


Marisa Gonzaga da Cunha1; Francisca Daza2; Flávia Cury Rezende3; Carlos D. Apparecida Machado Filho4
Introduction: The treatment of sagging skin in body areas is still a big challenge, as there are few aesthetic procedures aiming to improve it.
The poly-L-lactic acid (PLLA) is an injectable synthetic polymer of the alpha-hydroxy acids family, which injection into the deep dermis or superficial hypodermis induces a local and gradual reaction, with synthesis of new collagen by the fibroblasts and consequent increase of dermal thickness.
Purpose: Evaluate the effects of poly-L-lactic acid on the sagging skin of the body.
Methods: Fourteen patients with sagging in gluteal region underwent two applications of poly-L-lactic acid with a 45 days interval between them. We performed an initial clinical evaluation and after six months of the second application, photos before and after six months of treatment, questionnaires answered by the patient and by the evaluating physician and ultrasound examination of all patients to assess the increase of dermal thickness. The adverse effects observed were also evaluated.
Results: In patient's opinion, 85% presented improvement of general appearance of the skin and 71% noticed improvement of sagging. For the evaluating physician, 100% of patients presented improvement of general appearance of the skin and improvement of sagging, but in different degrees and not proportional to the initial degree of severity. There was no significant side effects in the period evaluated.
Conclusions: The results are promising and should be confirmed with studies with a larger sample size.
Keywords: CUTIS LAXA; SKIN; BUTTOCKS
Beauty and attractiveness are important sociocultural factors that tend to dictate how individuals are judged and accepted by the society.¹ As the world's population progressively ages and cosmetic procedures become increasingly popular, adults of all age and socioeconomic groups seek aesthetic improvement.
Currently, there is a great variety of procedures and materials for the treatment of facial aging, which opens up a series of possibilities and combinations that will have synergistic effects – e.g. the use of different cutaneous fillers at different points in time or of different products in different facial sites. 2 Concomitantly to the improvement of the facial appearance, the search for a perfect body is a concern for most of the population, particularly for women. However, the treatment of sagging skin continues to be a major challenge, since there are few procedures aimed at improving it.
The changes caused by the skin's chronological aging result from the normal physiological process, where there are epidermal, dermal and hypodermic thinning, which in turn are aggravated by photoaging. 1 In addition to aging, several factors contribute to the onset or aggravation of skin sagging, for instance restrictive diets, weight loss, liposuction and post-pregnancy, all of which favor the loss of the skin's elasticity, even in young patients.
Innovative treatments are being constantly developed, however few studies have been published on the treatment of sagging in the body's skin in general. Knowledge of the relationship between the various skin layers – especially that between the dermis and the hypodermis – and the changes they undergo, triggering skin sagging, is crucial for understanding the indications of possible treatments, based on their mechanisms of action. Given that the poly-L-lactic acid's (PLLA) mechanism of action induces a local and gradual reaction that can lead to recovery of the hypodermis and collagen network that were lost during the aging process, the hypothesis of its use for the treatment of general body skin sagging was raised.
Poly-L-lactic acid is an injectable synthetic polymer from the alpha-hydroxy acid family. It is biocompatible and biodegradable, has very low cytotoxicity, 3 and has been used for many years in absorbable surgical suture threads. Once injected, PLLA induces local and subclinical inflammatory response shortly after application, recruiting monocytes, macrophages and fibroblasts. It is then hydrolyzed into lactic acid monomers and eliminated; nonetheless there lingers an increased deposition of collagen produced by fibroblasts, with the resulting increase in dermal thickness. 3.4 It is this fibroplasia that will determine the cosmetic results. 5 Since PLLA is a biostimulating agent that depends on the host's reaction, its effects will not be immediate, and will be observed in a gradual and progressive manner, during the months ensuing its application. 6
The present study was performed at the Cosmiatry Sector, Dermatology Department of the Faculdade de Medicina do ABC (FMABC), in Santo André (SP), Brazil, aimed at analyzing the treatment of sagging skin in the gluteal region with subdermal applications of PLLA. It was approved by the Research and Ethics Committee of FMABC and conducted according to the Good Clinical Practice directives.
