


Meire Brasil Parada; Camila Cazerta; Joao Paulo Junqueira Magalhães Afonso; Danielle Ioshimoto Shitara do Nascimento
Filler injections are among the most popular cosmetic procedures performed worldwide. Although fillers have a safety profile, there has been a rise in litigation as a result of treatments in the USA. In the Brazilian scenario, the number of non-surgical procedures has increased in the past years, mainly due to the increase of filler options available in the Brazilian market, as well as in the type of professionals allowed to perform injectable procedures. Therefore we sought to review the related literature regarding semi-permanent and temporary fillers adverse effects and outline a practical guide for complications avoidance, diagnosis and management.
Keywords: GRANULOMA; ISCHEMIA; ESTHETICS; HYALURONIC ACID; DERMIS; SUBCUTANEOUS FAT; BIOFILMS; INFECTION
According to the American Society for Aesthetic Plastic Surgery, more than 13.5 billion dollars were spent on surgical and nonsurgical procedures in the USA in 2015, with nonsurgical procedures accounting for 42% of the total value1. While nonsurgical cosmetic procedures have increased by 44% in the past 5 years, injection based procedures have increased by 21%.
In the survey conducted by the International Society of Aesthetic Plastic Surgery, 20 million cosmetic procedures were performed worldwide in 2014, with Brazil ranking third for non-surgical procedures. Nonsurgical procedures accounted for 51% of the total procedures, with botulinum toxin and cutaneous filler injections being the most popular. Botulinum toxin and hyaluronic acid accounted for 71% of non-surgical procedures2.
In the United States, with the increased use of soft-tissue fillers, there has been a concomitant rise in litigation asserting harm as a result of treatments. The most common lesion giving rise to litigation was the formation of granuloma or autoimmune reaction3.
The number of cosmetic filler options available in the Brazilian market has increased in the past years. Although soft tissue fillers have a very favorable safety profile, between 2003 and 2008 the US Food and Drug Administration has received 930 post-marketed reports of adverse effects, with 823 of those having been classified as severe4. Therefore the authors of the present study sought to review the literature regarding semi-permanent and temporary fillers adverse effects, as well as outline a practical guide for avoiding, diagnosing and managing complications.
Pre-treatment considerations: clinical assessment and informed consent
Assessing the patient prior to the injection procedure is vital, not only aiming at evaluating the patient's expectations, choosing the optimal product, planning the injection, and choosing the injection points, but also evaluating the risks involved.
Patients should be thoroughly queried regarding medical history of bleeding disorders, herpes, auto-immune diseases, pregnancy, allergies, keloid formation and use of medicaments, such as blood thinners (including coumadin and non-steroidal anti-inflammatory drugs), or vitamins/herbal supplements associated with prolonged bleeding – examples include (vitamin E, chondroitin, feverfew - Tanacetum parthenium, ginger, garlic, ginseng, gingko-biloba, kava-kava, celery root, and fish oils)5, 6. Herbal medications should be discontinued 7-10 days prior to the procedure to reduce the risk of hematomas. Regarding patients under use of anticoagulant medication, if it has been is prescribed for a limited period of time, it may be prudent to postpone the injection treatment until the patient has stopped taking the drug. Nevertheless, if the medication has been prescribed indefinitely, the benefit-risk of discontinuing these drugs should be carefully evaluated 5,7.
The history of aesthetic procedures should be assessed observing the types of previous aesthetic procedures the patient has undergone and the types of fillers used, as well as previous allergic reaction to fillers or anesthetics.
Overall, fillers should be avoided in case of active adjacent site of infection (intraoral, mucosal, dental or even sinusitis), adjacent inflammatory process, immunosuppression, allergy to filler components or lidocaine, pregnancy and breastfeeding 8,9.
In case of active adjacent site of infection, the procedure should be postponed and the infection should be treated before any injection. If the patient is under dental treatment, Parahitiyawa et al. also recommend to postpone the procedure, due to the fact that dental treatment can cause transitory bacteremia, which is already proven to have systemic impact and lead to diseases, and in theory can also cause colonization of the filler and formation of a bacteria biofilm10. The patient should be advised of the risks in case the physician chooses to perform the procedure during an active infection. The use of prophylactic antibiotic is debatable.
The use of semi-permanent or temporary fillers in an area where permanent fillers have already been injected should be avoided due to the risk of exacerbation or stimulation of nodule formation11. Nevertheless, injection in areas different from those where permanent fillers have already been injected could be performed after careful evaluation of the permanent filler's location assisted by imaging techniques (high-frequency ultrasound - HFUS, optical coherence tomography, MRI and scintigraphy) 12-15 is carried out prior to the treatment, clearly defining the area that should be avoided. High frequency ultrasound has proven to be the first line tool (quick and cost-effective) for assessing filler site and class (temporary vs permanent). In complicated cases, MRI seems to be very helpful in correctly evaluating filler migration and identifying subcutaneous abscesses or granulomas15.
