


Fernanda Cardoso Bassani1; Sadamitsu Nakandakari2; Gabrielle Aline Zattar3; Cleverson Teixeira Soares4
Subungual squamous cell carcinoma is a rare condition, and its diagnosis is often late. The clinical presentation is atypical and simulates other benign conditions, such as verruca vulgaris, onychomycosis and trauma-induced nail dystrophy. Although it is an unusual entity, we should be attentive to its early diagnosis, considering the biopsy in the chronic nail lesions refractory to treatments. We present five cases of subungual squamous cell carcinoma, in which pain was the most prevalent symptom, and their possible association with trauma and HPV infection should be considered.
Keywords: CARCINOMA, SQUAMOUS CELL; NAILS; NAIL DISEASES
Even though Squamous Cell Carcinoma (SCC) of the nail bed is a rare disease, it is considered the most common subungual malignant tumor.1 Its diagnosis can be difficult and late due to the fact that its clinical presentation is not specific and may mimic several benign inflammatory conditions.2, 3 Diagnosis can be achieved with proper biopsy, and treatment depends on the tumor's extent. The patients were treated at the Nail Clinic of the Instituto Lauro de Souza Lima (ILSL) in Bauru – SP, Brazil.
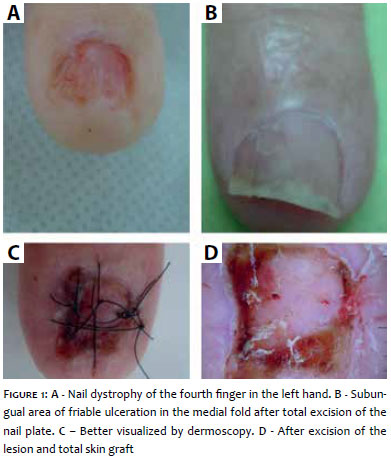
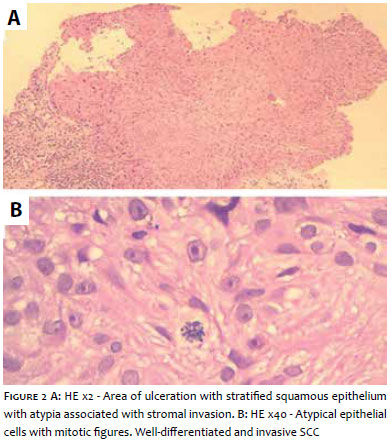
Case 1: A 72-year-old male patient, mechanic by profession, complaining of pain in the nail of the fourth finger of the left hand that started three years before. At the examination, it was possible to observe a discreet nail dystrophy in the medial fold, which was associated with erythronychia of the same region (Figure 1A), exulceration and crusts better demonstrated through dermoscopy of the nail bed (Figure 1B), and presence of subungual friable granulation tissue (Figure 1C). In light of the hypothesis of a glomus tumor, longitudinal fusiform biopsy was performed in the nail bed, evidencing a clearly differentiated and invasive SCC (Figure 2). The radiography was normal. Excision of the whole nail apparatus and local grafting (the donor area of which was the skin of the internal region of the ipsilateral wrist) were performed (Figure 1D). The patient progressed with good healing.
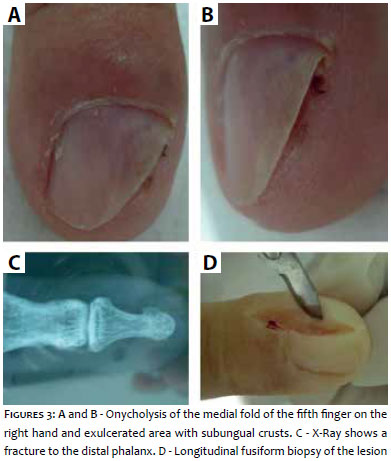
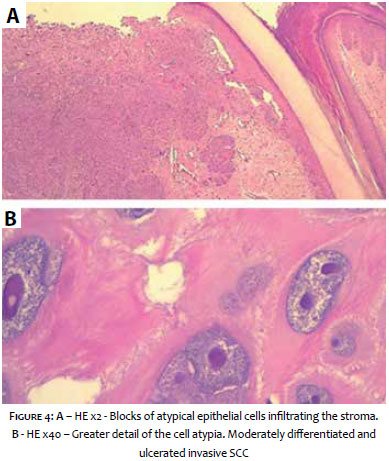
Case 2: A 71-year-old male patient, farmer, diabetic, had been having severe pain for two years in the fifth finger of the right, and sporadic subungual purulent secretion. On examination, onycholysis in the medial fold involving 50% of the plate, and an exulcerated area with subungual crusts could be observed (Figure 3). A lateral longitudinal fusiform biopsy of the nail apparatus was performed evidencing moderately differentiated and ulcerated SCC invasion (Figure 4). The radiography detected a fracture of the distal phalanx of the affected finger. Surgical enlargement of the scar area was performed, which resulted only in local fibrosis. The patient was referred for follow-up with the oncologist.
