


Rossana Catanhede F. de Vasconcelos1; Karla Leonardi Azuaga2; Renata Trefiglio Eid2; Géssica Cantadori Funes Arenas4
Alopecia areata can cause significant psychological problems due to the unpredictable nature of the disease, which results in hair loss. We report the case of a patient presenting alopecia areata of difficult treatment, with satisfactory response after intralesional applications of corticosteroid, but that showed recurrence and atrophy; it was then decided to perform intralesional applications of platelet-rich plasma, with improvement of the condition. The technique showed good results in this isolated case, proving to be a potentially useful therapy in the treatment of alopecia areata.
Keywords: ALOPECIA AREATA; ADRENAL CORTEX HORMONES; PLATELET-RICH PLASMA
Alopecia Areata (AA) is a chronic inflammatory condition that results in loss of scalp's and/or body hair, affecting up to 2% of the population.1 Several factors have been implicated in its etiopathogenesis.2 The clinical picture is characterized by a single or multiple alopecia plaques, and can involve up to 100% of the scalp's and body hair.2 Diagnosis is clinical, nevertheless dermoscopy and biopsy may be useful as complementary tests. The factors that indicate a worse prognosis are the extension or the ophiasis pattern of the hair loss.
The course of AA is variable. There are many therapeutic options that vary according to the extent of the clinical picture. There are currently two main evidence-based options, which are the glucocorticoids (topical and/or intralesional) and contact immunotherapy.1
The purpose of the use of platelet rich plasma (PRP) is to accelerate tissue regeneration, based on the principle of platelet influence in the processes of hemostasis, inflammation, regeneration and healing, where the production of platelet-derived growth factors (PDGF) takes place, stimulating cell proliferation and differentiation until the repair and total regeneration of the damaged tissue have ended.3
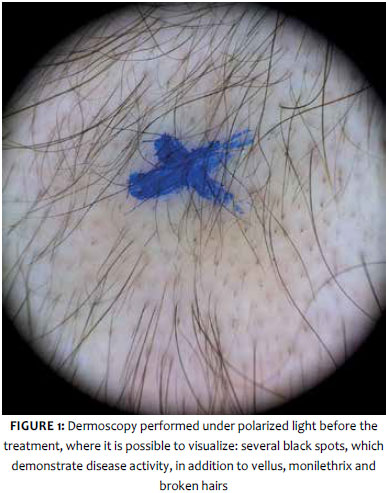
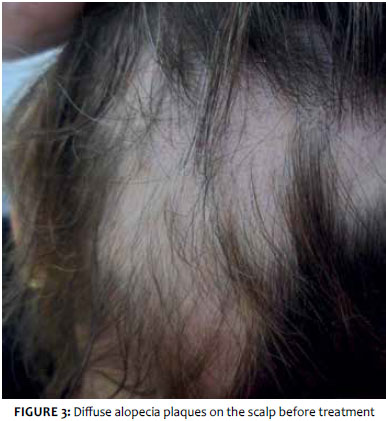
A 43-year-old female patient with a history of hair loss with onset one year before presented diffuse plaques of alopecia on the scalp, clinically characteristic of AA (Figure 1). A number of black spots were observed on the dermoscopy under polarized light, evidencing activity of the disease, as well as vellus hair, monilethrix hair, and broken hair (Figure 2).
Also, the patient had a history of gastric bypass surgery (three years before), and two previous episodes of Alopecia Areata, both treated with intralesional corticosteroids.
The laboratorial tests results showed TSH levels to be at 12.3 and Ferritin at 4. After treatment and normalization of the aforementioned parameters, the use of 5% Minoxidil Topical Solution and 10 mg/ml Intralesional Triamcinolone was started. There was an initial positive response, however recurrence and atrophy were observed after three months. Systemic corticosteroid was then introduced, with absence of response. The condition then coursed with progression of the picture in the scalp and involvement of the eyebrow, when a decision was made for introducing intralesional PRP applications, after the patient signed the a Term of Consent. Three applications were performed with three-week intervals. At each session the patient underwent blood tests performed by a responsible biologist; the PRP was then processed at average concentration of 6.5x as compared to the patient's baseline volume, following the procedures described in the Cantadori Protocol (Reg. 508.102 – Rio de Janeiro National Library), in compliance with all the biosafety and asepsis norms.
Injections were performed by a physician with sterile material and 26 G½ needles. A volume of 0.2ml of PRP was applied in the intradermal plane, at each point of the affected region, observing a 2cm spacing.
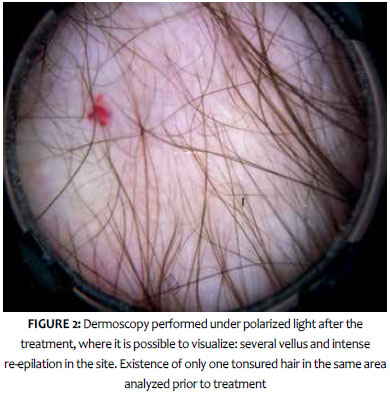
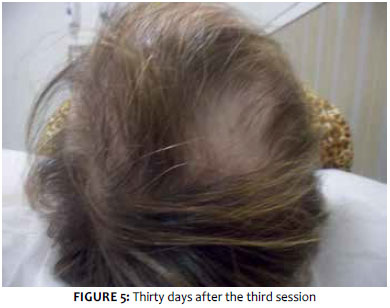
After the first session, important re-epilation could already be observed, with improvement of atrophy (Figure 3). At the end of the three sessions, it was possible to observe re-epilation of the area in the clinical and dermoscopic exams (Figures 4 and 5).
