


Ada Regina Trindade de Almeida1; Gabriel Ângelo de Araújo Sampaio2; Natássia Pinheiro Lavor Queiroz3
Noninvasive techniques for facial rejuvenation have grown exponentially in recent years. The greater understanding of the anatomical changes involved in the aging process was followed by a rapid evolution in the approach of these alterations and a great development of substances and technologies used for this purpose.
Volume replacement, particularly with hyaluronic acid, has been standing out due to its widespread availability and ease of use, immediate and long-lasting results, reversibility, and safety when properly used.
The objective of this sequel article is to offer a review of the literature and an update on the use of hyaluronic acid cutaneous fillers in the rejuvenation of the temporal and supraorbital regions.
Keywords: DERMAL FILLERS; HYALURONIC ACID; REJUVENATION
As already discussed in part 1 of this article, rejuvenation techniques using hyaluronic acid (HA) for the upper third of the face require that the physician has a deep anatomical knowledge (including soft tissues as well as bone and neurovascular structures) and an understanding of the innate or acquired facial volume deficiencies and the properties and characteristics of available products.1 In this second part, we will discuss the temporal and supraorbital regions included in the upper third of the face.
1. TEMPORAL REGION
A young face shows a subtle transition among the different regions and good coverage on bone prominences—especially on the temples, which should be flat or slightly concave in women, whereas local convexity provides the physiognomy with a more masculine appearance. Volume loss in this region is an early sign of aging; however, it may also occur in young adults who have a low body fat rate.2,3Volume replacement in the temples replaces the local concavity for the young face’s convexity; provides sustenance to the external portion of the eyes and lateral eyebrow elevation; and attenuates periorbital wrinkles.4
1.a Temporal region anatomy
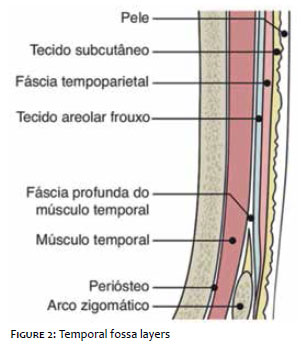
Temporal fossae are bilateral, shallow depressions of the skullcap that are delimited, for didactic purposes, as follows: upper limit, temporal line; anterior, lateral wall of the orbit; inferior, zygomatic arch; and posterior, implantation area of the scalp, where the skin is thicker and more vascularized (Figure 1).5-8 In the last years, several articles describing the anatomy of the temples for the use of fillers were published.3,6,7,9 Among them, the work by Sykes et al. stands out; it identifies, from the temporal fossa’s surface and towards its depth, six structural levels: skin (layer 1); subcutaneous cellular tissue (layer 2); superficial fascia, also referred to as temporofacial fascia (layer 3); loose areolar tissue (layer 4); deep temporal fascia (layer 5); and temporal muscle (layer 6).7
The temporoparietal fascia — or superficial temporal fascia — lies directly under the subcutaneous fat of the temporal region and represents the cephalic extension of the SMAS (superficial musculoaponeurotic system), which begins above the zygomatic arch and goes along the cranial aponeurosis of the forehead and scalp.5
The loose areolar tissue has thickening areas, forming two fibrous septa: one superior (coinciding with the temporal upper line) and one inferior, which divides the temporal region into upper and lower compartments. Near the end of the eyebrow, these two septa merge.6
The deep temporal fascia, known as temporal muscle fascia, covers this muscle and runs as one superiorly just to divide into two (intermediate and deep) at the lower temporal compartment, about 2-3 cm from the zygomatic arch. This division occurs to encompass a temporal fat compartment that is contiguous to the malar fat, located below the orbicularis oculi muscle (Soof — sub-orbicularis oculi fat). For this reason, instead of superficial temple compartment, some authors suggest calling this compartment “suprazygomatic fat of the temple,” as opposed to another deeper one that is contiguous to the oral fat and that could be called “deep or retrozygomatic fat of the temple”.6
The temporal muscle is fan-shaped, thinner at the upper portion, and inferiorly thicker and fibrous. It is firmly anchored in the temporal bone, from which it can execute its masticatory function of elevating and retracting the mandible.6,10 The layers forming the temporal fossa are illustrated in Figure 2. The blood vessels irrigating the temporal fossa are all branches of the external carotid and are located in three planes: superficial vessels (superficial temporal artery and veins) at the subcutaneous plane above the temporoparietal fascia; middle temporal vessels below this fascia and above the superficial temporal fascia layer; and deep vessels located below the temporal muscle and above the deep temporal fascia layer.3 A recent study conducted by Korean anatomists suggests that site showing the lowest risk of vascular lesion in the temple when administering a supraperiosteal injection would correspond to an area of the width of a finger above of the zygomatic arch.11
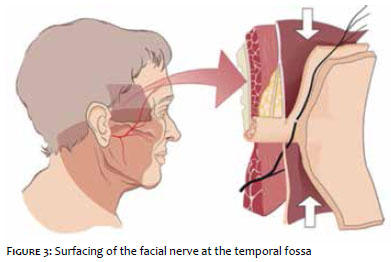
In the temple, the temporal branch of the facial nerve deeply emerges (at the deep temporal fascia), then surfaces above the middle portion of the zygoma to sit below the temporoparietal fascia or inside the SMAS (Figure 3). This nerve innervates the orbicularis, corrugator, and frontalis muscles of the corresponding side.
