


Mario Cezar Pires1; Maria do Rosario Vidigal2; Natalia Ivanoff dos Reis3; Lucia Romanó Santos3; Anita Rotter4; Liliana Bechelli de Oliveira Torloni5
Introduction: The use of moisturizers improves the skin barrier’s function and might be useful in atopic dermatitis.
Objectives: To assess the efficacy and safety of an active moisturizer-barrier repairer based on glycerin, erythritol, Imperata cylindrica and homarine as an adjuvant treatment in atopic dermatitis.
Methods: Application of the moisturizer in children with mild to moderate atopic dermatitis for 1 month, with subjective and objective evaluations after 15 and 30 days.
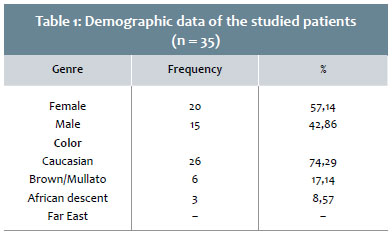
Results: Data from 35 children — 20 girls (57.15%), 15 boys (42.86%) / 26 Caucasians (74.29%), 6 mulattos (17.14%), 3 dark skinned (8.57%) — aged 1 to 10 years (mean age = 5.6) were analyzed. The values of the variables sleeping disorders, dryness, desquamation, pruritus and softness of the skin had significantly decreased on the 30th day of treatment as compared to the baseline. The objective evaluation of the severity using the Scoring Atopic Dermatitis severity index revealed a decrease to 9.30 from 25.27 (p <0.0001). There was a reduction in the use of dexchlorpheniramine and hydrocortisone to 5.72% each on the 30th day, from 25.71% (p = 0.0233) and 34.29% (p = 0.0075) on the 15th day, respectively.
Conclusions: The use of the moisturizer for 30 days improved the analyzed symptoms with a significant reduction in the Scoring Atopic Dermatitis severity index with decreased need for antihistamines and topical corticosteroids. The use of a suitable moisturizer was effective and safe as an adjuvant treatment for children with atopic dermatitis.
Keywords: DERMATITIS, ATOPIC; HYGROSCOPIC AGENTS; CHILD
Atopic dermatitis (AD) is a chronic, recurrent and pruriginous inflammatory skin disease resulting from a complex interdependence of genetic, immunological, and environmental factors.1 It occurs most often in childhood, however may persist into adulthood in roughly 40-60% of cases,2,3 causing substantial psychological and physical discomfort for patients and their families, with a considerable impact on the quality of life.4
In most cases, its signs and symptoms emerge in early childhood. It is estimated that 50% of new cases occur in the first year of life, with 85% of cases beginning before the age of five. It is the most important chronic dermatologic disease in this age group.1 The cardinal symptom of AD is pruritus, even in infants and young children, leading to restlessness or difficulty to fall asleep. Xerosis is another frequent sign in AD, resulting from several alterations in barrier function, such as increased transepidermal water loss, decreased ceramides 1 and 3, decreased fatty acids and cholesterol in the skin. Eczematous lesions vary according to the age group, being predominantly acute up to two years of age, subacute up until puberty and chronic in adults, however with surges at any time of life.1
The clinical diagnostic criteria of Hanifin and Hajka were introduced in 1980 and are still currently used for the diagnosis of AD in clinical studies, taking into account the main signs and symptoms of the condition.5
Basic control of AD requires efficient control of surges by treating inflammatory symptoms and promoting the reestablishment of the skin’s barrier homeostasis, in addition to avoiding aggravating or triggering factors of the disease.6 Topical and immunomodulatory corticosteroids are the first line of treatment for disease surges, while long-term control is based on the use of moisturizers aimed at maintaining the skin’s barrier integrity, relieving pruritus and preventing further surges.7-9 Although some studies have shown that the use of moisturizers increase the therapeutic response and improve results, there are few reports on the isolated application of these products in children bearing mild and moderate conditions.10,11
For these reasons, the authors of the present study investigated the effects of a formulation containing moisturizing ingredients (glycerin and erythritol), lipid components (ceramides and omegas), and botanical active principles with osmoregulatory properties (Imperata cylindrica and homarine) for reducing the severity of the lesions, relieving pruritus, and improving cutaneous hydration, sleeping disorders and tolerability in pediatric patients with mild to moderate AD.
To evaluate the efficacy and tolerability of a topical moisturizing product used as an adjuvant in the treatment of mild to moderate AD in children.
