;41(6):731-5.
8. Mourad B, Elfar N, Elsheikh S. Spray versus intralesional cryotherapy for keloids. J Dermatolog Treat. 2016;27(3):264-9.
9. van Leeuwen MC, Bulstra AE, Ket JC, Ritt MJ, van Leeuwen PA, Niessen FB. Intralesional cryotherapy for the treatment of keloid scars: evaluating effectiveness. Plast Reconstr Surg Glob Open. 2015;3(6):e437.
10. Ledon JA, Savas J, Franca K, Chacon A, Nouri K. Intralesional treatment for keloids and hypertrophic scars: a review. Dermatol Surg. 2013;39(12):1745-57.
11. Danielsen PL, Rea SM, Wood FM, Fear MW, Viola HM, Hool LC, et al. Verapamil is Less Effective than Triamcinolone for Prevention of Keloid Scar Recurrence After Excision in a Randomized Controlled Trial. Acta Derm Venereol. 2016;96(6):774-8.
12. Bijlard E, Steltenpool S, Niessen FB. Intralesional 5-fluorouracil in keloid treatment: a systematic review. Acta Derm Venereol. 2015;95(7):778-82.
13. Darougheh A, Asilian A, Shariati F. Intralesional triamcinolone alone or in combination with 5-fluorouracil for the treatment of keloid and hypertrophic scars. Clin Exp Dermatol. 2009;34(2):219-23.
14. Shah VV, Aldahan AS, Mlacker S, Alsaidan M, Samarkandy S, Nouri K. 5-fluoracil in the treatment of keloids and hypertrophic scars: a comprehensive review of the literature. Dermatol Ther (Heidelb). 2016;6(2):169-83.
15. Saray Y, Güleç AT. Treatment of keloids and hypertrophic scars with dermojet injections of bleomycin: a preliminary study. Int J Dermatol. 2005;44(9):777-84.
16. Aggarwal H, Saxena A, Lubana PS, Mathur RK, Jain DK. Treatment of keloids and hypertrophic scars using bleom. J Cosmet Dermatol. 2008;7(1):43-9.
17. Wang R, Mao Y, Zhang Z, Li Z, Chen J, Cen Y. Role of verapamil in preventing and treating hypertrophic scars and keloids. Int Wound J. 2016;13(4):461-8.
18. Verhiel S, Piatkowski de Grzymala A, van der Hulst R. Mechanism of action, efficacy, and adverse events of calcium antagonists in hypertrophic scars and keloids: a systematic review. Dermatol Surg. 2015;41(12):1343-50.
19. Baryza MJ, Baryza GA. The Vancouver Scar Scale: an administration tool and its interrater reliability. J Burn Care Rehabil 1995;16(5):535-8.
20. Manca G, Pandolfi P, Gregorelli C, Cadossi M, de Terlizzi F. Treatment of keloids and hypertrophic scars with bleomycin and electroporation. Plast Reconstr Surg. 2013;132(4):621e-630e.
21. Kim DY, Park HS, Yoon HS, Cho S. Efficacy of IPL device combined with intralesional corticosteroid injection for the treatment of keloids and hypertrophic scars with regards to the recovery of skin barrier function: A pilot study. J Dermatolog Treat. 2015;26(5):481-4.
22. Draaijers LJ, Botman YA, Tempelman FR, Kreis RW, Middelkoop E, van Zuijlen PP. Skin elasticity meter or subjective evaluation in scars: a reliability assessment. Burns. 2004;30(2):109-14.
This study was carried out at the Centro Brasileiro de Estudos em Dermatologia. (CBED) Porto Alegre (RS), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}