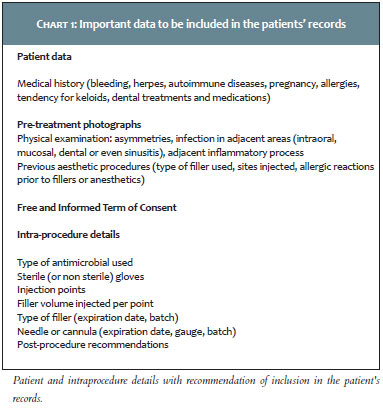
Photographs should be taken aimed at documenting the patients' appearance before the procedure, as well as for better analyzing the patient's areas of concern and eventual asymmetries. The patient's objectives and corresponding best filler types for his or her needs, risks and costs involved in the procedure should be discussed with the patient prior to the treatment, aiming at setting real expectations (7). The patient should read and sign a free and informed term of consent and the data in Table 1 should be well documented 16.
Intra-procedure general recommendations
In order to prevent infections and biofilm formation, all makeup and other potential contaminants present on the skin should be removed. In addition, the skin should be cleansed with an antimicrobial preparation, such as aqueous or alcoholic 2-4% chlorhexidine11,17. Chlorhexidine should be avoided in the periocular area due to risk of keratitis7. Also, it may be useful to have the patient rinse the mouth with a mouthwash before an injectable procedure to reduce oral microbiota. Oral 0.12%-0.2% chlorhexidine mouthwash was the most effective in reducing tooth biofilm in vivo 18, 19.
Even though it has not been proven that the use of non-sterile gloves and alcoholic chlorhexidine is insufficient in preventing filler infections, employing sterile technique throughout the procedure (i.e. using sterile gloves, drapes, gauze), in some authors' opinion may reduce the risk of these complications7,11. Making sure that good illumination is used during the procedure also helps to identify and avoid superficial vessels, reducing the risk of hematoma.
Injecting the product in the correct plane is critical to minimize adverse events, such as superficial placement. Some visual cues help the dermatologist physician to recognize the right plane for injection. For instance, in the superficial planes, the gray of the needle can be observed and the skin whitens. In the deep dermis, the gray of the needle is not seen, however its shape can be recognized. The supra-periosteal plane is reached inserting the needle perpendicular to the skin, until the periosteum can be palpated with the tip of the needle (7). The needle should be then pulled back slightly for better product placement.
Post-procedure general recommendations
Patients should not apply non-sterile make up in the first 4 hours after the procedure7. If massage is needed, for example after the injection of poly L-lactic acid (PLLA), aqueous or degerming chlorhexidine can be useful.
Managing adverse events
I) Early reactions (from a few days to several days)
A) Local reactions
Local reactions can be related to the injection alone, including local inflammation, hyperemia, tenderness, and hematoma. These are mainly influenced by the needle's gauge, physico-chemical properties of the injected material, and speed of injection4. Injection techniques that increase the dissection of the sub-epidermal plane (i.e. fanlike technique, rapid injection, rapid flow rates, higher volumes) have been associated with an increased number of local adverse events, due to tissue distension and trauma6,20. The use of blunt-tipped cannulas may decrease bleeding, hematoma and pain due to reduced intra-tissue trauma and number of punctures21.
B) Erythema
Transient erythema can occur, especially if massage is performed after the procedure. Anti-histamine and topical steroids can help minimize transient redness. In case of persistent erythema, after exclusion of hypersensitivity reaction and infection (22), the use of light treatments such as IPL and LED has been described6, 23.
C) Swelling
Swelling is one of the most common complications associated with fillers. Edema is usually localized and self-limiting. Most prone areas are the lips and periorbital region. The correct choices of product for the treatment area, as well as of correct plane for the treatment help prevent swelling. Applications of ice, anti-histamines and short time prednisone use, as well as the elevation of the head, have been described6. A rare form of recurrent and intermittent swelling that occurs after alcohol intake, sunlight exposure or vigorous exercise, has been reported.9
D) Superficial placement of fillers
The superficial placement of fillers can lead to blanching or, in case of hyaluronic acid (HA), bluish discoloration in the injection area (Tyndall effect)24. The Tyndall effect may result from either traces of hemosiderin after vascular lesion and/or visual distortion of light through the skin due to refraction caused by the filler25. Fillers should only be injected after the needle has reached the appropriate depth and injection should be stopped before the needle is withdrawn. Also, placement in the correct plane is crucial. For example, semi-permanent fillers, such as poly-L-lactic acid (PLLA) or calcium hydroxyapatite (CaOH), cannot be placed too superficially and need to be injected in the subcutaneous or supra-periosteal planes6.
Local massage, incision and drainage, and, in case of HA, hyaluronidase (HYAL), are treatment options. Also, the use of Q-switched 1,064nm laser has been reported26.
Calcium hydroxyapatite is ideally placed in the subcutaneous and may present product migration if the product is placed superficially or in highly mobile areas, such as the lips. Treatment options are intra-lesional steroid injection, saline injection followed by massage, incision and expression or surgical removal7. Also superficial filler placement can lead to lumps and nodule formation. Please, refer to the Nodules and the Lumps sections.
E) Herpes activation
The risk of herpes activation following dermal filler injection due to direct damage to the axon caused by the needle, with subsequent tissue manipulation and inflammatory reaction27 is estimated to be less than 1.45%. Since there are no defined guidelines, a systemic antiviral prophylaxis can be performed in patients with personal history of recurrent facial herpes (>3 episodes/year). Acyclovir 400mg three times per day for 10 days or valacyclovir 500mg twice per day for 7 days can be employed, starting 2 days before the procedure (28).
