


André Luiz Simião1; Marina de Almeida Delatti2; Larissa Mondadori Mercadante2; Amilcar Castro de Matos2; Marcela Baraldi Moreira3
Introduction: In the dermatologic surgery practice, Mohs micrographic surgery is of great value in the excision of cutaneous neoplasias. Nevertheless, in certain types of neoplasia, immunohistochemistry can increase diagnostic accuracy.
Objective: To describe the use of Mohs micrographic surgery associated to immunohistochemistry and evaluate their effectiveness regarding traditional methods.
Method: Mohs micrographic surgery was performed in 5 cases of diverse cutaneous neoplasias. Tissue evaluation with hematoxylin-eosin and immunohistochemistry were carried out intraoperatively.
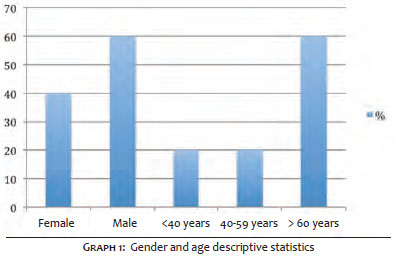
Results: There was greater prevalence of elderly female patients with higher frequency of recurred basal cell carcinomas in the face. In all cases it was possible to perform immunohistochemistry in the frozen specimen. In most cases, primary closure was carried out in the first stage of the Mohs surgery, without postoperative complications.
Conclusion: The combination of the two techniques can increase the procedure's sensitivity, guaranteeing the presence of free margins, leading to fewer recurrences and allowing the preservation of a greater amount of neoplasia-free tissue.
Keywords: MOHS SURGERY, IMMUNOHISTOCHEMISTRY, SKIN NEOPLASMS
Doctor Frederic Mohs pioneered the development of the micrograph surgery concept, in Wisconsin (USA), in 1930. While studying the effect of injecting different substances in neoplasias, he noticed that there was tissue necrosis in the presence of zinc chloride, however the microscopic structure was preserved as if it had been processed according to the anatomopathological routine. As a result, he inferred that the in situ fixation could be used in conjunction with surgical procedures to remove tumors in a microscopically controlled manner. In addition, Dr. Mohs also developed the idea of using frozen horizontal sections – rather than employing the traditional vertical cut – for evaluating 100% of the margins (deep and peripheral), with a higher cure rate. In 1941 he published his first scientific article, describing the treatment of 440 patients during a four-year period, rapidly attracting attention from the dermatological community. In 1951, Dr. Mohs developed the so-called Mohs micrographic surgery ( MMS), in which tumors were removed for subsequent fixation – known as fresh tissue technique. This made the method faster, more tolerable for the patient and offered greater preservation of the healthy tissue, turning it into the gold standard technique for the treatment of some primary or recurrent cutaneous neoplasms. 1
Over the years, this procedure started to be increasingly used, especially after the advent of tissue freezing, becoming the most reliable and more frequently used method for the removal of cutaneous malignancies.2,3
Immunohistochemistry (IH) is a technique used to detect specific antigens based on the use of previously selected antibodies, and can be performed in two ways: directly or indirectly. The direct form is less sensitive, requiring a greater amount of antibodies, consequently being progressively less used. The indirect form requires a lesser amount of antibodies, thus being more efficient, being the most used nowadays. The present study employed the indirect form of IH. 4.5
Since 1980, IH has been incorporated into MMS aiming at lending greater sensitivity to the method, since it makes easier to interpret the anatomopathological results, nevertheless it is still little used today. 6 The present study's objective is to demonstrate the applicability, advantages and limitations of immunohistochemistry in MMS. This is the first study in the Brazilian literature to describe the use of that technique – which has application in several types of cutaneous neoplasms – in the dermatology service of a university hospital.
Five surgical cases of patients being treated at a dermatology medical residency service in 2015 were reported. Mohs micrographic surgery was performed in different epithelial and mesenchymal tumors, with the procedure being performed according to the standards required by the technique, where the lesion's excision was followed by mapping, flattening of the fragments, freezing, cutting and preparation of the slides for hematoxylin-eosin (HE) staining, and immunohistochemical study.
Immunohistochemistry was performed in the corresponding specimens using BenchMarck Ultra device (Ventana Medical Systems, Inc. Roche, USA) automated system, and the following markers: AE1 and AE3 (pancytokeratins) for epithelial neoplasms, CD34 for mesenchymal tumors, and enolase for neural evaluation. Once verified the absence of neoplasia in the margins, the corrections of the surgical defects was carried out.
The study was conducted in accordance with the Declaration of Helsinki's ethical principles, which are aligned with the applicable good clinical practices and regulatory requirements. Also, it was performed according with the federal regulations in place and the International Conference of Harmonization (ICH)'s guidelines.
Each patient signed a free and informed term of consent before undergoing the procedures.