The choice for the gluteal region was linked to the fact that it is frequently linked to complaints – even in young patients – often being associated with the presence of cutaneous striae, in addition to the fact that this location is not significantly influenced by muscular sagging – unlike the inner part of the arms, for example, in this age group. The study's secondary objective was to evaluate the influence of improved sagging on the improvement of cellulitis.
Fourteen women between 27 and 37 years of age with complaints of cutaneous skin sagging in the gluteal region were selected.
Inclusion criteria: women with skin sagging.
Exclusion criteria: pregnancy, breastfeeding, vegetarian diet, history of hypertension, diabetes, allergies and skin diseases, previous treatments in the studied area, and weight gain during the study period.
The evaluation was carried out clinically, and the scoring system used in the initial evaluation was as follows:
Skin sagging: (0) absence of skin sagging, (1) little skin sagging, (2) moderate skin sagging, (3) intense skin sagging.
Striae: (0) absence of striae, (1) up to 5 striae, (2) between 6 and 15 striae, (3) more than 16 striae.
Gynoid-lipodystrophy cellulite (GLD) Grade II: (0) absence, (1) mild, (2) moderate, (3) severe.
The total score corresponded to the sum of the evaluated criteria's scores.
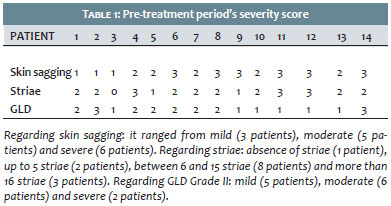
The patients and the applicator physician answered a detailed questionnaire about the local conditions of the skin, presence of striae, sagging, and degree of cellulite before the application. At the pretreatment stage, the degree of sagging ranged from mild (3), moderate (5), and severe (6), and was not correlated to the severity of the striae, due to the fact it was possible to observe that despite the presence of more pronounced sagging in some patients, they had only a few striae. At baseline, 90% of the patients had moderate GLD Grade II in the treated site.
The pre-treatment photographic evaluation was performed in three positions: frontal, dorsal and profile.
Two applications were performed in the gluteal region bilaterally with a 45-day interval, using one PLLA vial in each session. Each vial was diluted two days before in 9 ml of distilled water, leading to a final volume at the moment of the application of 8ml, to which 2ml of lidocaine without vasoconstrictor were added.
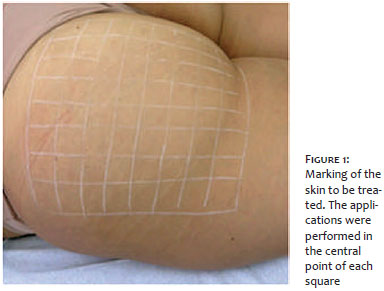
The applications were performed under local anesthesia with anesthetic cream. The skin was marked with squares with sides of approximately 2cm, as shown in Figure 1. A solution volume of 0.04ml per square was applied in the deep dermis-superficial hypodermis, in a puncture made in the center of each square. After the applications, local massage was applied for 5 minutes. The numbers of points of hematoma in the applications sites were recorded.
Six months after the second application, a new clinical evaluation was carried out by the patient and the evaluator physician, using the same questionnaire applied at baseline. The improvement score was as follows:
Absence of improvement (0), little improvement (1), moderate improvement (2), intense improvement (3). The total score corresponds to the sum of the responses to the treatment for each adopted criterion. In addition to the questionnaires answered by the patient and the evaluator physician, ultrasound examinations were performed in the various predefined application points (10 in total), for evaluation of the increase in the skin thickness in the treated areas.
The photographic evaluation was performed in three positions, 6 months after the second application.
The adverse effects were evaluated as follows:
Pain: (0) absence of pain, (1) mild, (2) moderate and (3) intense;
Number of points of hematoma observed after each application: (0) absence of hematoma, (1) up to 3 points of hematoma, (2) from 4 to 7 points of hematoma, (3) more than 8 points of hematoma.
