


Luiza Soares Guedes Augusto Gomes1; Bruna Sabatovich Villarejo Iosifovich2; Benjamin Solky3; Thiago Jeunon de Souza Vargas4
We report a case of pigmented Bowen's disease in the periungual region treated with Mohs micrographic surgery. Bowen's disease is a squamous cell carcinoma in situ. Although it is a common condition, the pigmented form is rarer, with periungual localization being even more uncommon. Pigmented Bowen's disease presents clinically as a non-uniform, desquamous or verrucous brownish lesion, and it is often confused with other diseases (pigmented actinic keratosis, seborrheic keratosis, melanoma, basal cell carcinoma, nevus). Dermoscopy is of great diagnostic and therapeutic value and is important in the evaluation of recurrence.
Keywords: BOWEN'S DISEASE; CARCINOMA, SQUAMOUS CELL; DERMOSCOPY
Bowen's disease (BD) is a form of Squamous Cell Carcinoma (SCC) in situ originally described by John Bowen in 1912. Bowen's disease is currently considered synonymous with SCC in situ for lesions located in non-anogenital areas.1
The peak incidence of the disease occurs in the seventh decade of life, and most studies show a slight increase of incidence in women.1
The most frequent locations of SCC in situ are the head and neck (photo exposed areas), followed by the lower limbs, in women. The risk of progression of BD into an invasive form of SCC varies between 3% and 5%.1
A 67-year-old male patient, Fitzpatrick's phototype III, reported the appearance of a pigmented and asymptomatic lesion, the size of which was increasing at the base of the nail of the third finger of his right hand.
The patient was found to be immunocompetent, having denied the ingestion of arsenic, trauma, burns or exposure to ionizing radiation at the site of the lesion.
He reported a history of nodular basal cell carcinoma in the supralabial region, SCC in the frontal region and lesion with atypical melanocytic proliferation on the abdominal region.
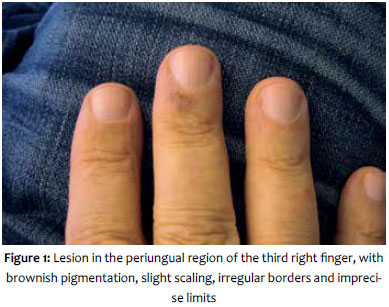
Clinical examination revealed a lesion with brownish pigmentation, with slight desquamation, irregular borders and imprecise limits, located in the distal region of the third finger of the right hand, close to the base of the nail (Figure 1).
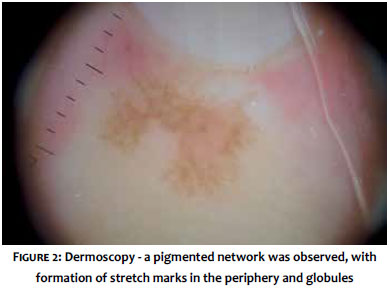
The dermoscopy showed the presence of brownish globules, a pigmented network with formation of stretch marks and some punctiform vessels (Figure 2).
The main diagnostic hypothesis raised by the authors was melanoma.
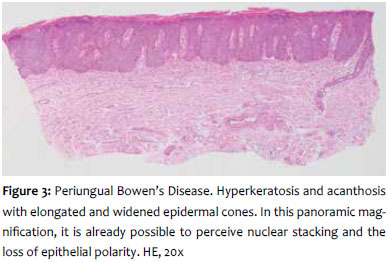
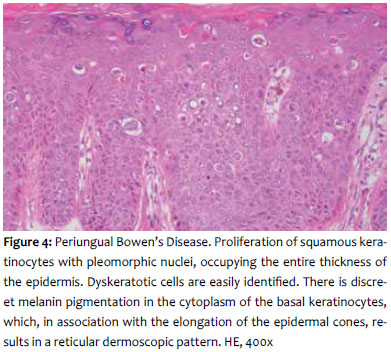
A punch biopsy performed, and the material was sent away for histopathological analysis, which came back with a Pigmented BD diagnosis (Figures 3 and 4).
After confirming the diagnosis, Mohs micrographic surgery was chosen as the course of treatment (Figure 5). Surgery was performed with local anesthetic nerve block. The area of the tumor was removed with minimal margins, positioning the blade at a 45-degree angle. The material was divided into the appropriate number of sections to allow for proper processing, and staining was used to allow for orientation of the material. Tumor free margins were obtained in three steps: in the Step 1, one section was performed; in Step 2, two sections were performed; in Step 3, two sections were performed. The initial lesion size was 7x7mm and the final defect, including the free margins, was 15x9mm. The surgical wound was closed with a graft removed from the right forearm. The nail matrix was fully preserved.
After 18 months of follow-up, the patient did not present a recurrence (Figure 6).