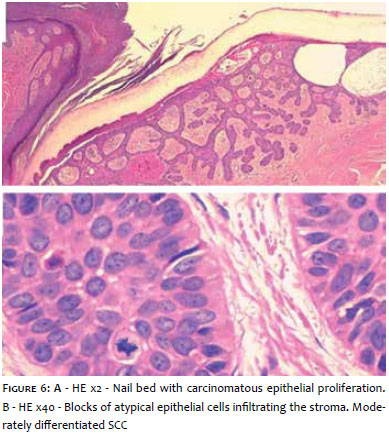
Case 3: A 47-year-old male patient, diagnosed with periungual viral wart in the fourth finger of the right hand, underwent several treatments, such as topical imiquimod therapy and cryotherapy, which yielded unsuccessful results. Upon examination, it was possible to observe onycholysis, exulceration of the medial fold and erythronychia (Figures 5A and B). A longitudinal fusiform biopsy was performed (Figures 5C and D) showing in situ SCC (Figure 6). Lesion exeresis was performed successfully, and the patient was followed up in an outpatient clinic.
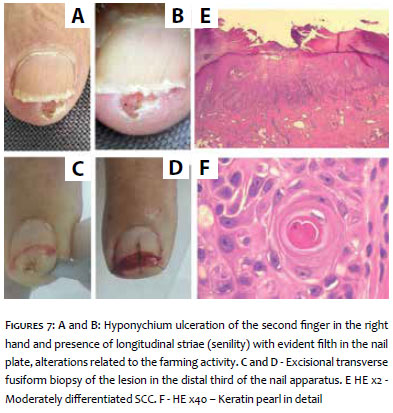
Case 4: A 75-year-old male patient, retired, does gardening for a hobby, had pain when flexing and extending the distal phalanx of the second finger of the right hand. At the examination, it was possible to observe an ulcerated lesion with infiltrated base in hyponychium (Figures 7A and B). A transversal fusiform excisional biopsy was performed in the distal third of the nail apparatus (Figures 7C and D). The results suggested a moderately differentiated SCC, and free margins (Figures 7E and F).
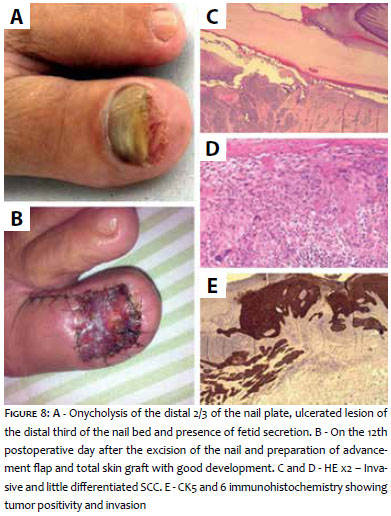
Case 5: A 67-year-old female patient, retired, with history of nail "mycosis" on the left hallux for the previous 12 years; He reported that several antifungal treatments were unsuccessful. Upon examination, it was possible to observe onycholysis of the distal 2/3 of the nail plate, ulcerated lesion of the distal third of the nail bed, and presence of a fetid secretion (Figure 8A). The transversal fusiform biopsy of the ulcerated area of the nail bed showed in situ SCC. The hallux radiography was normal. The proposed treatment was excision of the nail apparatus with implementation of flap and local total skin grafting (Figure 8B). The histological examination of the excised lesion showed a little differentiated invasive SCC (Figures 8C, D and E). The patient progressed with amputation of the distal hallux phalanx and is being followed up.