1.b Temporal aging
Facial changes due to aging occur both at soft tissues and bones. In the temporal region, fat compartments lose volume, the muscle is atrophied and thinned, and the bone retracts and becomes even more concave. All these changes gradually evidence the bone prominences of the zygomatic arch and temporal line until the appearance becomes skeletal and aged.3,9,12
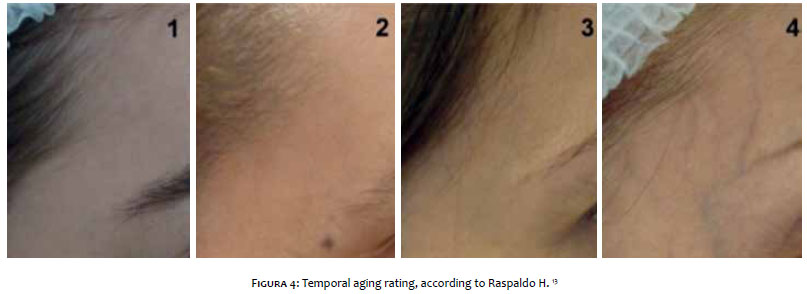
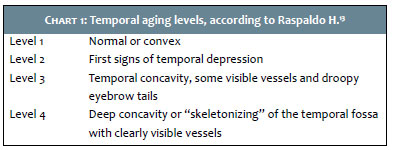
Raspaldo rated the temporal aging in four stages (Figure 4) : In stage 1. the temporal fossa shows no volume changes and is linear or convex. In stage 2, the first aging signs can be perceived, with a slight depression. In stage 3, the temporal fossa concavity is evidenced, with some vessels becoming visible and the eyebrows drooping. In stage 4, major “skeletonizing” and concavity of the temporal fossa are observed, making bones, veins and arteries clearly visible (Chart 1).13
1.c Correction techniques
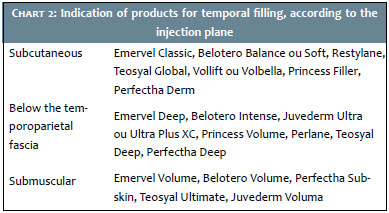
The temporal region can be safely filled in three planes: subcutaneous (superficial to the temporoparietal fascia), loose areolar tissue (between the superficial and deep temporal fasciae) and submuscular (at the periosteum).3,5,7
The selection of both the depth to deposit the filler and the product to be used will depend on the patient’s need and the physician’s preference and experience (Chart 2).
Overall, replacing volume near the temporal merging line reduces the skeletal appearance, while filling near the hairline makes the facial contour recover the “oval” shape considered attractive in women and lose the “peanut” shape acquired with aging.2,14
The injection can be in bolus, pillars, linear, fanning, retrograde, or anterograde. In superficial layers, the fanning technique and the use of more fluid and less thick HA are preferable, and, below the temporal muscle, “Depot or Bolus Technique” and products containing HA with high G’ and high cohesiveness are used. Both techniques should be preceded by aspiration prior to injection (to minimize the risk of intravascular injection) and followed by uniform massage.2
Needle or cannula gauges vary depending on the viscosity and cohesiveness of the selected hyaluronic acid and, again, the physician’s preference. In general, deep filling techniques are performed with needles and the superficial filling ones, with cannulas.