F) Infection
Early-onset infections arise with induration, erythema, tenderness and pruritus, and might be indistinguishable from transient post-procedure response. Fluctuating nodules and systemic symptoms (fever, chills) can occur later on. Skin infections are usually related to resident flora (Staphylococcus or Streptococcus spp.) introduced through injection. Microbiological culture should be performed and culture-appropriate antibiotic treatment installed. Abscess should be drained. In longer lasting infections or poor response to antibiotics, atypical infection (i.e. Mycobacterium spp.) and biofilms should be considered. In these cases alternative antibiotic may be necessary.
G) Acute hypersensitivity
Foreign body fillers can trigger immune response. Hypersensitivity reactions can range from mild redness to anaphylaxis. The incidence of hypersensitivity reaction related to HA is around 0.6%. About 50% (4) of these cases are transient and resolve within 3 weeks. In a prospective, randomized study, 433 patients injected with NASHA HA were evaluated using skin testing, IgE and IgG antibody serology, and histopathology studies. No detectable allergenicity (Type 1) or delayed hypersensitivity (Type IV) was reported (29). Use of anti-histamines, non-steroidal anti-inflammatory drugs (NSAIDs), intralesional or systemic steroids, minocycline and hydroxychloroquine have been reported. Hyaluronidase may help removing the core of the inflammation (30).
H) Lumps
Lumps are caused by excessive HA, superficial product placement, areas of thin skin (i.e. eyelids) or migration due to muscle movement (i.e. lips) (22). Treatment options comprise aspiration, incision and drainage or removal by HYAL injection in case of HA (24). It is important to note that this reversion ability of HA is unique (6). Previously diluted HYAL and lidocaine can be used to dissolve the lump (31).
In a retrospective study conducted in Brazil, 50 patients who underwent HYAL injections to treat complications or unaesthetic results following HA injections were given doses of this enzyme ranging from 40 to 160 Units per anatomic area (32).
I) Vascular complications
The most feared complication among those caused by the use of dermal fillers is injection-induced necrosis, which is caused by vascular occlusion or trauma. Impending necrosis was described with different filling materials with an estimated frequency of 0.001% of total procedures performed (33).
First and foremost, a thorough knowledge of the facial vascular network is crucial, especially when treating areas with terminal blood vessels, such as the glabella and the nose. Among risk factors for intra-arterial injection are related to: 1) the injected areas: high-risk areas include areas near the facial artery, angular artery along the nasolabial fold, nose and glabella. The glabella has tenuous blood supply, originating in branches of internal and external arteries, having a close connection with the eye's vascular system. The facial artery becomes superficial close to the pyriform fossa at the apex of the nasolabial fold. Therefore in this area, the filler placement should be carried out deeply in the supra-periosteal area with a needle, or more superficially, with a blunt cannula; 2) large volume of injection; 3) small sharp needles, that are more likely to penetrate the vascular lumen, as compared to larger bore needles and cannulas. Nevertheless blunt cannulas may reduce – but not eliminate – the risk of vascular lesion; 4) previous scarring, which stabilize and immobilize arteries in place, making them easier to penetrate with needles; 5) composition of the filling material: permanent fillers cannot be dissolved and can obstruct the lumen (34). The filling material primarily implicated in blindness is fat. Nonetheless, other substances, such as collagen, CaOH and HA, have also been reported to have caused blindness (30).
The typical clinical appearance following HA filling caused ischemia is transient blanching (duration of a few seconds), followed by a livid pattern or reactive hyperemia (minutes), black-bluish discoloration (ten minutes to hours), blister formation (hours to days), and cutaneous necrosis and ulceration (days to weeks).
Preventative measures include the use of small volumes, greater than 27G blunt cannulas, and slow injection. Aspiration prior to injection does not ensure vascular safety, but should be performed.
Clinical symptoms that should prompt the physician to immediately stop injecting are: pain, skin blanching or color changes (livedo, blue or gray color) in the distribution of the regional blood vessels. Another cue is observing the blood return after digital compression of the area. Return to normal color takes 1-2 seconds. Slower capillary blood return may be a sign of arterial insufficiency (35). Ice and epinephrine may mask the signs and symptoms of arterial insufficiency.
Hyaluronidase is considered the backbone of vascular occlusion treatment (5, 34). It consists of a soluble protein enzyme that hydrolyzes both natural and cross-linked HA. Even tough actual need of intravascular injection has been reported (34), diffuse injection of HYAL into the tissues affected by ischemia seems to be enough in most cases, for HYAL can easily cross facial planes and tissue structures by affecting the HA of the dermal matrix (35, 36).
A recent consensus recommendation for impending necrosis treatment included (33):
1) The use of significant amount of HYAL in the area of necrosis. It is important to flood the area, as soon as possible. A minimum of 200UI is recommended. No test is needed to assess impending necrosis. Early HYAL injection reduced the size of necrosis in animal experiments, when compared to late injection (24hs) (33). Also, the nature and quality of the dermal filler are important considerations for HYAL effectiveness. Hyaluronidase hydrolyzes Restylane® more quickly and with smaller volumes when compared to other HAs (Juvederm®, Volbella®, Prevelle® and Belotero®) (11, 33, 36-38). If no improvement is seen in 60 min, the injection should be repeated.
2) Vigorous massage and warm compress (for 5-10min, every 30-60 min).