Regarding the answers given in the questionnaires, the initial scores (baseline) of the patient and the applicator physician were equal (Table 1):
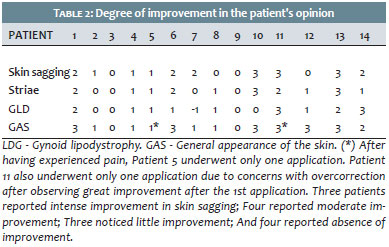
According to the patients' opinion, the improvement score 6 months after the second application (Table 2) indicates that 50% of the participants had moderate or intense improvement:
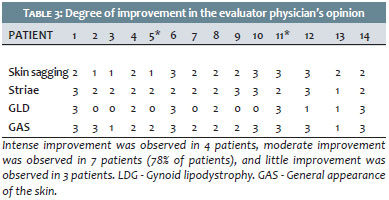
According to the evaluator physician's opinion, the improvement score 6 months after the second application (Table 3) suggests that 78% of the participants reported moderate and intense improvement.
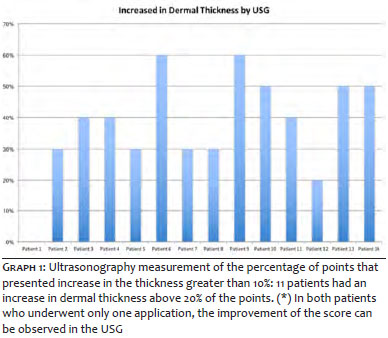
The evaluation of the ultrasonographic examination was expressed in percentage points (Graph 1). The response was considered good only for values that were above 10% of the baseline thickness, as this is the expected intraobserver variation, taking into account the extremely small dimensions of these measurements, despite the fact that the zoom feature has been used aimed at avoiding greater errors. The values presented correspond to the percentage of points that had the thickness increased.
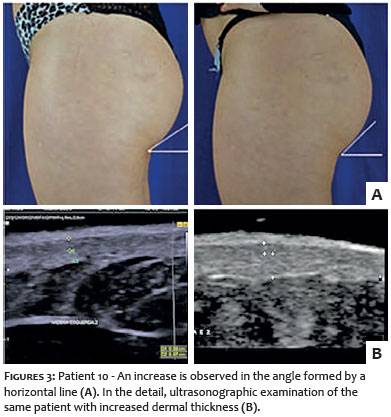
In the photographic analysis, it was possible to observe an increase in the angle formed in the gluteal fold, while the ultrasound examination detected a significant increase of the dermal thickness in 11 patients (Figures 2 and 3)
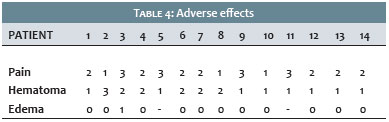
Shows adverse effects and hematoma after the first and second application (Table 4). None of the patients presented newly formed or late nodules.
New and innovative treatments are being constantly developed, however few studies have been published on the treatment of sagging in the body's skin in general.
The changes that take place in the skin's mechanical properties during adult life include the progressive loss of elasticity and an increase in the time required for the skin to return to its original state after being pinched. This process begins after the age of 20, and leads to a significant, linearly steady reduction of the cutaneous thickness over the years. 5 Clinically, the skin seems thinner, drier and less elastic, beginning to wrinkle and fall. These changes in texture can occur associated to changes in color (arising as hypopigmentation or hyperpigmentation areas) and to the emergence of visible vessels in areas exposed to the sun, worsening as a result of the patients' life-style related habits, such as smoking, for instance. 6
The thinning of the dermal thickness observed in chronological aging occurs due to biochemical and structural changes in the properties of the collagen and elastic fibers, and the ground substance, with a reduction in the synthesis of collagen and an increase in its degradation due to increased levels of collagenase. The elastic fibers decrease in number and diameter, and the amount of mucopolysaccharides in the ground substance decreases, especially that of hyaluronic acid, which negatively influences the skin's turgor, in addition to influencing the deposition, orientation and size of collagen fibers. 6 As a result, the dermis becomes thinner and the skin loses elasticity.
