


Maria Claudia Almeida Issa1; Aline Fassini2; Mariana Boechat2; Ana Carolina Junqueira Ferolla3
Topical photodynamic therapy (TPT) is a well-established therapeutic modality in the treatment of non-melanoma skin cancer. It is based on light-activated chemical reaction in the presence of oxygen. In recent years, this therapy has been used in cosmiatric dermatology, and studies on the mechanisms of TPT action in dermal remodeling of the photodamaged skin have been reported. This review addresses procedures with different light sources and photosensitizers, as well as clinical and collateral effects of this therapy in the treatment of photoaging.
Keywords: PHOTODYNAMIC THERAPY, PHOTOSENSITIZER, PHOTOAGING, REJUVENATION, COLLAGEN, DERMIS
Aging is a complex and multifactorial process that occurs in all individuals, being influenced by environmental, hormonal, and genetic factors. Photoaging, or extrinsic aging, arises from exposure to environmental factors. UV radiation is one of the main factors involved, being responsible for the increase in matrix metalloproteinase (MMPs) on in vivo human skin. MMPs are enzymes responsible for the degradation of protein in the extracellular matrix (ECM), such as collagen type I and III.1-2 Photodamaged skin manifests itself clinically by changes in texture and pigmentation, wrinkles, flaccidity, telangiectasia and, in some cases, actinic keratosis lesions, and non-melanoma skin cancer.1-2, 3
Photodynamic Therapy (PDT) bases itself in a photochemical reaction that causes the selective destruction of a tumor cell. In order for this reaction to take place, a topical photosensitizer placed on the tissue, a light source and oxygen are needed. The main photosensitizers are aminolevulinic-acid (ALA) and methyl aminolevulinate (MAL). MAL is an esterified derivative of ALA, it is more lipophilic and presents greater selectivity to neoplastic cells. The main light source is the Light Emitting Diode (LED), which emits visible blue or red light. The use of MAL - Red Light is recommended for the treatment of deeper lesions, due to the greater skin penetration that the MAL and the red light have on the skin.4-8 PDT with visible light is recommended in the treatment of actinic keratosis (AK), field cancerization and non-melanoma skin cancer (NMSC): Basal Cell Carcinoma (BCC) and Bowen's Disease.9-17
Clinical improvement of the photodamaged skin (texture, pigmentation, wrinkles and flaccidity) after the field cancerization treatment has been described as photodynamic rejuvenation. During a long time, only clinical studies sustained the indication of PDT for photoaging treatment.8-23 It has only been in the last few years that histological and immunohistochemical studies have described the dermal remodeling induced by PDT in the cutaneous rejuvenation.20, 23, 24 Among off-label indications, photorejuvenation is more often reported in cosmetic dermatology, however it is worth to note that PDT is being adopted as a form of treatment for other neoplasias, infectious and inflammatory diseases.25-30
Photoaging
Cutaneous alterations of aging derive from two distinct processes that come together. The natural aging process that occurs in all organs, in a similar way, is either intrinsic or chronological. Photoaging, or extrinsic aging, happens due to the overlapping of environmental factors such as exposure to UV radiation, smoke, wind, and chemical agents. UVA and UVB rays are involved in the pathogenesis of skin cancer and photoaging. UV radiation causes genetic and molecular changes in the epidermal cells and increases the levels of enzymes responsible for the modulation of ECM.1-3 Histologically, cellular atypia is observed, with loss of keratinocyte polarity and accentuated irregularity in cell size.1, 2, 3, 5 On the dermis, histological findings include solar elastosis, thickened and disorganized elastic fibers, and thinly squeezed and flattened collagenous fibers, and increased glycosaminoglycans.1-3
For photoaging treatment, surgical procedures are commonly associated with topical and / or oral clinical treatments. Among the procedures are chemical peels, lasers and lights, botulinum toxin and fillers. Photodynamic therapy has become an excellent choice for the treatment of photodamaged skin with actinic keratosis, not only for inducing rejuvenation, but also mainly for treating pre-malignant subclinical lesions not visible to the naked eye.2, 31-40, 41
Photodynamic Therapy