In the literature, variations in temporal volume replacement are found, as detailed below:
1.c.1. Deep filling
Raspaldo13
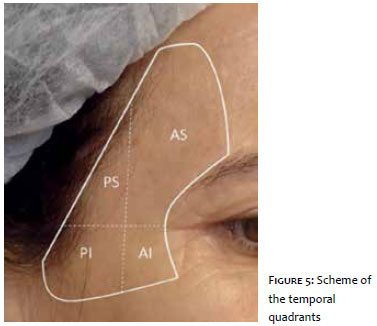
In the technique described by Raspaldo,13 27G needles are used to inject the product in the form of bolus under the deep temporal fascia with the purpose of providing higher projection and more volume and avoiding the facial nerve. For such, he suggests dividing the temporal region in quadrants (anteroinferior and superior and posterior-inferior and superior) from the crossing of two imaginary lines: one vertical at the zygomatic arch midpoint and one horizontal from the outer corner of the eye to the hairline (Figure 5). Injection should start with the anteroinferior quadrant, followed by the anterosuperior quadrant, then the posterior quadrants, in case of severe depression. He also suggests that the volume to be injected varies according to the temporal aging stage: In stage 1. no treatment is needed; in stage 2, 0.4-1.0 ml of hyaluronic acid/side is replaced; in stage 3, the volume reaches 2 ml; and in stage 4, it may reach 4 ml. following injection, gentle massages help shape the product.
One up/One over (Arthur Swift15)
A single-puncture injection using a 27G needle vertically positioned, 1 cm above the temporal merging line and 1 cm laterally, parallel to the supraorbital ridge. Digital pressure to detect arterial pulse, previous aspiration of venous reflux, and to maintain the needle tip at the bone surface ensures a safe plan for the filler’s deposit. This site—close to the temporal crest, where the muscle is less thick—is relatively avascular. The use of highly cohesive, viscous HA in this deep plane and single injection will cause circumferential dispersion towards the zygomatic arch (Canopy Effect). The index finger of the nondominant hand should be positioned behind the injection site to avoid the product to disperse in the area close to the scalp. This technique tends to be more economical, as it typically uses 0.25-0.75 ml of HA per temple. The author does not recommend deep deposits with the needle above the zygomatic arch due to the presence of branches of the second portion of the internal maxillary artery, of which embolization could result in ipsilateral palate necrosis.15
Three-point approach (Marmur16)
A three-point temporal filling technique, with HA being diluted in variable quantities — from 0.2-0.4 ml — of saline solution or lidocaine with epinephrine and 25-30G needles. The first selected point is located at the central portion of the temporal fossa, usually at 1.5-2 cm from the lateral corner of the eye. Once the palpation with the fingers puts local pulsation away, deeply inject 0.1-0.4 ml of the diluted HA. The second point is superior and posterior to the first, and it is only indicated to complement irregularities and depressions, when needed. The third point is located at the lateral forehead close to the temporal merging line, promoting the temple’s gradual transition to the forehead and eyebrow elevation.
Breithaupt3
Breithaupt uses a 27G or 30G needle and delimits an optimal injection window, in which the administration would be safer if placed juxtaperiosteally. He suggests beginning by palpating and drawing the superficial temporal artery in order to avoiding it. The window begins at the eyebrow tail, at the junction with the temporal merging line (superomedial limit). The injections should be administered below and posterior to this line, 1.5 cm or the width of a finger above the zygomatic arch, and in front of the temple’s hairline. The injection should be perpendicular to the bone, with previous aspiration being also suggested.
1c.2. Superficial filling
Moradi6,17
Moradi and colleagues prefer to use hyaluronic acid more superficially, at the subcutaneous or immediately below the temporoparietal fascia. With a 30G needle, the authors penetrate the skin at 90° up to the dermis, then place it at a 45° angle to inject the product. They inject volumes of 0.05-0.1 ml/injection site and make a fan-like dispersion (Fanning technique). These authors also use careful local massage following product injection.
