


Cibele Conceição dos Apóstolos Pereira1; Vando Barbosa de Sousa1; Solange Cardoso Maciel Costa Silva2; Candida Naira Lima e Lima Santana3; Mario Chaves Loureiro do Carmo4; Paula Renaux Wanderley Caratta Macedo5
The skin flaps are surgical techniques particularly useful to aesthetic repair in cases of extended excision and/or unusual sites, as in the ear. Many skin flaps options were already reported, resulting in variable results of the theoretical knowledge and practical experience of the surgeon. This article aims to describe two successful cases of ear reconstruction with the use of anterior and posterior flaps and to review the current literature.
Keywords: SURGICAL FLAPS; EAR; CARCINOMA, BASAL CELL
Cutaneous flaps constitute an important reconstructive technique in dermatologic surgery. They are characterized by the maintenance of the original vascular pedicle in the tissue to be transplanted and, for didactic purposes, can be classified into: advancement, rotation, transposition, interpolation, island and subcutaneous flaps. 1 Aiming at obtaining the best aesthetic outcome, the choice of the surgical technique for reconstructing facial areas must consider items such as vascularization, tension caused by the suture, skin redundancy, tension lines, the surgeon's experience with a certain technique and the base condition, among other factors.1, 2 The ear is comprised by the auricle (formed by cartilage with convexities and concavities covered with thin skin), the lobe (fibroadipose tissue) and the external auditory meatus. 1 Due to the small amount of skin available and restricted vascularization, in addition to the fact that the ear is an area difficult to manipulate, the surgical reconstruction in that region is challenging.
Basal cell carcinoma (BCC) is a common cutaneous neoplasm whose excision does not always allow primary closure of the surgical incision, especially in the ear. In this paper, the authors describe their experience with the reconstruction of the triangular fossa – a branch of the anti-helix and concha – after excision of BCC, employing flaps originated from similar cosmetic units using two different techniques.
Case 1
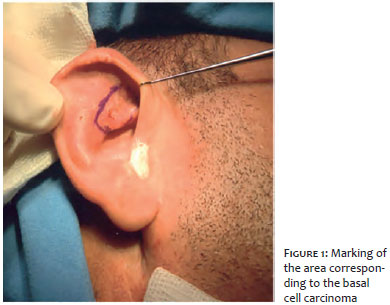
A 46 year-old male patient who did not have comorbidities bore a lesion in the auricular anti-helix with approximately 3cm in diameter in its longest axis and that was clinically suggestive of BCC.
Anterior auricular flap surgical technique
After both the lesion to be excised (Figure 1) and the pre-auricular flap were marked, local anesthesia and regional block were carried out with 2% lidocaine, epinephrine and 8.4% sodium bicarbonate solution.
The removal of the nodular lesion located in the triangular fossa was performed using curettage followed by spindle excision up until the cartilage was exposed (Figure 2).
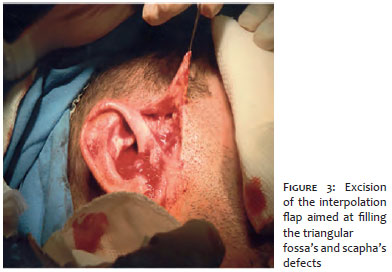
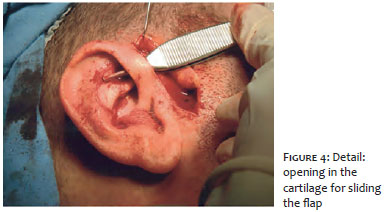
Next, the flap was prepared in the pre-auricular region (Figure 3). The transection of the helix by the flap's pedicle and subsequent positioning on the open area was performed via an incision in the helix's skin and cartilage (Figure 4). Suture with 5.0mm mononylon thread for internal stitches was then carried out, followed by a simple suture for attaching the flap to the receiver area.
The surgery was completed with the primary closure of the donor area in the anterior auricular region (Figure 5).
The pedicle resection and the defect closure was carried out in a second surgical time using 5.0 mononylon thread.
Case 2
A 83-year-old male patient with chronic obstructive pulmonary disease had been bearing a pruriginous ulcerated lesion located at the auricular concha for 8 months. The lesion had progressively grown in the previous 4 months. Clinical examination evidenced an ulcerated lesion with pearly border, as well as telangiectasias, suggesting the clinical diagnosis of BCC.
Posterior auricular flap surgical technique
The excision of the lesion located in the auricular concha was performed similarly to that described in Case 1.
In Case 2, however, the flap was originated from the retroauricular region, having been transfixed through the concha's cartilage, aimed at accommodating the flap in the receiving area (Figure 6). The suture was the carried out for attaching the flap in the receiving bed and primarily closing the donor area. The resection of the pedicle and closure of the defect were performed in the second surgical time (Figures 7 and 8).