In order to perform a topical PDT, a photosensitizing agent, a light source and oxygen are needed. Topical photosensitizers are, in fact, prodrugs, which are transformed into protoporphyrin IX (PpIX) inside the cytoplasm and mitochondria, after penetrating the target cell. The photochemical reaction triggered by PDT leads to cell death through the production of singlet oxygen and other reactive oxygen species (ROS).1, 2, 4, 5, 6, 7
The main topical photosensitizers are ALA and MAL. In the United States, 20% ALA (Levulan Kerastick®, DUSA Pharmaceuticals) is presented as a pen containing a solution that is activated at the time of use. It was approved by the FDA in 1999 and associated with blue light for treatment of non-hypertrophic AKs. It is not marketed in Brazil. The time of incubation of ALA in the target tissue ranges from 1 hour to 20 hours, with several protocols described in the literature. Once opened, the product must be fully used and cannot be used in more than one session.1 MAL is widely marketed in several countries around the world, including Brazil, under the name Metvix® (Galderma Pharmaceutical Industry, Paris, France), being approved for AK, BCC and Bowen's Disease. For these indications, the incubation time of MAL is 3 hours, with two sessions with a one-week interval for BCC and Bowen's Disease, and only one session for AK. It is presented as a lipophilic cream, and after it has been opened, it can be kept in refrigerator for up to 1 week. In the photorejuvenation treatment protocol, the incubation time can be reduced to 1 or 2 hours, with two to four sessions, and intervals varying between 2 and 4 weeks.2, 20
Light sources must emit luminous energy in the absorption spectrum of PpIX, which is the target of the treatment. PpIX has maximum light absorption peak at 410 nm, blue light, considered effective because it is very well absorbed by the photosensitizer in the target tissue. On the other hand, this wavelength penetrates superficially, being well indicated for treatment of actinic keratosis, field cancerization. PpIX also absorbs other light lengths, such as red light (630nm), which penetrates more deeply into the skin and is therefore the best choice for the treatment of carcinomas (NMSC). Both are well indicated for treatment of photodamaged skin.2, 31, 32 Other light sources for the treatment of photoaging include Intense Pulsed Light (IPL) and Lasers (PDL). It is worth to noting that although IPL yields good results in the overall appearance of the skin, including pigmentation and texture, it is less effective than LED for the treatment of actinic keratosis in the long term, and are contraindicated for the treatment of carcinomas.2, 31-40
Photodynamic Therapy in the Treatment of Photoaging
The effects of light on the skin involve complex mechanisms. Photoaging is mediated by direct absorption of UV radiation and by indirect mechanisms through ROS-mediated photochemical reactions.2 UV radiation activates AP-1 and NF-Kappa B transcription factors that regulate genes responsible for the production of enzymes that modulate MEC of the dermis, among them MMP-1, MMP-9, MMP-3 and MMP-10. MMP-1 degrades intact collagen, and MMP-9 cleaves the collagen that was previously cleaved by MMP-1. This degradation sequence is critical for repair of the dermis, since the cleavage of the collagen fractions that have a high molecular weight interrupts the synthesis inhibition of new, type I, collagen.42, 43, 44 The activation of AP-1 and NF Kappa is also responsible for increased transcription of cytokines such as IL-1 beta, IL-2, IL-6, IL-10, TNF-alpha and TGF-beta. TGF-beta is involved in dermal remodeling not only by stimulating the synthesis of procollagen (types I and III), but also by inhibiting its degrading enzymes.
The inflammatory response that accompanies PDT-mediated tumor destruction, with release of cytokines and growth factors, is of fundamental importance in the dermal remodeling of the photodamaged skin.45-47 In vitro study for the quantification of MMPs and the expression of mRNA of collagen, showed increased MMP-1 and 3 and reduced expression of type I collagen in culture of fibroblasts (normal skin and scleroderma) treated with ALA and red light.48 The result of this study suggests an antisclerotic effect of PDT in the skin. In contrast, Issa et al23 reported increased MMP-9, without modification of MMP-1 and 3, and increased type I collagen, three and six months after treatment of photodamaged skin with two sessions of PDT (MAL-Red light), respectively. The authors have concluded that the modification of the dermis caused by MMP-9, initially, allowed the modification of the ECM and its relation with the fibroblasts, which consequently produced new collagen, after six months.