Recently, however, a histopathologic study of corpses evidenced the presence of HA-based fillers at deeper planes (temporal fascia and temporal muscle), even when a superficial plane of filling had been adopted.18
Considering the risk of vascular injuries at intermediary planes, in order to ensure a safe injection, the use of cannulas for more superficial injections is recommended. The favorite ones are 25-27G. The entry hole is made with a larger gauge needle, located below or above the site to correct. The cannula should be introduced at the same angle and direction of the needle used in the entry hole; otherwise, there will be resistance and another puncture may be required. The movements should be perpendicular to the branches of the superficial temporal artery. The filler is deposited in small aliquots, in a retrograde manner, in tunnels spread throughout the region. Next, local gentle massage for molding is performed.5 The post-procedure result is illustrated in Figure 6.
The preferred HAs are more fluid, less viscous, and less concentrated (see Chart 2). Products that are too thick tend to form accumulations, are more difficult to shape in superficial planes, and gives an irregular or undulated appearance to the treated area. Even when using an appropriate material, too superficial or intradermal injection, which could make the filler visible and grey-blueish (Tyndall effect), should be avoided.5
Immediately after each injection, local, gentle compression for about 1-2 minutes are performed to avoid bleedings and ecchymoses. Cold compresses can be applied at the end of the procedure.
2. SUPRAORBITAL REGION
2.a. Normal aspects
The upper lid/eyebrow complex of youngsters is characterized by homogeneous abundance de soft tissues, extending from the orbital ridge to the upper end of the eyebrow hair portion, in a continuous transition to the temporal region.19
The ideal eyebrow position has been related to some anatomical references: it usually begins in the area corresponding to the intersection of a perpendicular line drawn from the alar base of the nose to the inner corner of the eye to the oblique straight-line intersection that begins at the alar base and passes through the lateral corner of the eye. Ideally, the beginning or head of the brow should be positioned at the same height as its tail (in women, the end of the eyebrow may be higher than the beginning), while the medial portion should be thicker, and becomes less dense as it progresses laterally, with its apex projecting over the oblique line that begins at the alar base and passes through the lateral limbus. In women, the peak should be positioned slightly above the orbital arch and in men, it should be at the height of the orbital rim (Figure 7).
2.b. Aging
The supraorbital region is one of the first to show signs of senility. This is easily observed in the photo essay by the photographer, Nicholas Nixon, who annually took pictures of four sisters for 40 years (1974-2004); they were between 15 and 25 years old when he started. The picture taken 10 years after the first one shows that their eyebrows considerably descend, lose the projection seen in the first pictures, and shadows in the forehead and temples become visible.
Loss of skin and soft tissue elasticity, gravitational action, and bone remodeling contribute to brow aging and ptosis. Computerized tomography studies showed that the orbital rim goes through thickening recess or reduction at its superomedial and inferolateral aspects, becoming larger and more inclined.12,20
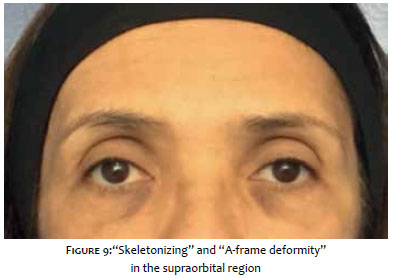
Such changes cause the loss of sustenance of the supraorbital components. The aging process can manifest in two ways: 1) The loss of sustenance promotes ptosis of the supraorbital tissues, cutaneous flaccidity, drooping of brows, and local skin excess (Figure 8); 2) in addition to bone reabsorption, the fat pads disappear and the skin tends to juxtapose the orbital rim, especially at the medial portion, manifesting as an upper central shadow, called "A-frame deformity," in milder cases (Figure 9), and as a deepening and "skeletonizing" of the entire upper orbit, in more severe cases.21,22
2.c. Anatomy of the supraorbital region
In this area, in addition to skin, subcutaneous and epicranial aponeurosis, there is the orbital portion of the orbicularis oculi muscle, and below it there is a fat compartment called Roof (Retro Orbicularis Oculi Fat) and then the periosteum of the orbital rim. It is the Roof that provides the eyebrows with their shape and projection. A volume loss in this compartment causes retreat, projection loss, and drooping of the entire brow in relation to the orbital ridge, as well as an aged appearance of the entire supraorbital region.6
As described in the previous article, in the glabella, the irrigation of the supraorbital region is performed by the supratrochlear arteries (which emerge from the supratrochlear foramen, located between 17 mm and 22 mm from the facial midline, often corresponding to the height of the eye corner) and the supraorbital arteries (which emerge from the supraorbital foramens and leave the orbital rim at the height of the midpupillary line).1 Laterally, the irrigation is performed by the temporal arteries.