Although the SCC of the nail bed is rare, it is the most common malignant neoplasm occurring in that body site.1 The diagnosis is often late due to the rarity of the disease and the lack of knowledge among the professionals.2 Affected individuals usually are between 50 and 59 years old.3 Most of the times, it arises as an erythematous, papular, scaly, ulcerated and even vegetative lesion, which can affect the nail bed, lateral folds and distal region of the nail.4 The initial clinical appearance is mistakenly diagnosed with that of a subungual viral wart (as it was in Case 3), pyogenic granuloma, paronychia, keratoacanthoma, traumatic lesions or other benign conditions.2, 3, 5 In general, it is possible to observe longitudinal erythronychia, leukonychia, melanonychia, onycholysis and, in rare cases, pain.2, 3 The data found in the literature contrasts with the findings of the present study, since pain was a symptom present in all patients, with the hypothesis of glomus tumor having been suggested in one case for this reason. Dermoscopy has been an important diagnostic tool in elucidating the etiologies of nail diseases, differentiating lesions of non-melanocytic origin, such as subungual hematoma, bacterial or fungal infections, from melanocytic ones, originating from nevi, racial pigmentation and even melanoma.6 Many patients have severe photodamaged skin on the back of their hands, nevertheless few develop subungual SCC, which strongly suggests that another factor is involved. Subungual SCC is most commonly observed in the fingernails,3-5 and this can be explained by much greater exposure to sunlight and a possible role of the Human Papilloma Virus (HPV).2-4 Human Papilloma Virus infections have been associated with Bowenoid SCC in the hands and subungual region as an important carcinogenic factor.3, 5 The possibility of digital-genital transmission has been suggested.3 In one study, HPV DNA was identified in 80% of patients with subungual SCC. Of these, 60% demonstrated a relationship with HPV Type 16.7, 8 Two of our patients were farmers, meaning that the association with trauma and possible HPV infection could be reported. In the case of the patient who was a mechanic, in addition to the trauma, it is important to investigate the association with frequent exposure to chemical components (greases, oils) as a carcinogenic factor. Subungual SCC appears to have a less aggressive course than it would in other locations.5 Bone invasion is found in approximately 20% of patients.6 Metastases and lymph node involvement are atypical, although they have been reported in some cases.3 Treatment depends on the extent of the tumor.2-4 In the isolated involvement of the nail bed, a wide local excision is indicated, which usually involves a nail fold, matrix, nail bed and the removal of the periosteum5 or, even in cases without bone involvement, Mohs Micrographic Surgery, which allows adequate excision with maximum preservation of normal tissue and function.1, 4 Classical excisional surgery, a technique which was used in the in the studied cases, has led to excellent results in the treatment of lesions without bone involvement, with outcomes similar to those obtained with Mohs surgery, however with a lower degree of complexity.4 Reconstruction with local flap is also indicated for limited and superficial lesions, when necessary.1, 5, 9 For tumors with bone involvement, amputation of the finger is the treatment of choice.1, 3 Radiotherapy may be used in inoperable or extensive cases, and in those with bone involvement or when there is an indication of decrease in the size of the tumor, with a view to performing a surgery later on. Grootenboers et al. showed that with the use of radiotherapy there was local and permanent control of 92% of the patients, with only one case with severe adverse effect leading to digital amputation. Despite the low incidence of metastases, this neoplasm is still generally treated primarily by amputation.10
Subungual SCC may resemble other common clinical conditions affecting the nail apparatus, such as onychomycosis, verruca vulgaris and psoriasis. Lesions that are refractory to treatment or of unusual appearance should be offered consideration in the differential diagnosis with SCC. Therefore, if there is suspicion of this diagnosis, it is recommended that x-ray and biopsy of the nail apparatus, which are easy-to-perform, be carried out, allowing for early diagnosis and effective treatment. Long-term follow-up of patients is also important.
1. Wong TC, Ip FK, Wu WC. Squamous cell carcinoma of the nail bed: Three case reports. J Orthopaedic Surg 2004:12(2):248-52.
2. Baran, R. Bowen's disease and squamous cell carcinoma of the nail unit. J Egypt wom Dermatol Soc. 2005; 2(1):1-8.
3. Dalle S, Depape L, Phan A, Balme B, Ronger-Savle S, Thomas, L. Squamous cell carcinoma of the nail apparatus: clinicopathological study of 35 cases. Br J Dermatol. 2007 156(5):871-4.
4. Pegas, JR, Fernandes, KKML, Prado, IDF, Bazzo, ILMS, Tebcherani, AJ, Cade, KV. Carcinoma espinocelular subungueal: relato de caso e revisão da literatura. Surg Cosmet. Dermatol. 2010; 2 (4) 316-8.
5. Patel PP, Hoppe IC, Bell WR, Lambert WC, Fleegler EJ. Perils of Diagnosis and Detection of Subungual Squamous Cell Carcinoma. Ann Dermatol. 2011; 23(Suppl. 3): s285-7.
6. Yip KM, Lam SL, Shee BW, Shun CT, Yang RS. Subungual squamous cell carcinoma: report of 2 cases. J Formos Med Assoc 2000; 99(8):646-9.
7. Guitart J, Bergfeld WF, Tuthill RJ, Tubbs RR, Zienowicz R, Fleegler EJ. Squamous cell carcinoma of the nail bed: a clinicopathological study of 12 cases. Br J Dermatol. 1990; 123(2):215-22.
8. Zabawski, EJ, Washak RV, Cohen JB, Cockerell CJ, Brown, SM. Squamous Cell Carcinoma of the Nail Bed: Is Finger Predominance Another Clue to Etiology? A Report of 5 Cases. Cutis. 2001;67(1): 59-64.
9. Jules B. Lipoff, AS, Klaus JB, Kishwer SN. Melanonychia Following Mohs Surgery for Recurrent Squamous Cell Carcinoma In Situ of the Nail Bed. J Cutan Med Surg. 2008;12(4): 194-7.
10. Choonhakarn C, Ackerman AB. Keratoacanthomas:a new classification based on morphologic findings and on anatomic site. Dermatopathology: Practical and Conceptual. 2001; 7(1):7-16
This study was performed at the Instituto Lauro de Souza Lima (ILSL), Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}