Procedure – PDT for Photoaging
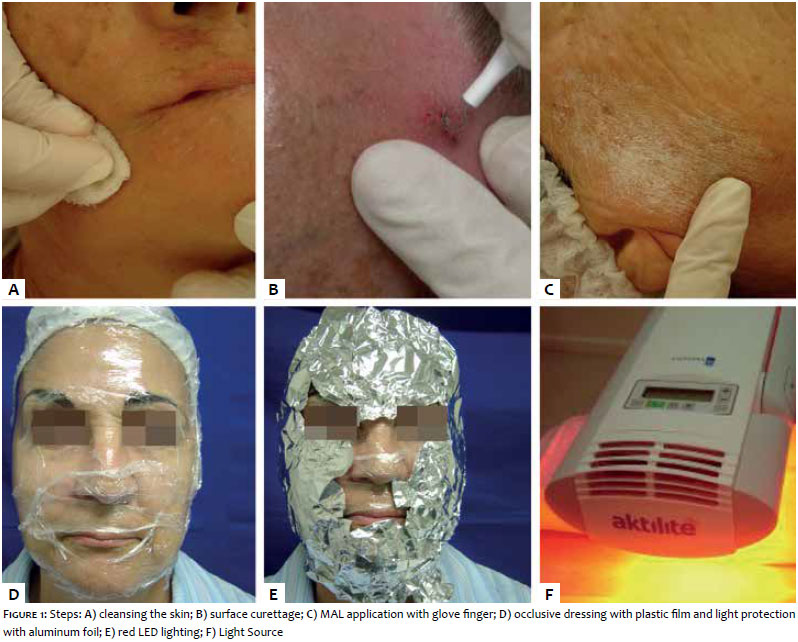
To proceed with of the conventional topic PDT in the treatment of the photodamaged skin we can consider the following steps: 1) Cleaning of the area that will be treated with makeup remover, followed by the application of alcoholic chlorhexidine;
2) Soft skin curettage, prior to the application of the photosensitizer, in order to remove the more superficial layers of the AK lesions; 3) Application of the topic photosensitizer in the entire area that will be treated; 4) Occlusive dressing with a plastic film to increase the penetration of the product, followed by aluminum foil to prevent the activation of PpIX by ambient light during the incubation period of the photosensitizer. For photorejuvenation, the need for occlusion is variable in the literature. The dressing and the excess of the medication are removed with saline solution 0.9% and gauze, before exposure to the light source; 5) Exposure to the light source (Figure 1). Patients and doctor should wear protective eyewear during lighting session. After each session, patients should be instructed to avoid sun exposure for 48 hours, and to use sunscreen after that period.2 Patients should be aware of the benefits and limitations of the technique as well as being made aware of the possible side-effects.
PDT application protocols for photoaging treatment vary widely in the literature. The number of sessions varies on average from two to three, ranging from 15 to 30 days in between each. Generally, a thin layer, half a tube, 1g. per face is used in each session. A thicker layer (5mm) should be applied over the AK lesions isolatedly. The incubation time of the photosensitizer varies from one to three hours, and each light source will have an adequate parameter. In the case of an LED, the required amount of light is predetermined by the lamp, which switches off automatically at the end of the treatment. When the incubation time is greater than one hour or when the patient has many AK lesions, the side effects are more evident. These include pain, especially during exposure to the light source, and in the initial 24 hours following the procedure; edema and erythema. Desquamation begins on the third or fourth day, and between the seventh and tenth days the facial skin is fully recovered (Figure 2). Cold compresses and soothing and healing creams can be used for approximately 7-10 days. Topical corticosteroids are rarely indicated. Dyschromias are rare and, if they occur, usually temporary. Anti-viral prophylaxis should be done in patients with a history of cold sores. Bacterial infection is rare, but sterile pustules are reported after acne treatment.1, 2
Treatment Protocols with Different Light Sources
a. PDT with Intense Pulsed Light (IPL)
Ruiz-Rodriguez et al.40, evaluated 17 patients with different degrees of photodamage and AKs (38 lesions altogether) treated with two sessions of ALA IPL. The ALA incubation time was 4 hours and the interval between sessions was 1 month. Thirty-three of the 38 AK lesions were healed in the three-month follow-up period. The technique was well tolerated, and aesthetic results were excellent in all patients.