Both ear reconstruction techniques were successfully performed with absence of complications, leading to excellent aesthetic and functional outcomes, based on the use of flaps prepared using both the anterior and posterior regions.
In both cases, the pathological examination's result of the surgical specimen evidenced BCC with free margins.
The use of flaps for reconstructing the ear after the excision of tumors is the most indicated technique, for direct closure is not feasible and grafts are difficult to adhere to this region. 1,2 Sites with adequate similarity and rich vascularity should be used as donor areas. 2-4 Among the sites compatible for ear reconstruction, the pre-auricular 5 and posterior auricular areas, as well as the retroauricular sulcus and the mastoid region stand out. 3,4
Interpolation flaps are performed by shifting the tissue to a nearby – but not contiguous – receiver area. 1 This technique was chosen due to the possibility of better local vascularization and aesthetic outcome, as compared to the second-intention closure. 2,6
Despite being the first choice in the reconstruction of the concha, the posterior flap's interpolation technique (or Masson's flap), firstly described in 1972, is a high-risk procedure. 6 The tissue tends to allow only a narrow pedicle, and performing the rotation inside the ear hampers local blood circulation. 6 Stemming from these characteristics, complications, such as necrosis, might arise. 7 Nevertheless, the literature does not highlight the need to preserve the posterior auricular artery's pedicle and suggests that the preservation of 50% of the flap's vascular pedicle is sufficient for its viability. 7
In this flap type, special attention should be given to the second surgical time 3 weeks after the primary approach, making possible proper revascularization, adhesion and viability of the transferred tissue. 2 This caution was observed in the reported cases. The need for the second surgical time is however a limiting factor for patients with low adherence to the treatment, with the risk of loss of follow-up. 8 As a consequence, the need for an additional intervention after the first surgery should be explained to the patient.
The pre-auricular region's flap was initially described by Pennisi and is also an option when it is not feasible to use retroauricular flaps (for instance, when there is a tumor in this region). 9 While thin, the flap originating from this area has the advantage that it can be used in the reconstruction of the upper and lower regions of the ear, 10 as well as being a better option than closure by second intention (associated with increased risk of infection and retraction as compared to covering the cartilage with flaps). 2.9
Due to the use of similar aesthetic units (skin with similar color and texture), this technique leads to a good aesthetic outcome and preserves the anatomy of the ear pavilion by maintaining its natural curvature. 8, 10
The anterior and posterior ear flaps techniques should be part of the therapeutic armamentarium for the correction of larger surgical defects arising from the removal of extensive tumoral lesions, preserving the site's anatomy, functionality and aesthetics.
1. Silva, SCMC. Técnica Avançada de Excisão. In: Cirurgia Dermatológica Teoria e Prática. Rio de Janeiro: DiLivros; 2008. p. 173 – 256.
2. Cordova A, D'Arpa S, Pirrello R, Giambona C, Moschella F. Retroauricular skin: a flaps bank for ear reconstruction. J Plast Reconstr Aesthet Surg. 2008;61(Suppl 1): S44-51.
3. Lynch J, Mahajan AL, Regan P. The trap door flap for reconstructing defects of the concha. Br J Plast Surg. 2003;56(7):709-11.
4. Johnson TM, Fader DJ. The staged retroauricular to auricular direct pedicle (interpolation) flap for helical ear reconstruction. J Am Acad Dermatol.1997;37(6): 975-8.
5. Sánchez-Sambucety P, Alonso-Alonso T, Rodríguez-Prieto MA. Tunnelized Preauricular Transposition Flap for Reconstruction of Anterior Auricular Defects. Actas Dermo-Sifiliográficas. 2008,99(2):161-162.
6. Masson, JK. A simple island flap for reconstruction of concha-helix defects. Br J Plast Surg. 1972;25(4):399-403.
7. Talmi YP, Horowitz Z, Bedrin L, Kronenberg J. Auricular Reconstruction with a Postauricular Myocutaneous Island Flap: Flip-Flop Flap. Plast Reconstr Surg. 1996; 98(7):1191-9.
8. Suchin KR, Greenbaum SS. Preauricular Tubed Pedicle Flap Repair of a Superior Antihelical Defect. Dermatol Surg. 2004;30(2 Pt 1):239-41.
9. Braga AR, Pereira LC, Grave M, Resende JH, Lima DA, De Souza AP, et al. Tunnelised inferiorly based preauricular flap repair of antitragus and concha after basal cell carcinoma excision: Case report. J Plast Reconstr Aesthet Surg. 2011;64(3): e73-5.
10. Pennise VR, Klabunde EH, Pierce GW. The Preauricular Flap. Plast Reconstr Surg. 1965;35:552-6.
This study was performed Hospital Universitário Pedro Ernesto – Universidade do Estado do Rio de Janeiro (Hupe/Uerj) - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}