2 d. Correction techniques
Some authors noticed improvement of the appearance of the eyes after brow volume replacement. Expanded eyebrows reflect more light; eliminate unwanted shadows; and even increase the height, projection, and balance of the upper third of the face.
Initially, the treatment was performed using autologous fat. In the last years, it has been replaced by hyaluronic acid, which is more promptly available and easier and safer to inject, as it can be dissolved with the use of hyaluronidase in cases of vascular occlusion or unsatisfactory outcomes.
Prior to the procedure, topical anesthesia may be applied with creams that should be left on the site for about 30 minutes. Antisepsis is performed with chlorhexidine 4%.
More viscous HA Fillers are ideal for this region to avoid occlusions and vascular embolisms and for higher firmness of the tissue.
The most generally accepted technique—and used by the authors—is applied by using (25-27G) cannulas.4,14 Preferably, the entry is at the lateral region, at the eyebrow tail. Using the nondominant hand, the brow is elevated, placing it away from the orbital rim. It is kept clamped while the cannula goes in, making the creation of a tunnel easier, through which the filler is injected. The injection plane is below the orbital portion of the orbicularis oculi muscle, into the retro-orbicularis fat (Roof). The filler (Belotero Intense, Juvederm Ultra or Ultra Plus, Restylane Perlane, Vollift, Volbella, Princess Volume, Emervel Deep, or Perfec-tha Deep) should be deposited gradually, in an anterograde and retrograde manner, always above the orbital rim. The push-ahead (anterograde) technique allows the injected material to elevate the region before the needle tip, thereby decreasing the risk of ecchymoses. Subsequently, the cannula is removed and reinserted ahead to complete the filling (Figure 10).
It can also be directed upwards to the peak site of the eyebrow to highlight it. To know where to position it, one should imagine an oblique line linking the nasal ala to the lateral limbus. The upper continuation of this line crosses the brow at its apex. Another way of finding it is by measuring the distance between the eyes (intercanthal distance) and horizontally using this measure in the eyebrow from the inner corner of the eye.10,14 Specific corrections at specific sites can be performed with a 27G needle, for a final finishing, when necessary. Manual modeling of the filler is posteriorly performed to promote symmetry, homogeneity, and anterior projection. Edema on the first two days and local sensitivity are expected effects. Overcorrection should be avoided, as it could lead to an artificial result.
To correct the “A-frame” deformity, previously described, the filler (Belotero Balance or Soft, Volift, Restylane, Princess Filler, Perfectha Derm, or Emervel Touch) should be deposited right below the beginning of the eyebrow. The cannula is horizontally positioned below the brow, using a lateral entry, and the deposit is performed into the retro-orbicularis fat, just above the periosteum, where important vascular bundles emerge from the bone. Small quantities (0.1-0.2 ml/side) are normally enough to obtain natural results.
On the same injection plane, some experienced authors prefer to perform the procedure with thin, short needles (30G, ½). Lambros prefers to inject in three directions at each puncture, distributing the filler to five entries into each eyebrow. The mean injection volume is 0.5 ml per side.6 Liew, in turn, who also uses thin needles, suggests the microdrop technique in a retrograde, slow supraperiosteal injection; for such, he uses three entry holes on average. These two authors complement the procedure with massage and filler molding at the wanted site.21
The product lasts longer in this area (2-4 years) due to the little mobility of the adjacent muscle and the supraperiosteal injection. Anatomical studies of corpses confirmed the clinical findings, by showing that the HA filler that is injected under eyebrows tends to remain at the injected site, retained by the dense fibrous septa existing inside retro-orbicularis fat (Roof).23
It is important to stress that the full periorbital rejuvenation treatment includes approaching the glabella—which projects and positions the beginning of the eyebrows—and the temples, which do the same with the tail. These two techniques were discussed in part I and II of this article.1
3. COMPLICATIONS
Frequently, reactions such as edema, venous congestion, bleeding, and ecchymosis may occur at the injection site, which are usually self-limited, especially in cases where the injection is performed too superficially. Some patients have tenderness at the injection site, which typically lasts only one day, although it may persist for more time during mastication, mainly after intra or submuscular injection.5
Another adverse effect is the presence of local nodules when a more viscous product is injected too superficially.