The present study was analyzed and approved by the Research Ethics Committee of the Complexo Hospitalar Padre Bento de Guarulhos, in the Brazilian State of São Paulo. At least one individual legally responsible for the patient (the mothers, in general) signed the Free and Informed Term of Consent after having received an explanation and understanding the scientific purpose of the results. Children who were already literate, read and signed the Term of Consent.
The inclusion criteria were:
• both genders, aged between 3 months and 10 years of age;
• presence of pruritus;
• presence of mild eczema according to the severity score SCORAD (Score On AD)5
• at least 1 week without using moisturizer and / or corticosteroid orally;
• at least 1 month without injectable corticosteroid;
• at least 72 hours without using antihistamine;
• no known history of allergic reaction to products of the same category as the test product or to the supportive products;
• absence of diseases that, at the discretion of the investigator, could interfere with the clinical evaluation or the visitation schedule.
The investigator excluded the children according to the following criteria: those who had carried any risk or bore any condition that could interfere with the study’s objectives; those with history and obvious clinical signs of intense exposure to the sun; female patients who had undergone menarche. During the course of the study, the following events also triggered the exclusion of patients: history and obvious clinical signs of intense exposure of the body to the sun since the previous visit; use of oral or injectable corticosteroids; application of another body moisturizing product; any other reason that, at medical discretion, offered a risk to the patient or interfered with the purpose of the study; failure to use investigated product for 3 consecutive days or 7 non-consecutive days during the 30 days of the treatment.
Study Design
Forty patients bearing AD were selected according to the Hanifin and Rajka criteria to undergo a clinical, open, prospective, phase IV study.5
The individuals responsible for the patients were instructed to apply the moisturizing product once a day throughout the skin after having bathed the patient. Evaluations were carried out at baseline (D0), 15 days after (D15) and 30 days after (D30). During the 30 days of the study, patients were allowed to use a rescue medication, with oral dexchlorpheniramine, at the recommended dose for the age, for pruritus symptoms; and hydrocortisone cream twice a day in case of skin lesions. The responsible parties were given a diary in which they should record signs, symptoms and use of the rescue medication during the 30 days of observation. The moisturizer’s safety was assessed at visits D15 and D30 through reports of adverse events and the completion of tolerability questionnaires. The SCORAD Index — based on the extent of the lesions, on the degree of xerosis, and on the presence of erythema, edema, crusts, scratching signs, lichenification, as well as the intensity of daytime and nighttime pruritus9 — in addition to the evaluation ofpruritus, intensity of symptoms, sleeping disorders and the clinical examination of the lesions at D0, D15 and D30, were used by the researchers for the clinical analysis of efficacy. Only children with SCORAD degrees considered mild or moderate were selected for the study. In the subjective analysis based on questionnaires filled out by the responsible parties, the following variables were considered: sleeping disorders; degree of pruritus (in a scale ranging from 1 to 10), skin’s dryness, desquamation, degree of hydration and softness.
In order to describe the profile of the sample according to the studied variables, frequency tables of the categorical variables were prepared with absolute frequency values (n), percentages (%) and descriptive statistics of the numerical variables, with values mean values, standard deviations, minimum and maximum values and medians.
ANOVA for repeated measures was used to compare numerical scores. The data were transformed into ranks due to the absence of normal. The McNemar's test was employed to compare categorical results.
The adopted level of significance was 5% (0.05) and the statistical analysis was performed using the software SAS (Statistical Analysis System), version 9.4., SAS Institute Inc, 2002-2015, Cary, NC, USA.
Patient profile
Of the 40 children selected, 5 were excluded due lack of compliance with the study’s protocol, such as use of oral corticosteroids and failure to attend D15 or D30 visits. Thirty-five children were considered in the final analysis.
The predominant profile of the patients who completed the study was Caucasian children (Table 1) of 1 to 10 years of age (mean = 5.6 years, median = 6 years).