Bowen's disease in the periungual region is uncommon and may assume different aspects, simulating melanoma lesions and affecting the nail plate2 or even resembling chronic paronychia.3, 4
Dermoscopy may aid in the diagnosis of BD, since the findings of glomerular vessels and desquamative surface are present in most cases.2, 5 However, in the pigmented form, findings of globules, pigmented network and striae are also frequent and cause the diagnosis to be confused with that of melanocytic lesions, leaving the final diagnosis for the histological examination. In the histology, the brown globules may correspond to the presence of melanophages and/or to a small increase in the number of pigmented keratinocytes.5
The use of dermoscopy in BD is also recommended for evaluation of recurrence after treatment with photodynamic therapy or imiquimod.6
Regarding Curettage or Shave Biopsy, Punch Biopsy is the most widely recommended, for it will include the entire thickness of the epidermis and dermis in evaluating if the tumor is invasive or not.1
By definition, BD presents in histology the involvement of the entire epidermal layer, characterized by atypical keratinocytes at all levels of the thickened epidermis and also by mitotic figures in the upper layers of the epidermis.5
Regarding therapeutics, there are several options described1 for SCC in situ such as the use of 5-Fluorouracil or Imiquimod, Photodynamic Therapy,7 Radiotherapy, CO2 Laser, Cryotherapy, conventional Surgical Excision and Mohs Surgery.
The best method for the treatment of SCC in situ should be chosen according to the size and location of the lesion, and the clinical condition of the patient.
The periungual region is quite rarely affected, and there are few cases reported in the literature.9 BD at this location represents a therapeutic challenge due to the risk of causing severe functional disability.
In this case, due to the fact that the lesion was a SCC in situ and in the periungual region, the best course of action should take into account the preservation of the motor and sensory function of the finger, yielding the highest probability of cure.
The available treatments were discussed with the patient, thus explaining the risks and benefits of each one of them.
Finally, the authors decided to use Mohs Micrographic Surgery, since this technique, when performed by an experienced surgeon, is capable of yielding high cure rates,9 and gives the patient the chance to have a lower surgical wound if the tumor does not present extensive impairment. On the other hand, if a common surgical excision was performed, a protocol margin of 5mm would be required, which, in the area of the lesion (distal phalanx of the third finger), would present a higher risk of functional and aesthetic alterations of the finger.
In addition to this, the use of a topical treatment, such as Imiquimod or Photodynamic Therapy, was discussed with the patient and discarded in view of the possibility of recurrence and eventual bone involvement in the future, which could lead to amputation of the distal phalanx.10
The periungual location of the Pigmented BD represents a diagnostic and therapeutic challenge, even though it is a SCC in situ.
In the dermoscopy of the Pigmented BD some findings may lead to the suspicion of melanoma, and only histopathological examination can clarify the diagnosis.
There are several therapeutic possibilities, and the choice of the best treatment depends on the evaluation of the risk of recurrence, the possibility of functional and aesthetic sequelae.
1. Morton CA, Birnie AJ, Eedy DJ. British Association of Dermatologist´s guidelines for the management of squamous cell carcinoma in situ (Bowen´s disease) 2014. Br J Dermatol. 2014;170(2):245-60.
2. Haenssle HA, Blum A, Hofmann-Wellenhof R, Kreusch J, Stolz W, Argenziano G, et al. When all you have is a dermoscope - start looking at the nails. Dermatol Pract Concept. 2014;4(4):2
3. Giacomel J, Lallas A, Zalaudek I, Argenziano G. Periungual Bowen Disease mimicking chronic paronychia and diagnosed by dermoscopy. J Am Acad Dermatol. 2014;71(3):e65-7.
4. Fung V, Sainsbury DC, Seukeran DC, Allison KP. Squamous cell carcinoma of the finger masquerading as paronychia. J Plast Reconstr Aesthet Surg. 2010;63(2):e191-2.
5. Zalaudek I, Argenziano G, Leinweber B, Citarella L, Hofmann-Welenhoff, Malvehy J, R et al. Dermoscopy of Bowen´s disease. Br J Dermatol. 2004;150(6):1112-6.
6. Mun JH, Park JM, Song M, Jwa SW, Kim HS, Ko HC, et al. The use of dermatoscopy to monitor therapeutic response of Bowen disease: a dermatoscopic pathological study. Br J Dermatol. 2012;167(6):1382-5.
7. Zink BS, Valente L, Ortiz B, Caldas A, Jeunon T, Marques-da-Costa J. Periungual Bowen's disease successfully treated with photodynamic therapy. Photodiagnosis Photodyn Ther. 2013;10(4):535-7.
8. Pugliano-Mauro M, Goldman G. Mohs surgery is effective for high-risk cutaneous squamous cell carcinoma. Dermatol Surg. 2010;36(10):1544-53.
9. Singh S, Khaitan BK, Sharma MC, Seenu V, Kumawat M, Chatterjee P. Bowen's disease on finger: A diagnostic and therapeutic challenge. Indian J Dermatol Venereol Leprol 2013;79(2):227-230.
10. Gong HS, Cho JH, Roh YH, Chung MS, Baek GH. Bone invasion by squamous cell carcinoma in situ (Bowen's disease) of the finger during treatment with imiquimod 5% cream: case report. J Hand Surg Am. 2010;35(6):999-1002.
This study was performed at the authors' private practices in Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}