3) Massaging topical 2% nitroglycerin (NTG) paste on the area immediately on suspicion of necrosis and up to 2-3 times daily is an option39. The patient should be lying down during the application of NTG to prevent syncope by fall of blood pressure due to systemic vasodilation. In addition, nitroglycerin paste is contra-indicated in patients taking PGE2 medications such as Viagra® (Pfizer, NY, USA). Alternative protocol39: nitroglycerin paste under occlusion for 12hs, followed by a 12-hour interval before applying again.
It is important to highlight that the use of topical NTG is controversial, since according to the preliminary data in animal models, topical NTG was not effective and, in theory, could worsen the picture with dilation of the arterioles, further propagating the product into the smaller capillaries, causing increased dermal ischemia40.
Nitroglycerin is not available in Brazil.
4) Introduce oral aspirin regimen: two 325mg pills per day, usually for 1 week to prevent further clot formation33. Since in Brazil available aspirin dosages are 100mg and 500mg, patients can take 500-600mg daily for 1 week.
5) Daily patient follow-up: HYAL and NTG can be continued as needed for the following few days. If improvement is observed, NTG massages can be stopped. If there is no improvement or progression, HYAL, NTG and aspirin should be repeated daily.
6) Daily low-molecular weight heparin, prostaglandin E1, systemic anticoagulation, hyperbaric oxygen therapy, and sildenafil have been recommended as other treatment options 41.
7) Patient aftercare should ensure: proper wound care with daily dressings and wound coverage with ointment to prevent crusting, skin hydration, debridement of necrotic skin and secondary infection prevention.
Even though the use of HYAL for the reversal of vascular complications is "off-label", the prompt diagnosis and immediate treatment with this enzyme is crucial33.
II) Late onset reactions (from weeks to years)
A) Nodules
In a 5-year retrospective review, 14 complications were reported out of 2,089 injectable soft-tissue filler treatments (PLLA, HA and CaOH), with nodule or granuloma formation being the most common. Calcium hydroxyapatite was the filling substance that was most associated with complications in this series (2.6% of treated cases)42. Delayed reactions to HA-based fillers are estimated to occur in approximately 0.02% of treatments43. More recently, the authors of a retrospective study reported an exceptionally high rate of late-onset recurrent and resistant inflammatory nodules (4.25% vs expected 0.02%) after HA injection using Vycross technology38.
Nodules can occur due to the misdistribution of the filling material, reaction to the product (including inflammation, hypersensitivity or granulomatous reaction) or infection25. Most are palpable and not visible, and can be noticed immediately after the procedure or several months later (late-onset).
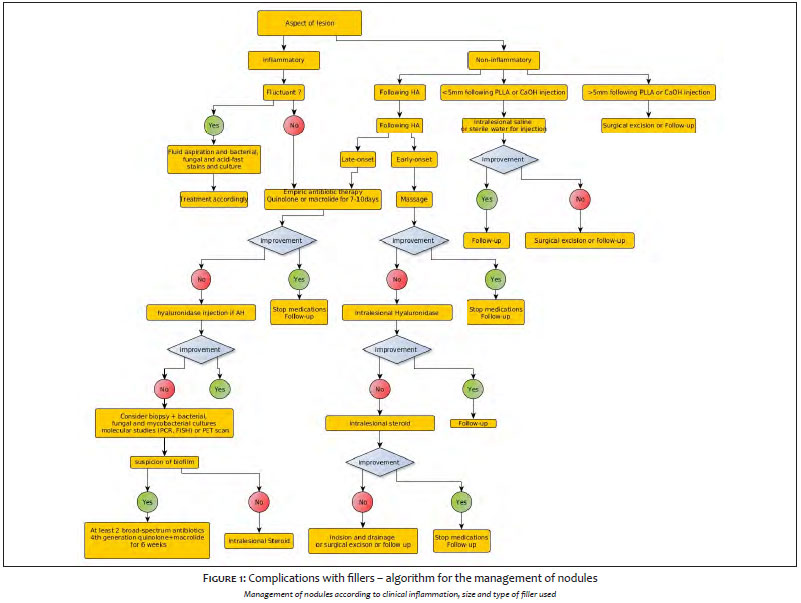
Nodules may be asymptomatic or inflammatory, and can present erythema, tenderness and swelling. These are denominated angry red bumps by some authors9,30. The role of biofilms in late-onset nodule formation has been discussed recently. Biopsy should be considered to differentiate infectious and inflammatory processes. The authors of the present study propose an algorithm for the management of nodules (Figure 1).
A1) Nodules caused by misdistribution of fillers (non-inflammatory)
Superficial placement of CaOH can lead to white nodules, especially in the lips. These nodules might resolve spontaneously or become permanent4. Incision with a number 11 blade or needle, and expression or surgical excision is recommended (24). Injection of saline can be performed in an attempt to dilute the material11.
Poly-L-lactic acid: palpable non-inflammatory nodules with sizes greater than or equal to 5mm can occur due to incorrect reconstitution, uneven product distribution in the suspension, superficial injection, product placement in contraindicated areas (such as perioral region and eyelids), or lack of post treatment massage4. Recommendations of 8ml sterile water for injection dilution, at least 24hs before the procedure and deep plane placement (subcutaneous or supra-periosteal fat) reduce nodule formation to <1% 7,42,44. These lesions might resolve spontaneously, otherwise they need to be injected with saline.