Subjective analysis
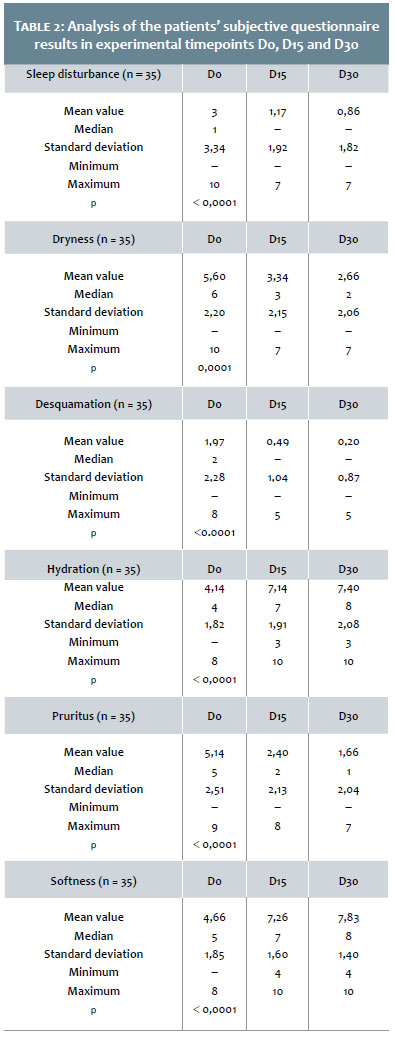
All parameters evaluated in the patients who completed the study showed significant variation of the scores between the baseline visit (D0) and the experimental points D15 and D30. There was no significant variation in outcomes between timepoints D15 and D30, except for pruritus, which presented a significant reduction (Table 2).
Clinical evaluation
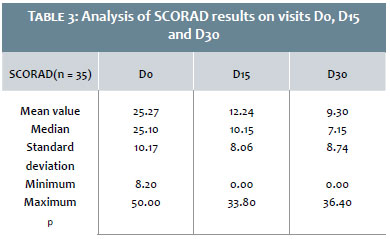
For the sample that concluded the study, there was a significant decrease in the SCORAD between D0 (baseline) and D15, D0 and D30, and D15 and D30. Regarding the intensity of symptoms, pruritus and sleeping disorders, there was a significant reduction of the scores in the comparison between visits D0 and D15, and D0 and D30 (Table 3).
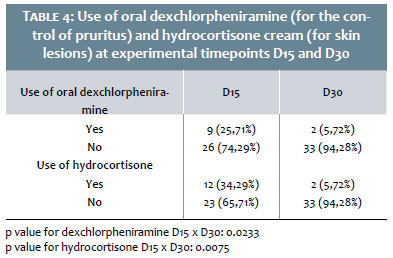
Another parameter analyzed regarding the moisturizer’s effectiveness was the comparison between the use of supportive medications — namely dexchlorpheniramine and hydrocortisone — in visits D15 and D30. As observed in Table 4, there was a clear decrease in the need for dexchlorpheniramine and hydrocortisone between the two visits.
There was a statistically significant reduction in the use of both dexchlorpheniramine and hydrocortisone between visits D15 and D30.
Tolerability
The tolerability was considered excellent by 94.29% of patients in D15 and by 97.14% in D30. There was no report of either regular or poor tolerability. Regarding the sensations of pruritus, burning, pinching and comfort, there was no significant change in results between visits D15 and D30, with adequate tolerability during the period of product use.
AD is deemed as one of the most prevalent childhood dermatological diseases. In Brazil, it affects 5 to 10% of children under 12 years of age, depending on the geographic region. It causes a great impact in the life of these children and their families, especially due to the appearance of the skin lesions and pruritus — always present and in varying degrees. Dry skin is one of the main signs of AD, with several repercussions for the body.
Increasing evidence suggests that skin barrier dysfunctions promote the development of and worsen AD.12 Defective synthesis of ceramides, in special of the types 1 and 3, has been linked to xerosis in AD.13 Alterations in at least three clusters of genes encoding structural proteins, epidermal proteases and protease inhibitors promote predisposition to an altered epidermal barrier and increased risk for AD.14 The strong association between genetic defects of the barrier and environmental aggressions that cause damage to it, suggests that this dysfunction is a primary event in the development of the condition.15 There are important changes in lipids in AD, such as reductions in ceramides and increased hydrolysis of sphingomyelin.14,15 The impairment of the barrier function is currently considered an important etiologic factor in the pathogenesis of AD in a significant number of patients. Filaggrin is key for the formation of the skin barrier and factors of natural humidification (a set of substances with hygroscopic functions that are metabolized from the hydrolysis of filaggrin). These factors prevent transepidermal water loss, blocking the entry of irritants, allergens, infectious agents and chemical offenders.16,17 In addition to filaggrin, the so-called envelope proteins — loricrin, involucrin and claudin — had proven their importance in the formation of the skin barrier, with a relevant role also in the dryness of the atopic skin.17 Today, all consensus guidelines for the control of AD consider not only cutaneous hydration, but also the recovery of the impaired barrier function, a crucial part of the short and long-term control of the condition.16-19
In line with the literature, there was predominance of the female gender for this age group in this study.1,4 Caucasians were the majority, which reflects the profile of the ambulatory’s care. The age group was in line with the expected: from 1 to 10 years of age, with a mean value of 5.6 years (Table 1).