More serious — and rare — complications found in the literature include: infections (biofilm), granulomatous reactions due to foreign body, cutaneous necrosis, and blindness.3,17
In the temporal region, the superficial temporal artery’s embolization or compression can cause skin damage to the area it irrigates: forehead, eyebrows, upper lateral eyelid portion and lateral scalp portion. The lesion at the temporal branch of the facial nerve, in turn, will cause inability to frown the forehead and elevate the eyebrow.
In a recent literature review, Beleznay and colleagues found five confirmed cases of blindness after temples’ filling — only 1 with HA, 3 with fat and 1 with silicone.24
There are several anastomoses between the superficial temporal arteries (branches of the external carotid) and the supraorbital and supratrochlear arteries (branches of the internal carotid). The proposed mechanism leading to blindness would be the intravascular injection and the filler’s retrograde embolization. If the involved vessels have a small gauge, even a small quantity of HA — if injected rapidly — can overpower the blood pressure and find less proximal resistance, migrating in a retrograde manner. When the applicator stops the injection’s pressure, the blood pressure impels the material to distal retinal arteries, thereby causing occlusion and potential blindness.24
The highest risk, however, lies in the medial-temporal vein, which connects with the cavernous sinus through periorbital veins. Because it is larger than arteries at the same plane, if inadvertently occluded, this vein can lead to embolization of the cavernous sinus, and by retrograde flux, to occlusion of the central retinal artery.3,11,24
If vascular occlusion is noticed through the presence of livedo reticularis, local whitening, or acute pain complaint, the procedure should be immediately interrupted. The site and neighboring area should be inundated with hyaluronidase25,26 (preferably injected with a cannula) and massaged. In cases of retinal vessels, after 90 minutes of occlusion, damages are irreversible. Other measures that could be tried are local heat, massage, oral anticoagulants, and hyperbaric chamber.
The appearance of the temporal fossa and periorbital area have a major impact on facial aging. The use of hyaluronic acid fillers allows recovering local volume and projection, thereby providing a younger, more harmonic look in a natural, safe, and outpatient manner. Patients should be treated in accordance with the local aging stage, and having a good knowledge of the anatomy, injection techniques, and products is essential to obtain good results with minimal complications.
Ada Regina Trindade de Almeida:
Guidance of the coauthors
Review, correction and co-elaboration of all the text topics
Gabriel Ângelo de Araújo Sampaio:
Elaboration and Bibliographical research and review of supraorbital area (eyebrow and upper lid)
Natássia Pinheiro de Lavor Queiroz:
Bibliographical research and review of the temporal region
1. Almeida ART, Sampaio GAA. Ácido hialurônico no rejuvenescimento do terço superior da face: revisão e atualização - Parte 1. Surg Cosmet Dermatol. 2015;8(2):148-53.
2. Buckinghan ED, Glasgold R, Kontis T, Smith SP Jr, Dolev Y, Fitzgerald R, et al. Volume rejuvenation of the facial upperthird. Facial Plast Surg. 2015;31(1):43-54.
3. Breithaupt AD, Jones DH, Braz A, Narins R, Weinkle S. Anatomical basis for safe and effective volumization of the temple. Dermatol Surg. 2015;41Suppl 1:S278-83.
4. Almeida ART, Sampaio GAA. Preenchimentos e técnicas para o terço superior da face. In: Kadunc B, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, Martins S, editores. Tratado de Cirurgia Dermatológica, Cosmiatria e Laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2013. p. 355-60.
5. Almeida ART, Queiroz NPL. Região Temporal. In: Sandoval MHL, Ayres EL editores. Preenchedores: guia prático de técnicas e produtos. São Paulo: AC Farmacêutica; 2013. p.182-189.
6. Sykes JM, Cotofana S, Trevidic P, Solish N, Carruthers J, Carruthers A, et al. Upper face: clinical anatomy and regional approaches with injectable fillers. Plast Reconstr Surg. 2015;136 5 Suppl: S204-18.