Moreover, the reduction of serum estrogen levels in women is also associated with the reduction of the dermal content of collagen, further increasing skin extensibility and reducing elasticity. These changes are more related to menopause than chronological aging, 6 which explains the worsening of sagging in the climacteric. Associated with chronological aging, body skin sagging is aggravated by the presence of striae, which arise due to the rupture of collagen fibers and disorganization of elastic fibers. In addition to the disorganization of extracellular matrix fibers in the dermis, the thinning of the hypodermis caused by the loss of adipose tissue due to aging, weight loss and the practice of high-performance sports (with a reduction of the BMI) manifests in patients by the loose skin sensation. On palpation, the skin feels thin and lacking in consistency, lacking "filling". These changes are observed even in younger patients.
Poly-L-lactic acid is an injectable synthetic polymer of the alpha-hydroxy acid family. It is biocompatible and biodegradable, has very low cytotoxicity, 7 and has been used for many years in absorbable suture. Injections of PLLA into the deep dermis or superficial hypodermis induce local and progressive reaction, with subclinical inflammatory response soon after application, recruiting monocytes, macrophages and fibroblasts. The new collagen begins to form a month after the application and continues to increase during a period varying from 9 months to 1 year. In the 6th month, many PLLA particles become porous and surrounded by macrophages. It is then hydrolyzed into lactic acid monomers and eliminated, however the increased deposition of collagen produced by fibroblasts lingers, resulting in the increase of dermal thickness, 7.8 nevertheless without evidence of fibrosis. 6.7
This fibroplasia determines the aesthetic outcomes and 5 the improvement of skin sagging. Due to the fact it is an stimulating agent, it promotes the production of collagen in the deep dermis, 3which, in turn, will act by increasing the tissular volume progressively, 5.7 possibly leading to the recovery of the collagen network. Its mechanism of action has important implications on how the product should be applied in order to improve outcomes and avoid adverse effects. 9
Given that PLLA is a biostimulating agent that depends on the host's reaction, its effects are not immediate, but will gradually and progressively be observed during the months following its application. 6 Results might not be evident for weeks after the application, and it is important to wait for the biological response to occur between application sessions aiming at avoiding overcorrection. 9 Regarding the face, the literature recommends 2 to 4 applications observing intervals of 30 to 60 days between them. 5.9
It is important to note that the PLLA treatment's final outcome depends on the amount of product used, the age of the patient, the quality of the treated tissue and its ability to stimulate collagen. 5 Loss of cutaneous fat and poor skin quality can be treated successfully, however greater amount of product and number of applications will be required for a satisfactory final outcome. On the other side, younger patients who feel the first signs of cutaneous lipoatrophy, and report skin thinning, usually respond rapidly to the treatment. In this manner, a decision was made for 2 applications with intervals of 45 days between them, as well as for evaluations before (baseline) and 6 months after the second application.
According to the self-assessment, 85% of patients showed improvement in the general appearance of the skin while 71% noticed improvement in sagging. According to the evaluator physician, 100% of patients had some improvement in the general aspect and sagging of the skin, which were confirmed by the photographic evaluation. This fact demonstrates that the patient's perception is not objective and varies according to her or his expectation regarding the treatment.
It is important to highlight that some patients had little or no improvement in sagging, which could be related to the number of applications. As the response is variable and individual, it may be the case that some patients needed a greater stimulus to achieve better outcomes, since the improvement of striae has been observed in almost all patients, a finding that should be considered in future studies.
Regarding GLD (cellulitis), little improvement was observed in general. Nevertheless, one of the patients who had an edematous GLD picture, experienced an important improvement (Figure 4), probably linked to the improvement of skin sagging and striae (Figure 4, detail). Also, a patient who had a hard or fibrous GLD picture, experienced a slight worsening, perhaps linked to the increase in local fibroplasia, evidenced by the improvement in the striae (Figure 4, detail). Therefore, it can not be stated that PLLA is an appropriate treatment for GLD, for it can improve its appearance due to the improvement in skin sagging that is commonly associated with GLD cases with a higher degree of edema, however it can even cause aggravation in the case of GLD with a higher degree of fibrosis.
