


Marcela da Costa Pereira Cestari1; Andrea Penhalber Frange1; Bianca Pinheiro Bousquet Muylaert1; Anna Rita Ferrante Mitidieri de Oliveira1; Eduarda Braga Esteves1; Nátalie Schnaider Borelli1; Douglas Haddad Filho2
The nevus sebaceous of Jadassohn is a congenital benign hamartoma of the skin that occurs more frequently in the scalp, but can also arise in the face. Due to its potential for malignization, exeresis is often required. Lesions located in the scalp are challenging to surgeons because of the anatomical characteristics of this body site, namely scarcity and inelasticity of the adjacent skin. In the present report, the authors describe a case of excision of a nevus sebaceous of Jadassohn located in the scalp, using a bilateral rotation flap – a very straightforward and versatile technique, excellent for reconstructing difficult topographies such as the scalp – for the closure of the surgical wound.
Keywords: AMBULATORY SURGICAL PROCEDURES; NEVUS, SEBACEOUS OF JADASSOHN; SURGICAL FLAPS
The sebaceous nevus of Jadassohn (SNJ) or organoid nevus is a congenital benign hamartoma of the skin, characterized by hyperplasia of the epidermis, degenerated hair follicles, sebaceous and ectopic apocrine glands. It occurs in approximately 0.3% of the individuals, with no gender prevalence. The lesion in general is present at birth and arises as a well-defined plaque composed of multiple confluent orangish-yellow or brownish-yellow colored papules, predominantly located on the scalp, where it courses with alopecia at the lesion's site.
Its surface becomes thickened and verrucous during puberty due to hormonal stimulation of the eccrine and apocrine components, with the possibility of the lesion becoming nodular in adulthood, with the occurrence of ulcerations and crusts. The probability of secondary neoplasms to emerge in this stage (mainly basal cell carcinoma, papillary syringocystadenoma and trichoblastoma) is of 10% to 30%. In a possible malignant transformation or in cases with presence of ulceration, surgical excision can be required. Large lesions located in the scalp are usually difficult to reconstruct due to local anatomical features. 1.2
The cephalic segment's lining can be classified into soft parts and osseous tissues. The soft parts are responsible for covering and protecting the osseous structure, being sub-classified into skin, subcutaneous tissue, galea, loose areolar tissue and pericranium. The subcutaneous tissue is formed by dense connective tissue, fat and several fibrous septa resulting in inelastic structures. The main arteries and veins responsible for the region's irrigation and venous drainage are located in this layer. Among the most important are the superficial temporal, supraorbital, supratrochlear, posterior auricular and occipital vessels. This vast vascular network allows the use of various types of flaps, with considerable safety. The loose areolar tissue – or subaponeurotic tissue – is located between the galea and the pericranium. Its structural characteristics facilitate the surgical access and the elevation of the flaps, constituting a plane of easy dissection. It also has small arteries supplying the pericranium, and small emissary veins, which connect the intracranial venous sinuses with the superficial venous system. 3
Reconstruction of surgical wounds on the scalp can be performed with the assistance of simple sutures, flaps and grafts, with the latter being used in very particular cases due to the difficulty of obtaining similar donor areas. Direct sutures are not always viable due to the scarcity of adjacent skin in the scalp, as well as its inelasticity. In this way, wounds with diameter greater than 3cm usually require reconstructions based rotation, advancement or transposition flaps. 3,4
A 57-year-old male patient, originary from the Brazilian Southeast city of São Paulo sought assistance complaining of a lesion in the scalp, which had arisen in childhood and changed appearance in adulthood.
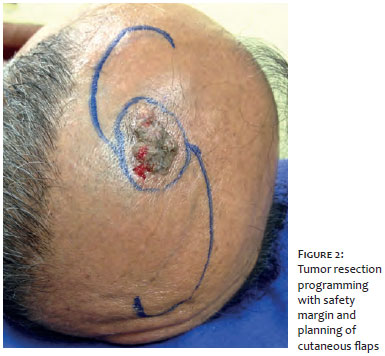
The dermatological examination showed a normochromic verrucous plaque with brownish and friable areas measuring 3.6 cm on their longest axis, in the left parietal region of the scalp (Figure 1). An incisional biopsy was performed with histological analysis, confirming the diagnosis of SNJ. Due to the patient's complaint and malignization risk, a decision was made for the exeresis of the lesion.