A2) Inflammatory nodules
The histopathology examination inflammatory nodules may reveal foreign body reaction, infection, sterile abscess or granuloma30. Given that slow growing bacteria are thought to play a role in formation of nodules, some authors suggest that inflammatory nodules should be treated empirically as an infection. Empiric antibiotics such as clarithromycin 500mg 12/12 and/or a tetracycline should be administered for 7-10 days. If no improvement is observed, punch biopsy, microbiological culture and prolonged antibiotics should be considered30. Hyaluronidase has been used successfully.
A3) Granuloma
The term nodule is used generically when no pathological diagnosis is available. The term granuloma should only be used when the pathologic criteria of granuloma have been fulfilled11. Granuloma occurs in 0.01-1% of the treated population and is a distinctive form of chronic inflammation25,45, consisting of a nodular or more prolonged inflammation, with modified macrophages (epithelioid cells) and multinucleated cells. It typically appears months to years after injection and remains in the injection site. Many triggering factors have been proposed, such as systemic infection, intense exposure to sunlight and systemic drugs, however the pathogenesis of inflammatory granuloma remains unknown45-47. The inflammatory reaction may be caused by a hypersensitivity to the filling material or immunologic response to the protein contaminants in the preparations5.
Considering that subclinical granulomatous inflammation is normal and in case of some injected materials, the desired tissular response, the clinical significance of granulomatous inflammation should be based on its extent, severity and long-term progression of the response25. Clinically, granulomas may be accompanied by discomfort, persistent or transient edema, erythema and periods of crisis and regressions. Also, when all implantation sites develop a similar scenario, the differentiation from a nodule caused by filler misdistribution is easier (45).
In the absence of fluctuation and systemic symptoms, histologic and/or microbiologic examination is required to rule out infection. Histopathology is useful not only for the diagnosis of granuloma, but also for the recognition of the implant's nature (48). Permanent fillers present higher risk of granulomatous reaction (49). Less frequently, granulomatous reactions have been described after CaOH (50, 51), PLLA, and HA injections (45).
Intralesional steroid is the recommended treatment for granuloma (6). Usual dosage would be 5-10mg/cc, repeated 4-6 weeks later, according to necessity (9). In case of HA, HYAL injection may be a therapeutic option. Massage, oral steroids (0.5-1mg/kg/day up to 60mg/day), oral minocycline (anti-inflammatory, immunomodulating and anti-granulomatous properties), pulsed dye laser, intralesional bleomycin and intralesional 5-fluoracil have been reported as additional therapeutic tools. Antimalarials (hydroxychloroquine 4-6.6mg/kg/day) have anti-inflammatory and immunoregulatory properties, inhibiting phospholipase activity and blocking several pro-inflammatory cytokines (52). Retina evaluation should be performed periodically. Anecdotic reports have suggested colchicine, anti-histamines and cyclosporine A use in refractory cases. Surgical excision should be avoided during active inflammatory processes or in patients with multiple and/or extensive lesions, due to the risk of filler migration, fistulae formation, scars and persistent granulation tissue (52). The prognosis is usually good for temporary filler granulomas (49).
B) Infection
Late infection typically manifests as tingling sensation followed by swelling 8-12 days after injection. Usually common skin pathogens, such as S. aureus are associated. Symptoms are usually described as abscesses, abscess-like nodules, foreign-body nodules or delayed-onset reactions. Fluctuation and systemic symptoms help diagnose infection (25). Nevertheless, in face of a firm, tender mass or nodule, which develops from 2 weeks after the procedure, atypical infection and mycobacteria should be considered in the differential diagnosis (53). Biological material from biopsy or fluid aspiration should be sent for staining, and for alcohol-acid resistant bacterial, fungal and bacilli culture25.
B1) Biofilms
One factor is a common denominator for all biofilm implants: a bacterium or infective microorganism is necessary to contaminate the injection for the formation of a biofilm to begin. Biofilm is a glue-like matrix secreted by bacteria, forming a medium in which other bacteria thrive, while evading antibiotics and the immune system11. The colony-biofilm becomes antibiotic-resistant by lowering its metabolism, also being protected from phagocytosis by an extra-polymeric system membrane54. Chronicity and recurrence of infection are hallmarks of biofilms42.
Implanted foreign bodies can become infected with skin contaminants during a procedure, or be colonized by direct or hematological spread of an infectious agent55. Biofilm may exist in a dormant state and be activated by local trauma, manipulation and injections. Once the biofilm is activated, it can become an acute purulent or a sub-acute course infection, with granulomatous response to the activated biofilm. The active infection can be controlled with antibiotic therapy, however the underlying biofilm can generate recurrence.54
In addition to being difficult to treat, biofilms can be involved in delayed-onset skin reactions to fillers, such as granulomatous inflammation, abscesses, nodules or recurrent infection7,9,11. A review of hypersensitivity reactions reports suggested that most of the reactions described were due to infectious processes56.
Biofilms are difficult to diagnose, due to the fact that most microbiological cultures from biofilm-infected tissues are negative. Some bacteria are difficult to grow using traditional methodology, given that their slow-growing nature is often overgrown by faster growing bacteria. Molecular studies, such as PCR and fluorescent in situ hybridization (FISH) are more accurate methods55,57. Finding the location of the material for biopsy or HYAL injection in case of HA, can be performed by ultrasonography, computed tomography scan (radiopaque material), MRI (non radiopaque implant)55. Positron emission tomography scans may help identify foci of infection. Sufficient tissue from biopsy should be obtained for bacterial, fungal and mycobacterial cultures.
