


Artur Jorge Fernandes César1; Ana Margarida Barros2; Paulo Henrique Santos2; Filomena Maria Azevedo3
Repairing surgical defects of the nasal tip is challenging, mainly because of the lack of freely mobile skin available peripherally. The Peng flap is a one-stage cutaneous flap that circumvents this difficulty by recruiting skin from the nasal dorsum and sidewall regions. The design produces a tridimensional shape perfectly adapted to the conFiguretion of the nasal tip and allows for an inconspicuous closure of the defect. Herein, we describe a modified version of a Peng flap in a single-stage procedure, performed in three patients subjected to excison of basal cell carcinomas.
Keywords: NOSE; NOSE NEOPLASMS; CARCINOMA, BASAL CELL; SURGICAL FLAPS
Basal cell carcinoma (BCC) is the most common non-melanoma skin cancer affecting the head and neck regions. 1 Nearly 80% of all BCCs arise in the facial region, with up until 30% of these, occurring in the nose. 2 Surgical excision is the treatment of choice; however, it is often challenging to close the surgical defects when they are located in the nasal tip, mainly due to the lack of elastic and mobile skin at the defect's periphery so that direct suture can be performed.
This paper describes 3 cases of women with full thickness surgical defects located in the nasal tip, resulting from the excision of BCCs, in which the used reconstructive technique was a modified version of the Peng flap.
The purpose of the present article is to describe this reconstruction technique, demonstrate its aesthetic results and discuss its surgical applicability in light of the literature and the authors' experience.
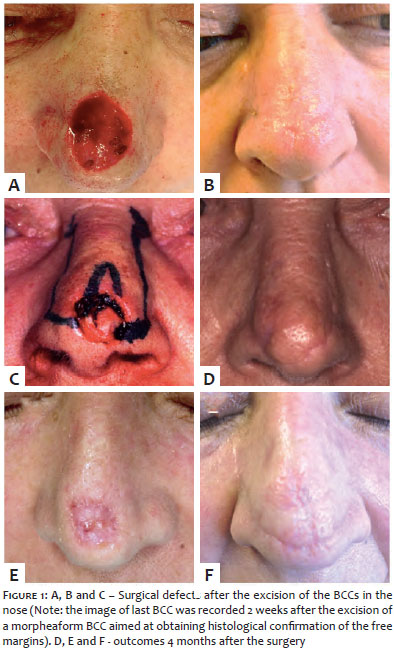
Three patients bearing BCCs in the nasal tip (nodular, micronodular and morpheaform types, respectively) underwent wide excision of the tumors. In two of the cases the removal of the BCC and the closure of the surgical wound were performed in one surgical time. In the other case, due to the morpheaform lesion's poor delimitation, the BCC was excised in the first surgical time, with the closure being performed in a second surgical time, after margins free of neoplasia were histologically confirmed.
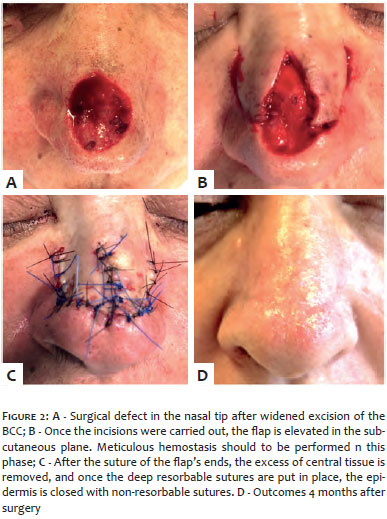
The post-excisional defects measured between 1.6cm and 2.0cm horizontally and between 1.6cm and 2.2cm vertically (Figures 1A, B and C). The intraoperative steps of the closure technique were as follows (Figure 2):
• The flap was demarcated with the incision beginning in the surgical defect's distal margins, continuing laterally and superiorly, along the ala nasi folds and the transition between the nose's lateral region and the malar region;
• Local with 1% lidocaine was performed in the nasal pyramid;
• After the incision of the skin was carried out, the flap and the surrounding skin were separated from the subcutaneous plan. Meticulous hemostasis was performed at this moment aimed at avoiding any bleeding or hematoma that might compromise the flap's survival;
• The distal extremities of each of the flap's "arms" were trimmed (in order that a thickness adequate to the defect could be obtained) and sutured in place using resorbable subcutaneous sutures 4-0;
• The excess of triangular skin in the center of the flap's "arms" were removed later on. (Note: in midline defects, the triangle's direction should be vertical, while in eccentric defects it must be directed obliquely towards the wider "arm" of the flap);
• Once the deep resorbable sutures are completely put in place along the flap's limits, the removal of the redundant tissue in the eye's medial epicanthus area is sometimes necessary in order to prevent "dog ear" deformities;
• Finally, the epidermis was approximated using non-resorbable sutures 5-0 with the proper eversion of the wound's edges;
• The non-resorbable sutures were removed between 8 and 10 days after the procedure, and the patients re-evaluated monthly for the first 4 months.