In AA cases, an apparent improvement followed by recurrence can be distressing. One of the most important aspects of the treatment is to advise the patient about the nature of the disease and the limitations of the existing treatments.
Platelet rich plasma is a product derived from laboratory processing of autologous blood, described in the early 1970s by Matras and his team. Currently some areas such as plastic surgery, orthopedics, dentistry, and cardiovascular surgery already use it. In dermatology, PRP has been used with the purpose of promoting the acceleration of wound healing, as an adjuvant in rejuvenation and alopecia treatments, and even after laser sessions.4
In PRP there is an accumulation of growth factors (GF) due to the concentration of platelets (approximately one million per cubic millimeters of blood). These growth factors are known in the literature as PDGF, transforming growth factor-β (TGF-β), transforming growth factor-α (TGF-α), endothelial cell growth factor (ECGF), in addition to adhesive glycoproteins such as fibronectin and thrombospondin, which are important constituents of the provisional extracellular matrix.5 Other GFs are also cited by different authors, such as epidermal growth factor (EGF) and insulin-like growth factor (IGF). Monocytes are activated and transformed into macrophages, whose function is to remove damaged components, performing the biological cleansing in the tissue; in addition to phagocytosis, they also secrete chemotactic factors, which attract other inflammatory cells, produce prostaglandins that function as important biological modulators in the maintenance mechanisms of homeostasis, and potent vasodilators that increase the permeability of microvessels.3 Macrophages still produce many GFs, such as PDGF, TGF-β, FGF and VEGF, which stand out as the major cytokines necessary in the formation of granulation.
Many authors cite GFs as modulators of the inflammatory response, as well as their ability to induce the remodeling and healing process in several types of lesions, presenting no harm to the patient.7
In his thesis on the application of PRP in hair micrograft surgeries, Mates verified the action of GF in hair growth and density, showing abrupt reduction of apoptosis, stimulation of angiogenesis and new and efficient mitoses for the resumption of the new anagen phase.8 Another study also cites a cellular marker for proliferation (Ki-67), which is present in greater amounts in PRP-treated patients. In the studied patient, the authors observed improvement of her condition shortly after the first application. The following could be involved in its mechanism of action: the effect of stimulation on the hair follicle, angiogenesis and the modulatory action of the local inflammatory response. It is also not possible to completely exclude the possibility of spontaneous re-epilation.
In the medical literature, a study of 45 patients with AA demonstrated a significant increase in hair growth in patients treated with PRP, with complete remission in more than half of the cases, and a low rate of recurrence.9 In another study, 20 patients who had been diagnosed with AA were treated with PRP for one year, with only one recurrence and total absence of side effects.10
Despite many studies, the treatment of AA in some cases still poses a great challenge. Alopecia areata can cause significant psychological problems due to its unpredictable nature. In this manner, studies that propose new therapeutic options become relevant.
The PRP infiltration technique was proven a promising method for difficult-to-control cases or for those that appear in important areas of atrophy. In the isolated case studied in the present paper, an apparently effective response was observed, nonetheless further studies are necessary to better evaluate the results and elucidate the mechanisms of action.
1. Garg S, Messenger AG. Alopecia areata: evidence-based treatments. Semin Cutan Med Surg. 2009;28(1):15-8.
2. Alkhalifah A. Alopecia areata update. Dermatol clinics 2013; 31(1): 93-108.
3. Pontual MAB; Magini R. S. Plasma Rico em Plaquetas PRP e fatores de crescimento das pesquisas científicas à Clínica Odontológica. Ed. Santos, SP, 2004
4. Monteiro MR .Plasma rico em plaquetas em dermatologia. Surg Cosmet Dermatol 2013;5(2):155-9.
5. Mendonça RJ, Coutinho-Netto J. Aspectos Celulares da Cicatrização. An Bras Dermatol. 2009; 84 (3): 257-62.
6. Rocha JCT. Terapia Laser, Cicatrização Tecidual e Angiogênese. RBPS 2004;17(1):44-48.
7. Herculano J, Gonçalves JC, Cury VF. Moduladores Biológicos e Fatores de Crescimento na Regeneração Periodontal. PerioNews. 2011; 5(2):151-6.
8. Vasconcelos RCF, Azuaga K, Arenas GCF, Vasconcelos JGF, Borelli NS. A aplicação do plasma rico em plaquetas no tratamento da alopecia androgenética. Surg Cosmet Dermatol 2018;8(2):130-7.
9. Trink A, Sorbellini E, Bezzola P, Rodella L, Rezzani R, Ramot Y, Rinaldi F. A randomized, double-blind, placebo- and active controlled, half head study to evaluate the effects of platelet-rich plasma on alopecia areata. Br J Dermatol. 2013; 169(3): 690-4.
10. 10) Singh S. Role of platelet-rich plasma in chronic alopecia areata: Our centre experience. Indian J Plast Surg. 2015; 48(1): 57- 9.
This study was performed at the Universidade de Santo Amaro (Unisa) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}