The assessed product significantly improved the clinical picture of the studied children, regarding both the dryness and the degree of eczema. The subjective analysis of variables such as sleep disturbances, skin dryness and desquamation had a statistically significant reduction in timepoints D15 and D30, reflecting the effectiveness of the product used (Table 2). The degree of pruritus was also the subject of questioning for mothers (in the case of younger children) and for the patients themselves (in cases where they understood the question). The analog scale used in the questionnaires ranged from 0 to 10 points, with an initial mean value of 5.14, progressing to 1.66 after one month of treatment. In the literature, there are several studies reporting the efficiency of cutaneous hydration in improving pruritus in patients with AD.20,21 The most likely mechanism underpinning the improvement of pruritus with the use of moisturizers is probably linked to the recovery of the skin barrier.22 Despite the fact that it is a variable that suffers great subjective influence, the degree of softness of the skin evidenced a clear difference between the baseline and the final experimental timepoint (Table 2).
The researcher physicians, also evaluated participating children objectively, in special with the assistance of the SCORAD, which is one of the severity indexes most commonly described in the literature.
As can be seen in Table 3, there was a significant reduction of the SCORAD between the baseline and D15, and between D15 and D30, confirming the literature data, showing that cutaneous hydration decreased the signs and symptoms of mild to moderate AD. The SCORAD is probably the most commonly used and widely accepted severity score in the literature. It is based on the objective criteria obtained with clinical examination and on the degrees of daytime and nighttime pruritus. Aiming at reducing the subjectivism, evaluations were always performed by two physicians.
A major concern in the treatment of AD is the chronic use of corticosteroids, especially in the pediatric age group.9 A number of reports have shown side effects of topical corticosteroids, such as atrophy, acne, systemic absorption, glaucoma, and cataracts.9,23-25 Some studies have already demonstrated a corticosteroid-sparing effect with regular use of moisturizers, in addition to reduction of pruritus.26,27 Table 4 shows a clear reduction in the need for administration of the antihistamine dexchlorpheniramine between visits D15 and D30 (25.71% of the cases to 5.72%), objectively demonstrating the decrease in pruritus symptoms. Likewise, hydrocortisone was less frequently used in the second fortnight of product use, with a reduction from 34.29% to 5.72%, indicating the presence of the capability of sparing the corticosteroid contained in the moisturizer applied in the children. Based on literature data and in order to simplify the care with the children, the authors of the present article chose to apply the moisturizer only once a day after bathing.28 This does not seem to have influenced the outcomes, with good action having been evidenced from both the subjective and objective standpoints — including that of the corticosteroid-sparing effect.
More recently, reviews have corroborated the therapeutic action of moisturizers on the skin of patients bearing AD.29 Their cost effectiveness has been proven in maintaining the patients’ improvement, which makes them useful in the short and long term.30 Specifically in children, the association of moismoisturizers with the treatment showed beneficial effects, reducing the corticosteroids' risks and side effects.31,32 In the more recent literature, moisturizers are classified as true therapeutic agents in AD,31,32 which was confirmed by the present study.
In light of this, the authors of the present article reiterate the view that the use of suitable moisturizers in AD patients is no longer considered adjuvant, but an essential part of the treatment. The correct balance in the moisturizer's formulation, with ceramides, fatty acids, cholesterol and other components, is necessary for the sound correction of the impaired skin barrier. 1,9 On the other hand, atopic patients often have sensitive skin, preferably being treated with products without irritants, perfumes or any aggressive agent.7-9 The moisturizer evaluated in the present study has hydrating substances, such as glycerin and erythritol, lipid components (ceramides and omega acids) and osmoregulators (Imperata cylindrica and homarine). In the literature there is strong evidence of the action of glycerin-based moisturizers in the recovery of atopic skin. However, comparative studies of moisturizers are scarce.33 A systematic review of literature on the use of moisturizers in AD has shown that the most well-documented studies were performed on glycerin and urea.33 Nevertheless, those on glycerin alone were the most subject to methodological deviations.33 Erythritol is a humectant compound with an action similar to that of the glycerin, which strengthens its effect.34 There are also studies in the literature that have proved the osmoregulatory capacity of Imperata cylindrica.35 In this manner, the present study showed that the addition of other humectants and osmoregulators yields better outcomes, as compared to the isolated use of glycerin. The outcomes of the present study demonstrated a significant reduction in the SCORAD, with a baseline mean value of 25.27 that progressed to 9.30 by the end of the study, as well as improvement of pruritus and of the subjective and objective evaluations of AD.