Several IPL parameters, in regards to the cut-off filter wavelength, pulse duration, pulse interval and energy density, have been used for photorejuvenation with PDT. Many authors have reported significant improvement of photoaged skin (texture, pigmentation, fine wrinkles and AK) with the combination of ALA and IPL, when compared to the use of IPL alone. MAL is also used with IPL to treat photodamaged skin effectively and safely.
Although both photosensitizers are effective for photorejuvenation with IPL, AK healing should be monitored long term.8, 35, 36, 39
b. PDT with Pulsed Dye Laser (PDL)
Alexiades-Armenakas et al.37, in a study using PDT-PDL (585nm), evaluated 2,561 AK lesions on the face, scalp and extremities. They reported a cure rate of 99.9% on the 10th day, and 90.1% for lesions on the face, on the fourth month. The lesions at the extremities showed a lower percentage of response. PDT with PDL is considered to be an adequate form of treatment for the vascular component of the photodamaged skin, since this component has a lower response to PDT visible light.37, 49
c. PDT with Blue Light
Even though Blue Light penetrates the skin superficially, many studies confirm the efficacy of PDT with Blue Light in the treatment of aging. These studies report improvement not only with AK lesions, but also in texture and pigmentation of the skin.
Palm et al31 who treated 18 photoaging patients with photodynamic therapy using MAL Visible Light, and compared the Blue Light with the Red Light, reported that there was no significant difference between the treatments.
The inflammatory reaction after treatment with ALA-Blue Light is usually more intense than with MAL-Red Light, when the photosensitizers have the same incubation time.
d. PDT with Red Light
Sanclemente et al.32 studied the histopathological changes after treatment with photodynamic therapy in combination with MAL and Red Light, and reported improvement of collagen and elastic tissues, although not statistically significant.
Ferola et al.1 demonstrated the overall clinical improvement of the skin with whitening, AK improvement, fine wrinkles and flaccidity after three sessions of photodynamic therapy with ALA (2 hours) and Red Light (20 min) with a fifteen-day interval in between sessions. The histology, due to picrosirius staining, observed an improvement in the organization of the collagen fibers in the dermis.
Issa MCA1 evaluated the therapeutic response of PDT in the treatment of photodamaged skin in 14 women with and without AKs. Two sessions of MAL-Red Light were performed with a 30-day interval between sessions. Three skin biopsies were performed on the face (pre-treatment, after 3 months and after 6 months). The incubation time of the MAL was of 2 hours under occlusion.
The LED used was Aktilite (Photocure, Oslo, Norway) at the dose of 37mJ /cm2. Clinical results showed improvement in texture, pigmentation and wrinkles after the first session, with progressive improvement after a 3-month and 6-month follow-up. At 6 months, it was observed an improvement in the firmness of the skin, with decrease of sagging, becoming more evident (Figures 3 and 4). The improvement findings were observed for up to a 12-month period. Among the observed side effects there were pain, edema, erythema and desquamation with variable intensity, in most cases of mild to moderate intensity. There were also some cases with greater intensity.
Issa et al.20 studied the histological and morphometric changes in the patients mentioned above, observing a statistically significant increase in collagen by picrosirius staining three months after treatment. This improvement was maintained after 6 months, when it was noted that, due to orcein staining, elastic fibers also increased, becoming thinner and with better histological organization. Issa et al.23 also evaluated, through immunohistochemical studies, the substrates involved in dermal remodeling, such as type I and III collagen, ECM-degrading enzymes involved in photoaging, such as MMPs 1, 3, 7, 9, 12, as well as inhibitors of MMPs such as TIMP 1 and 2. The results found included a statistically significant increase of MMP-9 after 3 months and a statistically significant increase in type I collagen after 6 months.
Le Pillouer-Prost and Cartier,50 in reviewing of the literature, have observed that PDT has a high level of efficacy, improvement of fine wrinkles, tonus, skin roughness, texture and remodeling of the dermis. The best indication is for the patient who had chronic exposure to the sun and has multiple actinic keratoses.