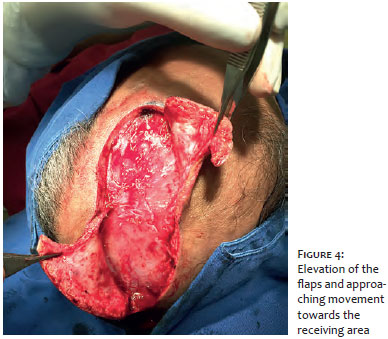
The patient underwent circular resection of the tumor, with a safety margin of 5mm (Figure 2), up until the galeal plane, followed by the reconstruction with the rotation of bilateral circular skin flaps, also prepared up until the galeal plane, based on branches of the occipital and superficial temporal vessels (Figures 3 and 4). The flaps were rotated towards the medial direction, and the suture was carried out with simple stitches and nylon 4.0 (Figure 5). The surgical specimen was sent for pathological examination, which verified free margins and absence of neoplasms.
The patient had good postoperative development, with excellent healing and final aesthetic outcome (Figure 6).
Sebaceous nevus of Jadassohn occurs in approximately 0.3% of individuals, usually at birth, being more commonly located on the scalp. In adulthood, it may be associated with several tumors, most commonly with basal cell carcinoma, papillary syringocystadenoma, and trichoblastoma. Although initially arising as a benign lesion, surgical excision is indicated in most cases due to the risk of malignization, which increases over the years. Lesions located on the scalp can be difficult to approach due to the region's anatomical characteristics. 1, 2
The scalp has little tissular expandability, which hampers the primary suture in larger lesions, very frequently entailing the necessity of more extensive undermining of tissues, which in turn leads to an inadequate tense approach of the borders, resulting in widened scars and / or alopecia 3, 4
The alternative applied in such cases is the use of scalp skin flaps. The planning possibilities and options for these flaps are very diverse, given the extensive vascular network of the segment.
The scalp's irrigation network comprises – bilaterally – the supratrochlear, supraorbital, superficial temporal, occipital and posterior auricular vessels, forming a very extensive vascular network, mainly in the central region, where the branches of these major vessels anastomose, 4 allowing large rotation arches for arterial flaps, as well as cutaneous transpositions in other aesthetic units (for instance the Washio flap for the reconstruction of facial regions). 4, 5
With this rich vascularity, the flap options for closure of tumor resections can be considerably varied: from small skin flaps to large reconstructions that require cutaneous expansions and microsurgical flaps.
Among the various possibilities for the use of scalp flaps, the rotation flap is a very safe and easy to implement option. In general, the reconstruction begins with the rotation of a unilateral flap and primary closure of the donor area. In cases where the unilateral rotation is not sufficient, it is possible to use another contralateral flap, similar in size and shape, in the same surgical time, demonstrating the great versatility of this proposal for rotation flaps.
1. Quadros JM, Marques AS. Aspectos evolutivos do nevo sebáceo de Jadassohn. An Bras Dermatol. 1982;57(2):109-115.
2. Moody MN, Landau JM, Goldberg LH. Nevus sebaceous revisited. Pediatr Dermatol. 2012;29(1):15-23.
3. Leedy JE, Janis JE, Rohrich RJ. Reconstruction of acquired scalp defects: an algorithmic approach. Plast Reconstr Surg. 2005;116(4):54e-72e.
4. Washio H. Retroauricular-temporal flap. Plast Reconstr Surg. 1969;43(2):162-66 .
5. Washio H. Further experience with the retroauricular temporal flap. Plast Reconstr Surg. 1972;50(2):160-62.
This study was performed at the Faculdade de Medicina da Universidade de Santo Amaro (Unisa) – São Paulo(SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}