The daily application of the moisturizer tested in the present study for 30 days reduced the symptoms of pruritus and dryness, and improved softness and hydration. In the objective analysis, there was a significant decrease in SCORAD, with the moisturizer also reducing the need for the use of antihistaminic and topical corticosteroids. Tolerability was considered excellent throughout the period of use of the moisturizer. Therefore, the present study demonstrated that the application of adequate moisturizers in patients with AD is a crucial part of the therapeutic armamentarium.
Mario Cezar Pires
Head researcher, evaluation of patients, preparation of the protocol, writing of the paper.
Maria do Rosario Vidigal
Co-researcher, evaluation of patients.
Natalia Ivanoff dos Reis
Co-researcher, review literature, evaluation of patients.
Lucia Romanó Santos
Co-researcher, literature review, evaluation of patients.
Anita Rotter
Co-researcher, preparation of the study protocol.
Liliana Bechelli de Oliveira Torloni
Co-researcher, preparation of the protocol
1. Pires MC, Cestari SCP. Dermatite atópica. Rio de Janeiro: Diagraphic Editora; 2005.
2. Boguniewicz M, Leung DYM. Atopic dermatitis: a disease of altered skin barrier and immune dysregulation. Immunol Rev. 2011;242(1):233-46.
3. Eyerich K, Novak N. Immunology of atopic eczema: overcoming the Th1/Th2 paradigm. Allergy. 2013;68(8):974-82.
4. Kiken DA, Silverberg NB. Atopic dermatitis in children, part 1: epidemiology, clinical features, and complications. Cutis. 2006;78(4):241-7.
5. Hanifin, J.M. and Rajka, G.: Diagnostic features of atopic dermatitis. Acta Derm Venereol Suppl (Stockh). 1980;92:44–47.
6. Angelova-Fischer I, Neufang G, Jung K, Fischer TW, Zillikens D. A randomized, investigator-blinded efficacy assessment study of stand-alone emollient use in mild to moderately severe atopic dermatitis flares. J Eur Acad Dermatol Venereol. 2014;28 Suppl 3:9-15.
7. Ring J, Alomar A, Bieber T, Deleuran M, Fink-Wagner A, Gelmetti C, et al. Guidelines for treatment of atopic eczema (atopic dermatitis) part I. J Eur Acad Dermatol Venereol. 2012;26(8):1045-60.
8. Hanifin JM, Cooper KD, Ho VC, Kang S, Krafchik BR, Margolis DJ, et al. Guidelines of care for atopic dermatitis, developed in accordance with the American Academy of Dermatology (AAD)/American Academy of Dermatology Association "Administrative Regulations for Evidence-Based Clinical Practice Guidelines". J Am Acad Dermatol. 2004;50(3):391-404.
9. Harper J, Oranje A, Prose N, editors. Textbook of Pediatric Dermatology. 1st ed. Oxford: Blackwell Science; 2000.
10. Pires MC, Sittart JA, Cestari SCP, Rodrigues RNS, Tkcaz RM. Estudo clínico multicêntrico, nacional, aberto, para avaliar a eficácia, a segurança e a tolerabilidade de um hidratante contendo alfa-bisabolol*, aloe vera, óleo de girassol e alantoína, como adjuvante no tratamento das dermatites atópicas leves. Rev Bras Med. 2006;63(8):378-83.
11. Heald P, Burton CS, Callaway L. Moisturizing the Skin. N C Med. 1983;44(4):234.
12. Cork MJ, Danby SG, Vasilopoulos Y, Hadgraft J, Lane ME, Moustafa M, et al. Epidermal barrier dysfunction in atopic dermatitis. J Invest Dermatol. 2009;129(8):19892-908.
13. De Benedetto A, Agnihothri R, McGirt LY, Bankova LG, Beck LA. Atopic dermatitis: a disease caused by innate immune defects? J Invest Dermatol. 2009;129(1):14-30.
14. Hvid M, Vestergaard C, Kemp K, Christensen GB, Deleuran B, Deleuran M. IL-25 in atopic dermatitis: a possible link between inflammation and skin barrier dysfunction? J Invest Dermatol. 2011;131(1):150-7.
15. Lynde CW, Andriessen A. A cohort study on a ceramide-containing cleanser and moisturizer used for atopic dermatitis. Cutis. 2014;93(4):207-13.