The technique called "photodynamic rejuvenation" has been discussed in the literature since 2002.40 Many authors have described the beneficial clinical effects of this therapy, and studies on the histological and immunohistochemical modifications induced by PDT corroborate the clinical findings in photorejuvenation.2, 20, 23, 24 The protocols vary in the preparation of the skin, in the incubation time and occlusion of the photosensitizer, in the number and break of sessions, and in the light source and its parameters. Regardless of the protocol used, an overall skin rejuvenation is achieved, with improved texture, pigmentation, wrinkles and sagging, in addition to the cure of actinic keratoses. Patients who have suffered chronic exposure to the sun and have photodamaged skin with actinic keratosis are the most indicated for this therapeutic modality.
1. Ferolla ACJ. Estudo da pele humana fotoenvelhecida após tratamento com terapia fotodinâmica associada ao ácido 5 delta aminolevulínico tópico: avaliação imunoistoquímica, do colágeno e do tecido elastic [tese]. São Paulo: Faculdade de Medicina da Universidade de São Paulo; 2007.
2. Issa MCA. Estudo Da Remodelação Dérmica Induzida Pela Terapia Fotodinâmica (MAL-TFD) Na Pele Fotodanificada [tese]. Rio de Janeiro: Universidade Federal do Rio de Janeiro; 2008.
3. Gilchrest BA. Skin aging and photoaging: an overview. J Am Acad Dermatol. 1989; 21:610-3.
4. Issa MCA, Patricia-Azulay M. Terapia Fotodinâmica: revisão da literatura e documentação iconográfica. Anais Bras Dermatol. 2010; 85(4): 501-11.
5. Kalka K, Merk H, Mukhtar H. Photodinamic therapy in dermatology. J. Am. Acad. Dermatol. 2000; 42(3): 389-413.
6. Szeimies RM, Calzavara-Pinton P, Karrer S, Ortel B, Landthaler M. Topical photodynamic therapy in dermatology. J Photochem Photobiol. 1996; 36(2): 213-9.
7. Casas A, Fukuda H, Di Venosa G, Batlle A. Photosensitization and mechanism of cytotoxicity induced by the use of ALA derivatives in photodynamic therapy. Br J Cancer. 2001; 85(2):279-84
8. Nestor MS, Gold MH, Kauvar AN, Taub AF, Geronemus RG, Ritvo EC, et al. The use of photodynamic therapy in dermatology: results of a concensus conference. J Drugs Dermatol. 2006; 5:140-54
9. Hurlimann, AF, Panavizzon, RG, Burg, A. Topical photodynamic treatment of skin tumours and dermatoses. Dermatology 1994; 3(3): 327.
10. Szeimies RM, Morton CA, Sidoroff A, Braathen LR. Photodynamic therapy for non-melanoma skin cancer. Acta Derm Venereal. 2005;85(6):483-90.
11. Szeimies RM, Karrer S, Sauerwald A. Photodynamic therapy with topical application of 5-aminolevulinic acid in the treatment of actinic keratoses: an initial clinical study. Dermatology. 1996; 192(3):246-51.
12. Fink-Puches R, Soyer HP, Hofer A, Kerl H, Wolf P. Long-term follow-up and histological changes of superficial nonmelanoma skin cancers treated with topical-aminolevulinic acid photodynamic therapy. Arch Dermatol. 1998; 134(7):821-6.
13. Szeimies R-M, Sassy T, Landthaler M. Penetration potency of topical applied-aminolevulinc acid for photodynamic therapy of basal cell carcinoma. Photochem Photobiol. 1994; 59(1):73-6.
14. Szeimies RM, Karrer S, Radakovic-Fijan S, Tanew A, Calzavara-Pinton PG, Zane C, et al. Photodynamic therapy using topical methyl 5-aminolevulinate compared with cryotherapy for actinic keratosis: a prospective, randomized study. J Am Acad Dermatol. 2002; 47(2):258-62.
15. Salim A, Leman JA, McColl JH, Chapman R, Morton CA. Randomized comparison of photodynamic therapy with topical 5-fluorouracil in Bowen's disease. Br J Dermatol. 2003;148(3): 539-43.