The postoperative recovery was uneventful. Figures 1D, 1E and 1F depict the outcomes 4 months after the reconstructive surgery, with absence of any distortion of the nasal anatomy and with excellent aesthetic results.
The reconstruction of surgical defects in the nasal tip poses particular difficulties given the three-dimensional shape form the latter and the limited area from which to mobilize skin with similar characteristics (thickness, color and adnexa composition). The more frequently used closure methods in this location are: the primary closure (small defects), cutaneous flaps (bilobed flap, dorsal-nasal glabellar flap, Rintala flap, bilateral rotation flap and frontal paramedian flap), and skin grafts.
The Peng cutaneous flap is seen as an advancement and rotation flap that was initially described by Peng et al. in 1987. 3 This flap's fundamental concept is a "pincer-like" modification applied to the Rintala flap (linear advancement flap starting in the glabella and dorsum of the nose), classically used to repair defects on the nasal dorsum and tip. 3 This modification allows the closure of larger defects in the nasal tip, taking advantage of the skin excess in the lateral wall of the nose, and improves the flap's survival, since it reduces the length and widens the pedicle's base. Furthermore, the medial rotation movement in its two "arms" produces a convex configuration that perfectly adapts to the nasal tip's three-dimensional shape. 4
In 1995, Rowe et al. proposed to begin the incisions of the flap's two "arms" more distally regarding the defect, thus reducing the extent of the flap's advancement. 4 More recently, Ryan et al. added another modification, placing the incisions more laterally along the transition between the nose and the cheek. In most of the total thickness defects in the nasal tip that the authors have performed in their care service practice, they have implemented the last version of the modified Peng flap. This is not only due to the fact that the pedicle's base is larger therefore improving the flap's survival, but also because it produces better aesthetic outcomes since the incisions are placed along the junctions between different facial aesthetic units. 5 Moreover, this flap's symmetrical shape minimizes the risk of asymmetrical distortion of the nose, especially of the nasal ala, a complication sometimes observed in other flaps used in the nasal tip. 4
In the authors' experience with more than 20 patients who underwent this procedure, the Peng flap led to excellent results in medium/large nasal tip defects, whether paramedian or located in the midline. It still leads to good outcomes in defects simultaneously involving the distal portion of the nasal dorsum and the tip of the nose. However, the authors' opinion is in line with that of others, who advocate that this flap is not suitable for most defects affecting more than 50% of the nasal tip subunit or deep defects involving cartilage. In these cases, the additional volume of frontal paramedian flaps, skin grafts or composite techniques, should be considered. The authors of the present paper did not observe cases of distortion or complications with this technique; nonetheless, this flap is not exempt from possible complications. In addition to cases of partial necrosis and infection, cases of elevation of the nasal alae have been described in larger defects, as well as asymmetries in eccentric defects, corrected by this technique. 4.5
In conclusion, this modification of the Peng flap is a reconstructive technique for defects in the nasal tip, even when they extend up until the nasal dorsum, being capable to be executed in a single surgical time. This flap usually leads to excellent matching of color and texture with the perilesional skin, preserves the nasal architecture and results in minimum surgical scars, which are camouflaged in the transition lines between facial aesthetical subunits. Thus, the authors of the present paper are of the opinion that this is an essential tool for the dermatologic surgeons' armamentarium for reconstructing defects in the nasal tip.
1. McGuire JF, Ge NN, Dyson S. Nonmelanoma skin cancer of the head and neck I: histopathology and clinical behavior. Am J Otolaryngol. 2009;30(2):121-33.
2. Choi JH, Kim YJ, Kim H, Nam SH, Choi YW. Distribution of Basal cell carcinoma and squamous cell carcinoma by facial esthetic unit. Arch Plast Surg. 2013;40(4):387-91.
3. Peng VT, Sturm RL, Marsh TW. "Pinch modification" of the linear advancement flap. J Dermatol Surg Oncol. 1987;13(3):251-3.
4. Rowe D, Warshawski L, Carruthers A. The Peng flap. The flap of choice for the convex curve of the central nasal tip. Dermatol Surg. 1995;21(2):149-52.
5. Ahern RW, Lawrence N. The Peng flap: reviewed and refined. Dermatol Surg. 2008;34(2):232-7.
This study was performed in the Centro Hospitalar São João EPE - Porto, Portugal.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}