16. Lodén M. Role of topical emollients and moisturizers in the treatment of dry skin barrier disorders. Am J Clin Dermatol. 2003;4(11):771-88.
17. Draelos ZD. Concepts in skin care maintenance. Cutis. 2005;76(6 Suppl):19-25.
18. Kim JE, Kim HJ, Lew BL, Lee KH, Hong SP, Jang YH, et al. Consensus guidelines for the treatment of atopic dermatitis in korea (part i): general management and topical treatment. Ann Dermatol. 2015;27(5):563-77.
19. Wollenberg A, Oranje A, Deleuran M, Simon D, Szalai Z, Kunz B, et al. ETFAD/EADV Eczema task force 2015 position paper on diagnosis and treatment of atopic dermatitis in adult and pediatric patients. J Eur Acad Dermatol Venereol. 2016;30(5):729-47.
20. Weber TM, Samarin F, Babcock MJ, Filbry A, Rippke F, et al. Steroid-free over-the-counter eczema skin care formulations reduce risk of flare, prolong time to flare, and reduce eczema symptoms in pediatric subjects with atopic dermatitis. J Drugs Dermatol. 2015;14(5):478-85
21. Hon KL, Leung AK, Barankin B. Barrier repair therapy in atopic dermatitis: an overview. Am J Clin Dermatol. 2013;14(5):389-99.
22. Elias PM. Stratum corneum defensive functions: an integrated view. J Invest Dermatol. 2005;125(2):183-200.
23. Turpeinen M, Salo OP, Leisti S, et al. Effect of percutaneous absorption of hydrocortisone on adrenocortical responsiveness in infants with severe skin disease. Br J Dermatol. 1986;115(4):475-84.
24. Queille C, Pommarede R, Saurat JH. Efficacy versus systemic effects of six steroids in the treatment of atopic dermatitis in childhood. Pediatr Dermatol. 1984;1(3):246-53.
25. Haeck IM, Rouwen TJ, Timmer-de Mik L, de Bruin-Weller MS, Bruijnzeel-Koomen CA, et al. Topical costicosteroids in atopic dermatitis and risk of glaucoma and cataracts. J Am Acad Dermatol. 2011;64(2):275-81.
26. Grimalt R, Mengeaud V, Cambazard F; Study Investigators' Group. The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: a randomized controlled study. Dermatology. 2007;214(1):61-7.
27. Harcharik S, Emer J. Steroid-sparing properties of emollients in dermatology. Skin Therapy Lett. 2014;19(1):5-10.
28. Nisbet SJ, Dykes P. Twelve-hour skin hydration after a single application of a lamelar moisturizer. J Cosmet Sci. 2015;66(5):305-6.
29. Giam YC, Hebert AA, Dizon MV, Bever HV, Tiongco-Recto M, Kim KH, et al. A review on the role of moisturizers for atopic dermatitis. Asia Pac Allergy. 2016;6(2):120-8.
30. Norrlid H, Hjalte F, Lundqvist A, Svensson Å, Tennvall GR. Cost-effetiveness of maintenance treatment with a barrier-strengthening moisturizing cream in patients with atopic dermatitis in Finland, Norway and Sweden. Acta Derm Venereol. 2016;96(2):173-6.
31. Correa MCM, Nebus J. Management of patients with atopic dermatitis: the role of emollient therapy. Dermal Res Pract. 2012;2012:836931.
32. Varothai S, Nitayavardhana S, Kulthanan K. Moisturizers for patients with atopic dermatitis. Asian Pac J Allergy Immunol. 2013;31(2):91-8.
33. Lindh JD, Bradley M. Clinical effectiveness of moisturizers in atopic dermatitis and related disorders: a systematic review. Am J Clin Dermatol. 2015;16(5):341-59.
34. Leite e Silva VR, Schulman MA, Ferelli C, Gimenis JM, Ruas GW, Baby AR, et al. Hydrating effects of moisturizer active compounds incorporated into hydrogels: in vivo assessment and comparison between devices. J Cosmet Dermatol. 2009;8(1):32-9.
35. Yamada K, Yamashita J, Todo H, Miyamoto K, Hashimoto S, Tokudome Y, et al. Preparation and evaluation of liquid-crystal formulations with skin-permeation-enhancing abilities for entrapped drugs. J Oleo Sci. 2011;60(1):31-40.
This study was carried out at the Complexo Hospitalar Padre Bento de Guarulhos – Guarulhos (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}