16. Lee PK, Kloser AJ.Current methods for photodynamic therapy in the US: comparison of MAL/PDT and ALA/PDT. J Drugs Dermatol. 2013 Aug;12(8):925-30
17. Babilas P, Karrer S, Sidoroff A, Landthaler M, Szeimies RM. Photodynamic therapy in dermatology: an update. Photodermatol Photoimmunol Photomed. 2005; 21(3):142-9.
18. Bruscino N, Rossi R, Dindelli M, Ghersetich I, Lotti T. Facial skin rejuvenation in a patient treated with photodynamic therapy for actinic keratosis Dermatol Ther. 2010; 23(1):86-9.
19. Park MY, Sohn S, Lee ES, Kim YC. Photorejuvenation induced by 5-aminolevulinic acid photodynamic therapy in patients with actinic keratosis: a histologic analysis. J Am Acad Dermatol. 2010; 62(1):85-95.
20. Issa MC, Piñeiro-Maceira J, Vieira MT, Olej B, Mandarim-de-Lacerda CA, Luiz RR, et al. Photorejuvenation with Topical Methyl Aminolevulinate and Red Light: A Randomized, Prospective, Clinical, Histopathologic, and Morphometric Study. Dermatol Surg. 2010; 36(1):39-48.
21. Shamban AT. Current and new treatments of photodamaged skin. Facial Plast Surg. 2009;25(5):337-46.
22. Bjerring P, Christiansen K, Troilius A, Bekhor P, de Leeuw J. Skin fluorescence controlled photodynamic photorejuvenation. J Lasers Surg Med. 2009; 41(5): 327-36.
23. Almeida Issa MC, Piñeiro-Maceira J, Farias RE, Pureza M, Raggio Luiz R, Manela-Azulay M. Immunohistochemical expression of matrix metalloproteinases in photodamaged skin by photodynamic therapy. Br J Dermatol. 2009;161(3):647-53.
24. Szeimies RM, Torezan L, Niwa A, Valente N, Unger P, Kohl E, et al. Clinical, histopathogical and immunohistochemical assessment of human skin field cancerization before and after photodynamic therapy. Br J Dermatol. 2012 l;16(1):150-9.
25. Morton CA, Szeimies RM, Sidoroff A, Braathen LR. European guidelines for topical photodynamic therapy part 2: emerging indications: field cancerization, photorejuvenation and inflammatory/infective dermatoses. J Eur Acad Dermatol Venereol. 2013; 27(6):672-9.
26. Alster TS, Tanzi EL. Photodynamic therapy with topical aminolevulinic acid and pulsed dye laser irradiation for sebaceous hyperplasia. J Drugs Dermatol. 2003; 2(5):501-4.
27. Calvazara-Pinton P, Arisi M, Sereni E, Ortel B. A critical reappraisal of off-label indications for topical photodynaic therapy with aminovelunic acid and methylaminolevulinate. Rev Recent Clin Trilas 2010; 5 (2):112-6.
28. Bissonnette R, Tremblay J-F, Juzenas P, Boushira M, Lui H. Systemic photodynamic therapy with aminolevulinc acid induces apoptosis in lesional T lymphocytes of psoriatic plaques. J Invest Dermatol. 2002; 119(1):77-83.
29. Szeimies RM, Landthaler M, Karrer S. Non-oncologic indications for ALA-PDT. J Dermatolog Treat. 2002(b); 13(suppl 1):S13-8.
30. Gold MH, Goldman MP. 5-aminolevulinic acid photodynamic therapy: where we have been and where we are going. Dermatol Surg. 2004; 30(8):1077-84.
31. Palm MD, Goldman MP. Safety and efficacy comparison of blue versus red light sources for photodynamic therapy using methyl aminolevulinate in photodamaged skin. J Drugs Dermatol. 2011; 10 (1):53-60.
32. Sanclemente G, Correa LA, Garcia JJ, Barrera M, Villa JF, Garcia HI. Methyl aminolevulinate plus red light vs. placebo plus red light in the treatment of photodamaged facial skin: histopathological findings. Exp Dermatol. 2012;37(4):379-86.