Reported adverse reactions related to the use of PLLA (such as ecchymoses, hematomas, edema, papules, nodules and granulomas) mainly arise at the sites of product injection. 10,11
The response to treatment occurred in varying degrees and were not proportional to the initial degree of severity. For instance, even bearing a more severe degree of skin sagging, Patient 6 had a better response than Patient 2, who had a mild degree of sagging skin, reinforcing the hypothesis that the clinical response depends on the host and varies from patient to patient.
Regarding the adverse effects observed in the present study, pain was described by all patients, ranging from mild to intense, causing one of the patients to drop out before the second application. As for hematomas, an interesting fact was the improvement in their formation in the second application in 100% of the patients, which may correspond to an improvement of vascular fragility in the treated site. There were no cases of early formation of nodules or late granulomas.
The application PLLA for improving facial skin sagging is already well known, however there are few reports on its use in other body sites.12 In the present study, the authors described a technique for treating skin sagging in the gluteal region with applications in the deep dermis-superficial hypodermis with considerably promising results. These findings should be confirmed by more encompassing studies aimed at better evaluating both the beneficial and adverse effects and ideal number of applications, ideal doses and duration of the results of PLLA injections.
Aknowledgements: We would like to thank Dr. Ayrton Pastore for performing the ultrasound examinations.
1. Langlois JH, Kalakanis L, Rubenstein AJ, Larson A, Hallam M, Smoot M. Maxims or myths of beauty? A meta-analytic and theoretical review. Psychol Bull. 2000; 126(3):390-423.
2. Beer K. Dermal fillers and combinations of fillers for facial rejuvenation. Dermatol Clin. 2009; 27(4):427-32.
3. Lacombe V. Sculptra: a stimulatory filler. Facial Plast Surg. 2009 May;25(2):95-9.
4. Tan CY, Statham B, Marks R, Payne PA. Skin thickness measurement by pulsed ultrasound: its reproducibility, validarion and variability. Br J Dermatol. 1982;106(6):657-667.
5. Fitzgerald R, Vleggaar D. Facial volume restoration of the aging face with poly-l-lactic acid. Dermatol Ther. 2011;24(1):2-27.
6. Varani J, Dame MK, Rittie L, Fligiel SE, Kang S, Fisher GJ, Voorhees JJ. Decreased collagen production in chronologically aged skin: roles of age-dependent alteration in fibroblast function and defective mechanical stimulation. Am J Pathol. 2006;168(6):1861-1868.
7. Lam SM, Azizzadeh B, Graivier M. Injectable poly-L-lactic acid (Sculptra): technical considerations in soft-tissue contouring. Plast Reconstr Surg. 2006;118(3 Suppl):55S-63S.
8. Yang J, Liu F, Tu S, Chen Y, Luo X, Lu Z, et al. Haemo-and cytocompatibility of bioresorbable homo- and copolymers prepared from 1,3-trimethylene carbonate, lactides, and epsilon-caprolactone. J Biomed Mater Res A. 2010;94(2):396-407.
9. Bauer U, Graivier MH. Optimizing injectable poly-L-lactic acid administration for soft tissue augmentation: the rationale for three treatment sessions. Can J Plast Surg. 2011;19(3):e22-7.
10. Machado Filho CDS, Santos TC, Rodrigues APLJR, Cunha MG. Ácido Poli-L-Láctico: um agente bioestimulador. Surg Cosmet Dermatol. 2013;5(4):345-50.
11. Rendon MI. Long-term aesthetic outcomes with injectable poly-l-lactic acid: observations and practical recommendations based on clinical experience over 5 years. J Cosmet Dermatol. 2012;11(2):93-100.
12. Coimbra DD, Amorim AGF. Ácido Poli-L-láctico na região medial dos braços. Surg Cosmet Dermatol. 2012;4(2):182-5.
This study was performed at Faculdade de Medicina do ABC (FMABC) - Santo André (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}