Some authors suggest avoiding additional injections in the region of the implant, as well as dental procedures and facial trauma for 2 weeks following dermal filler injection42. Even tough, the use of prophylactic antibiotics is debatable and it may be reasonable for certain large-volume filler injections54.
Since the risk of biofilm should be considered in late-onset reactions, the use of oral steroids and NSAIDs should be avoided. Biofilms may require a 32 times higher amount of antibiotics than that required for killing planktonic bacteria. The recommended treatment should consider the association of at least 2 broad-spectrum antibiotics such as a quinolone (i.e. ciprofloxacin) and a third-generation macrolide (i.e. clarithromycin) for up to 6 weeks7,21. Macrolides have superior efficacy in treating biofilms, since they accumulate in the subcutaneous fat21. In addition, since bacteria are bound to the foreign material, complete resolution is difficult without its complete removal42. Therefore use of HYAL should be considered in case of HA or excision (11). Another reported option is the use of intralesional 5-FU, which has been shown to interact with a bacteria regulatory gene (AriR) that inhibits biofilm formation55.
C) Filling material migration
Filler migration can occur early or late, regardless of the type of the filling substance. Several mechanisms, such as poor technique, high volume of filler injected, filler injected under pressure, massaging after filler injection, muscle activity, gravity, pressure-induced displacement (i.e. injection of additional filler), lymphatic and intravascular spread (more related to permanent fillers) have been related22,46. Imaging and histopathology techniques are of assistance in the correct diagnosis.
Hyaluronidase (HYAL)
It is important to point out that HYAL is not commercially available in Brazil. The dosage is highly variable, depending on the treated area and volume of HA placed, ranging from 25UI (in tear though) to 1,500UI (in the case of vascular occlusion)11. Hyaluronidase can be diluted in saline or local anesthetics, however the resulting pH may alter the efficiency of the enzyme. It may be injected slowly and directly into the site of HA injection36. Massaging is important for obtaining the therapeutic effect. Hyaluronidase treatment should be performed as soon as possible. In a review study, if HYAL were injected within 2 days, full recovery was expected. On the contrary, if injection of HYAL were delayed, there was an increase in the risk of scar and tissue defect formation58.
Adverse reactions to HYAL are uncommon. Urticaria and angioedema are reported in less than 0.1% of patients and have occurred after retrobulbar or intravenous injections5. Therefore, some authors suggested that before applying HYAL, a sensitivity test should be performed injecting 3 units intradermally, with the patient being observed for at least 20 minutes. Local swelling indicates a positive reaction and may reflect sensitivity to animal protein or to preservative or cross-reaction with bee venom5,24, 36,41.
Hyaluronidase has a half-life of 2.1 minutes, caused by inactivation in the kidneys and liver. The most common drug interactions occur with furosemide, benzodiazepines, and phenytoin, which are incompatible with HYAL. Hyaluronidase should not be used to enhance the absorption and dispersion of dopamine and/or alpha agonist drugs. Also, HYAL may accelerate the onset, shorten the effect's duration, and increase the incidence of systemic reactions to local anesthetics. Large doses of salicylates, cortisone, ACTH, estrogens or antihistamines may require larger amounts of HYAL for an equivalent dispersing effect (31).
The dermal filler's nature and quality are important factors for the effectiveness of HYAL in case of an adverse effect. Hyaluronidase can more quickly hydrolyze Restylane® (Q-med) as compared to other HAs (Juvederm® - Allergan, Volbella® - Allergan, and Belotero®). Juvederm® takes significantly longer to disperse than Restylane®11, 33, 36-38.
Hyaluronidase should not be used in case of infection, due to the risk of spreading the infected material diffusely11.
Dermal fillers are among the most common aesthetic injectable procedures. Although considered very safe, adverse events may occur. Careful patient assessment, adequate therapeutic planning, and an accurate technique are crucial for achieving the best treatment outcomes. To be prepared to assess and handle possible adverse effects promptly is of paramount importance.
1. Surgery.org [Internet]. New York: The American Society for Aesthetic Plastic Surgery; c2009-16 [acesso 2016 Nov 23]. Disponível em: http://www.surgery.org/sites/default/files/ASAPS-Stats2015.pdf
2. Isaps.org [Internet]. Hanover: International Society of Aesthetic Plastic Surgery; c2006-16 [acesso 2016 Nov 23]. Disponível em: http://www.isaps.org/Media/Default/global-statistics/2015 ISAPS Results.pdf
3. Ezra N, Peacock EA, Keele BJ, Kingsley M. Litigation arising from the use of soft-tissue fillers in the United States. J Am Acad Dermatol. 2015 Oct;73(4):702-4
4. Luebberding S, Alexiades-Armenakas M. Safety of dermal fillers. J Drugs Dermatol. 2012;11(9):1053-8.
5. Hirsch RJ, Stier M. Complications of soft tissue augmentation. J Drugs Dermatol. 2008;7(9):841-5.
6. Winslow CP. The management of dermal filler complications. Facial Plast Surg. 2009;25(2):124-8.
7. Bailey SH, Cohen JL, Kenkel JM. Etiology, prevention, and treatment of dermal filler complications. Aesthet Surg J. 2011;31(1):110-21.