7. Sykes JM. Applied anatomy of the temporal region and forehead for injectable fillers. J Drugs Dermatol. 2009;8 Suppl 10:24-27.
8. Tamura BM. Topografia facial das áreas de injeção de preenchedores e seus riscos. Surg Cosmet Dermatol. 2013;5(3):234-8.
9. Sadick NS, Dorizas AS, Krueger N, Nassar AH. The facial adipose system: its role in facial aging and approaches to volume restoration. Dermatol Surg. 2015;41 Suppl 1:S333-9.
10. Swift A, Remignton K. BeautiPHIcationTM a global approach to facial beauty. Clin Plastic Surg. 2011;38(3):347-77.
11. Jung W, Youn KH, Won SY, Park JT, Hu KS, Kim HJ, et al. Clinical implications of the middle temporal vein with regard to temporal fossa augmentation. Dermatol Surg. 2014;40(6):618-23.
12. Wong CH, Mendelson B. Newer understanding of specific anatomic targets in the aging face as applied to injectables: aging changes in the craniofacial skeleton and facial ligaments. Plast Reconstr Surg. 2015;136Suppl 5:S44-8.
13. Raspaldo H. Temporal Rejuvenation with fillers: global face sculpture approach. Dermatol Surg. 2012;38(2):261-5.
14. Goodman GJ, Swift A, Remington BK. Current concepts in the use of voluma, volift, and volbella. Plast Reconstr Surg. 2015;136 Suppl 5:S139-48.
15. Swift A. Dr. Arthur Swift's personal "one up, one over" technique to treat signs of aging in the temple hollows. From "Upper Face: Clinical Anatomy and Regional Approaches with Injectable Fillers". Plast Reconstr Surg [internet]. 2015 Sep 10. 136(5S): [http://journals.lww.com/plasreconsurg/pages/videogallery.aspx?videoId=713&autoPlay=true].
16. Juhász ML, Marmur ES. Temporal fossa defects: techniques for injecting hyaluronic acid filler and complications after hyaluronic acid filler injection. J Cosmet Dermatol. 2015;14(3):254-9.
17. Moradi A, Shirazi A, Perez V. A guide to temporal fossa augmentation with small gel particle hyaluronic acid dermal filler. J Drugs Dermatol. 2011;10(6):673-6.
18. Chundury RV, Weber AC, McBride J, Plesec TP, Perry JD. Micro anatomical Location of Hyaluronic Acid Gel Following Injection of the Temporal Hollows. Ophthal Plast Reconstr Surg. 2015;31(5):418-20.
19. Lam SM, Glasgold R, Glasgold M. Analysisof facial aesthetics as applied to injectables. Plast Reconstr Surg. 2015;13 6Suppl 5:S11-21.
20. Kahn DM, Shaw RB Jr. Aging of the bony orbit: a three-dimensional computed tomographic study. Aesthetic Surg J. 2008;28(3):258-64.
21. Liew S, Nguyen DQ. Nonsurgical volumetric upper periorbital rejuvenation: a plastic surgeon's perspective. Aesthetic Plast Surg. 2011;35(3):319-25.
22. Ayres E, Reis M. Região supraorbitária. In: Sandoval MHL, Ayres EL, editores. Preenchedores: guia prático de técnicas e produtos. São Paulo: AC Farmacêutica; 2013. p.189-194.
23. Griepentrog GJ, Lucarelli MJ. Anatomical position of hyaluronic acid gel following injection to the eyebrows. Ophthal Plast Reconstr Surg. 2013;29(5):35-39.
24. Beleznay K, Carruthers JD, Humphrey S, Jones D. Avoiding and Treating Blindness From Fillers: A Review of the World Literature. Dermatol Surg. 2015;41(10):1097-117.
25. Trindade de Almeida AR. Saliba AF. Hialuronidase na cosmiatria: o que devemos saber? Surg Cosmet Dermatol. 2015;7(3):197-204.
26. Balassiano LKA, Bravo BSF. Hialuronidase: uma necessidade de todo dermatologista que aplica ácido hialurônico injetável. Surg Cosmet Dermatol. 2014;6(4):33843.
Work conducted at the Civil Servant Hospital of the City of São Paulo Dermatologic Clinic - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}