33. Bjerring P, Clement M, Heickendorff L, Lybecker H, Kiernan M. Dermal collagen production following irradiation by dye laser and broadband ligt source. J Cosmetic laser Ther. 2002;4(2):39-43.
34. Karrer S, Bäumler W, Abels C, Hohenleutner U, Landthaler M, Szeimies R-M. Long-pulse dye laser for photodynamic therapy: investigations in vitro and in vivo. Lasers Surg Med.1999; 25(1):51-9.
35. Dover JS, Bhatia AC, Stewart B, Arndt KA. Topical 5-aminolevulinic acid combined with intense pulsed light in the treatment of photoaging. Arch Dermatol. 2005; 141(10):1247-52.
36. Alster TS, Tanzi EL, Welsh EC. Photorejuvenation of facial skin with topical 20% 5-aminolevulinic acid and intense pulsed light treatment: a split-face comparison study. J Drugs Dermatol. 2005; 4(1):35-8.
37. Alexiades-Armenakias MR, Gernemus RG. Laser-mediated photodynamic therapy of actinic keratosis. Arch Dermatol. 2003;139(10):1313-20.
38. Gold MH, Bradshow VL, Boring MM, Bridges TM, Biron JA. Split face comparison of photodynamic therapy with 5-aminolevulinic acid and inense intense intense pulsed light versus intense pulsed light versus intense pulsed light alone for photodadage. Dermatol Surg. 2006;32(6):795-801.
39. Mamur ES, Phelps r, Goldberg DJ. Ultraestructural changes seen after ALA – IPL photorejuvenescimention: a pilot study. J Cosmetic Laser Ther. 2005;7(1):21-4.
40. Ruiz-Rodriguez R, Sanz-Sanchez T, Cordoba S. Photodynamic photorejuvenation. Dermatol Surg. 2002 A;28(8):742-44; discussion 744.
41. Touma DJ, Gilchrest BA. Topical photodynamic therapy: a new tool in cosmetic dermatologic. Semin Cutan Med Surg. 2003;22(2):124-30.
42. Fisher GJ, Kang S, Varani J, Bata-Csorgo Z, Wan Y, Datta S, et al. Mechanisms of photoaging and chronological skin aging. Arch Dermatol. 2002;138(11):1462-70.
43. Kang S, Fisher GJ, Voorhees JJ. Photoaging: pathogenesis, prevention, and treatment. Clin Geriatr Med. 2001; 17(4): 643-659, v-vi.
44. Chung JH, Seo JY, Choi HR, Lee MK, Youn CS, Rhie G, et al. Modulation of skin collagen metabolism in aged and photoaged human skin in vivo. J Invest Dermatol. 2001; 117(5): 1218-1224.
45. Naderi-Hachtroudi L, Peters T, Brenneisen P, Meewes C, Hommel C, Razi-Wolf Z, et al. Induction of manganese superoxide dismutase in human dermal fibroblasts: a UV-B-mediated paracrine mechanism with the release of epidermal interleukin 1 alpha, interleukin 1 beta, and tumor necrosis factor alpha. Arch Dermatol. 2002; 138(11): 1473-1479.
46. Dougherty TJ, Gomer CJ, Henderson BW, Jori G, Kessel D, Korbelik M, et al. Photodynamic therapy. J Natl Cancer Inst. 1998 Jun 17; 90(12):889-905.
47. Brenneisen P, Sies H, Scharffetter-Kochanek K. Ultraviolet-B irradiation and matrix metalloproteinases: from induction via signaling to initial events. Ann N Y Acad Sci. 2002; 973:31-43.
48. Karrer S, Bosserhoff AK, Weiderer P, Landthaler M, Szeimies RM. Influence of 5-aminolevulinic acid and red light on collagen metabolism of human dermal fibroblasts. J Invest Dermatol. 2003 Feb; 120(2): 325-31.
49. Friedmann DP, Goldman MP, Fabi SG, et al. Multiple sequencial light and laser sources to activate aminolevulinic acid in photodamage: A retrospective study. Cosmet Laser Ther. 2015; 17(5): 252-8
50. Le Pilloer-Prost A; Cartier H Photodynaimic Photorejuvenation: A Review. Dermatol Surg 2016;42(1): 21-30.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}