8. Sánchez-Carpintero I, Candelas D, Ruiz-Rodríguez R. [Dermal fillers: types, indications, and complications]. Actas Dermosifiliogr. 2010;101(5):381-93.
9. Lafaille P, Benedetto A. Fillers: contraindications, side effects and precautions. Journal of cutaneous and aesthetic surgery. 2010;3(1):16-9.
10. Parahitiyawa NB, Jin LJ, Leung WK, Yam WC, Samaranayake LP. Microbiology of Odontogenic Bacteremia: beyond Endocarditis. Clin Microbiol Rev. 2009;22(1):46–64.
11. DeLorenzi C. Complications of injectable fillers, part I. Aesthet Surg J. 2013;33(4):561-75.
12. Wortsman X. Identification and complications of cosmetic fillers: sonography first. J Ultrasound Med. 2015;34(7):1163-72.
13. Singh M, Wang S, Yee RW, Larin KV. Optical coherence tomography as a tool for real-time visual feedback and biomechanical assessment of dermal filler injections: preliminary results in a pig skin model. Exp Dermatol. 2016;25(6):475-6.
14. Di Girolamo M, Mattei M, Signore A, Grippaudo FR. MRI in the evaluation of facial dermal fillers in normal and complicated cases. Eur Radiol. 2015;25(5):1431-42.
15. Grippaudo FR, Di Girolamo M, Mattei M, Pucci E, Grippaudo C. Diagnosis and management of dermal filler complications in the perioral region. J Cosmet Laser Ther. 2014;16(5):246-52.
16. Jones JK. Patient safety considerations regarding dermal filler injections. Plast Surg Nurs. 2006;26(3):156-63.
17. Soothill JS, Bravery K, Ho A, Macqueen S, Collins J, Lock P. A fall in bloodstream infections followed a change to 2% chlorhexidine in 70% isopropanol for catheter connection antisepsis: a pediatric single center before/after study on a hemopoietic stem cell transplant ward. Am J Infect Control. 2009;37(8):626-30.
18. Mouchrek Junior JC, Nunes LH, Arruda CS, Rizzi Cde C, Mouchrek AQ, Tavarez RR, et al. Effectiveness of oral antiseptics on tooth biofilm: a study in vivo. J Contemp Dent Pract. 2015;16(8):674-8.
19. Quintas V, Prada-López I, Donos N, Suárez-Quintanilla D, Tomás I. Antiplaque effect of essential oils and 0.2% chlorhexidine on an in situ model of oral biofilm growth: a randomised clinical trial. PLoS One. 2015;10(2):e0117177.
20. Glogau RG, Kane MA. Effect of injection techniques on the rate of local adverse events in patients implanted with nonanimal hyaluronic acid gel dermal fillers. Dermatol Surg. 2008;34 Suppl 1:S105-9.
21. Gilbert E, Hui A, Meehan S, Waldorf HA. The basic science of dermal fillers: past and present Part II: adverse effects. J Drugs Dermatol. 2012;11(9):1069-77.
22. Kim JH, Ahn DK, Jeong HS, Suh IS. Treatment algorithm of complications after filler injection: based on wound healing process. J Korean Med Sci. 2014;29 Suppl 3:S176-182.
23. Calderhead RG, Kim WS, Ohshiro T, Trelles MA, Vasily DB. Adjunctive 830 nm light-emitting diode therapy can improve the results following aesthetic procedures. Laser Ther. 2015;24(4):277-89.
24. Cohen JL. Understanding, avoiding, and managing dermal filler complications. Dermatologic Surg. 2008;34 Suppl 1:S92-9.
25. Lowe NJ, Maxwell CA, Patnaik R. Adverse reactions to dermal fillers: review. Dermatol Surg. 2005;31(11 Pt 2):1616-25.
26. Hirsch RJ, Narurkar V, Carruthers J. Management of injected hyaluronic acid induced Tyndall effects. Lasers Surg Med. 2006;38(3):202-4.
27. Kim B, Somia N. Herpes reactivation after injection of dermal fillers. ANZ J Surg. 2013;83(12):998.
28. Gazzola R, Pasini L, Cavallini M. Herpes virus outbreaks after dermal hyaluronic acid filler injections. Aesthet Surg J. 2012;32(6):770-2.
29. Hamilton RG, Strobos J, Adkinson NF Jr. Immunogenicity studies of cosmetically administered nonanimal-stabilized hyaluronic acid particles. Dermatol Surg. 2007 Dec;33 Suppl 2:S176-85.
30. Sorensen EP, Urman C. Cosmetic complications: rare and serious events following botulinum toxin and soft tissue filler administration. J Drugs Dermatol. 2015;14(5):486-91.
31. Cavallini M, Gazzola R, Metalla M, Vaienti L. The role of hyaluronidase in the treatment of complications from hyaluronic acid dermal fillers. Aesthet Surg J. 2013;33(8):1167-74.
32. Balassiano LKA, Bravo BSF. Hialuronidase: uma necessidade de todo dermatologista que aplica ácido hialurônico injetável. Surg Cosmet Dermatol. 2014;6(4):338-43.
33. Cohen JL, Biesman BS, Dayan SH, DeLorenzi C, Lambros VS, Nestor MS, et al. Treatment of hyaluronic acid filler-induced impending necrosis with hyaluronidase: consensus recommendations. Aesthet Surg J. 2015;35(7):844-9.
34. DeLorenzi C. Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J. 2014;34(4):584-600.
35. DeLorenzi C. Transarterial degradation of hyaluronic acid filler by hyaluronidase. Dermatol Surg. 2014;40(8):832-41.
36. Landau M. Hyaluronidase caveats in treating filler complications. Dermatol Surgery. 2015;41 Suppl 1:S347-53.
37. Rao V, Chi S, Woodward J. Reversing facial fillers: interactions between hyaluronidase and commercially available hyaluronic-acid based fillers. J Drugs Dermatol. 2014;13(9):1053-6.
38. Artzi O, Loizides C, Verner I, Landau M. Resistant and recurrent late reaction to hyaluronic acid-based gel. Dermatol Surg. 2016;42(1):31-7.
39. Glaich AS, Cohen JL, Goldberg LH. Injection necrosis of the glabella: protocol for prevention and treatment after use of dermal fillers. Dermatol Surg. 2006;32(2):276-81.
40. Hwang CJ, Morgan PV, Pimentel A, Sayre JW, Goldberg RA, Duckwiler G. Rethinking the role of nitroglycerin ointment in ischemic vascular filler complications: an animal model with icg imaging. Ophthal Plast Reconstr Surg. 2016;32(2):118-22.
41. Nettar K, Maas C. Facial filler and neurotoxin complications. Facial Plastic Surg. 2012;28(3):288-93.
42. Daines SM, Williams EF. Complications associated with injectable soft-tissue fillers: a 5-year retrospective review. JAMA Facial Plastic Surg. 2013;15(3):226-31.
43. Friedman PM, Mafong EA, Kauvar AN, Geronemus RG. Safety data of injectable nonanimal stabilized hyaluronic acid gel for soft tissue augmentation. Dermatol Surg. 2002;28(6):491-4.
44. Ballin AC, Brandt FS, Cazzaniga A. Dermal fillers: an update. Am J Clin Dermatol. 2015;16(4):271-83.
45. Lemperle G, Gauthier-Hazan N, Wolters M, Eisemann-Klein M, Zimmermann U, Duffy DM. Foreign body granulomas after all injectable dermal fillers: part 1. Possible causes. Plast Reconstr Surg. 2009;123(6):1842-63.
46. Jordan DR, Stoica B. Filler Migration: A Number of Mechanisms to Consider. Ophthal Plast Reconstr Surg. 2015;31(4):257-62.
47. Bisschop C, Bruijn MS, Stenekes MW, Diercks GF, Hospers GA. Foreign body reaction triggered by cytotoxic T lymphocyte-associated protein 4 blockade 25 years after dermal filler injection. Br J Dermatol. 2016 Apr 18. doi: 10.1111/bjd.14674. Pubmed PMID: 27086747.
48. Molina-Ruiz AM, Requena L. Foreign Body Granulomas. Dermatol Clin. 2015;33(3):497-523.
49. Rongioletti F, Atzori L, Ferreli C, Pau M, Pinna AL, Mercuri SR, et al. Granulomatous reactions after injections of multiple aesthetic micro-implants in temporal combinations: a complication of filler addiction. J Eur Acad Dermatol and Venereol. 2015;29(6):1188-92.
50. Shahrabi-Farahani S, Lerman MA, Noonan V, Kabani S, Woo SB. Granulomatous foreign body reaction to dermal cosmetic fillers with intraoral migration. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;117(1):105-10.
51. Sankar V, McGuff HS. Foreign body reaction to calcium hydroxylapatite after lip augmentation. J Am Dent Assoc. 2007;138(8):1093-6.
52. Alijotas-Reig J, Fernandez-Figueras MT, Puig L. Late-onset inflammatory adverse reactions related to soft tissue filler injections. Clin Rev Allergy Immunol. 2013;45(1):97-108.
53. Rodriguez JM, Xie YL, Winthrop KL, Schafer S, Sehdev P, Solomon J, et al. Mycobacterium chelonae facial infections following injection of dermal filler. Aesthet Surg J. 2013;33(2):265-9.
54. Monheit GD, Rohrich RJ. The nature of long-term fillers and the risk of complications. Dermatol Surg. 2009;35 Suppl 2:1598-604.
55. Beer K, Avelar R. Relationship between delayed reactions to dermal fillers and biofilms: facts and considerations. Dermatol Surg. 2014;40(11):1175-9.
56. Dayan SH, Ellis DA, Moran ML. Facial fillers: discussion and debate. Facial Plastic Surg Clin North Am. 2012;20(3):245-64.
57. Dumitrascu DI, Georgescu AV. The management of biofilm formation after hyaluronic acid gel filler injections: a review. Clujul Med. 2013;86(3):192-5.
58. Sun ZS, Zhu GZ, Wang HB, Xu X, Cai B, Zeng L, et al. Clinical outcomes of impending nasal skin necrosis related to nose and nasolabial fold augmentation with hyaluronic acid fillers. Plastic Reconstr Surg. 2015;136(4):434e-41e.
This study was performed at the authors' private practice, São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}