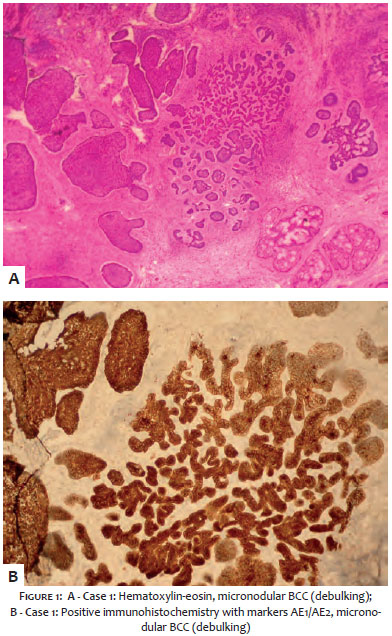
1. Seventy-four male patient (PG) under follow-up in the dermatology service due to various cutaneous neoplasms. In 2015, a new lesion emerged in the left lateral nasal wall: pearly-erythematous plaque, approximately 1.2 cm in diameter, with poorly defined borders and visible telangiectasia, covered by hematic micro crusts, diagnosed as a solid expansive basal cell carcinoma (BCC), after incisional biopsy. A decision was made for using MMS associated with IH for excising the lesion due to its highly sensitive location and poorly delimited margins, in addition to the proximity to previous surgical scar. The neoplasia's delimitation was defined observing 2mm surgical margins, with the lesion's exeresis being carried with preparation of the lateral and deep edges, and subsequent freezing of the specimens. The margins were analyzed with HE staining (Figure 1A) and IH technique using the AE1/AE3 cytokeratins panel. All surgical margins were found to be free of neoplasia after the first MMS' stage. The tumor's debulking was then performed, with subsequent freezing, HE staining, and AE1/AE3 IH, respectively aimed at visualizing the tumor and evaluating the IH of the frozen specimen (Figure 1B). Once all margins were found to be free of neoplasia, the reconstruction of the operative wound was carried out, and the patient was kept under clinical follow up.
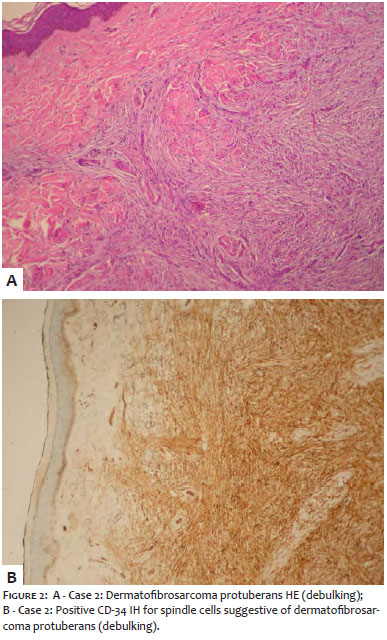
2. Thirty-three years old male patient (TGZ) began to be followed up at the dermatology service in August 2015 due to an asymptomatic lesion that had emerged one year before in his left leg, with progressive growth. The patient had previously undergone exeresis of the lesion (May 2015), with diagnosis of dermatofibrosarcoma protuberans. The dermatological examination evidenced an infiltrated, well delimited brownish plaque measuring 1cm. The diagnosis hypothesis of recurrent dermatofibrosarcoma protuberans was then raised, with a decision having been made for using MMS, which is deemed the gold-standard procedure for the treatment of this type of neoplasia. The lesion exeresis was performed with 1cm margins, with the specimen being divided into eight fragments. In the freezing and subsequent HE staining, the fragments were found to be free of neoplastic involvement, with only one MMS stage being needed, followed by primary closure (Figure 2A). Tumor debulking was then carried out, with freezing, HE staining, and CD34 IH, respectively aimed at visualizing the tumor and performing the IH analysis of the frozen specimen (Figure 2B).
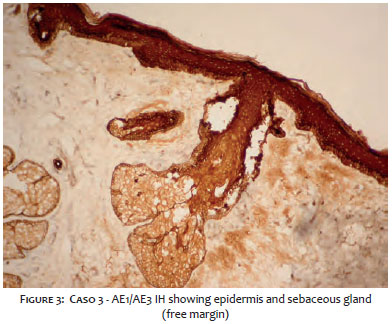
3. A sixty-six year-old female patient (PSL) being followed up at the dermatology service due to multiple actinic keratoses, was found to be bearing an pearly-erythematous 0.8cm papule with central ulceration in the right nasal wing, after a dermatological examination in July 2015. An incisional biopsy resulted in methatypic CBC with squamous differentiation. Due to the prime location and histologic subtype of the neoplasia, the patient was referred to MMS. Surgical margins of 2mm were defined and divided into four fragments, all of which were found to be free of neoplasia in the first stage. Pancytokeratins AE1 and AE3 based IH also did not evidenced tumor involvement in the margins (Figure 3). The reconstruction of the postoperative wound was performed via a transposition flap.
4. A 74 years old female patient (MCC) was referred to the dermatology service with a lesion in the left malar region and infiltrative BCC diagnosis after incisional biopsy underwent MMS. The margins were found to be free from neoplasia after the first stage, however large cells were visualized in margin B that were submitted to IH for confirmation of its histogenesis. Antibodies AE1/AE3 were negative in B's topography, leading to the conclusion that the surgical margins were free of cancer. The operative wound underwent primary closure.
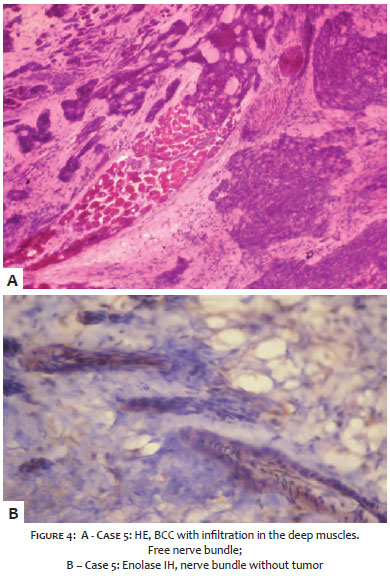
5. A 47 year-old female patent (MCGS) was referred to the to dermatology service for clinical follow up after the complete exeresis of a solid and sclerodermiform BCC with neoplastic infiltration up until the deep dermis and perineural invasion, located in the left hand side epicanthus. The initial dermatological examination only evidenced a scar with good aspect and no signs of recurrence. Nonetheless, three months after, an infiltrated, hardened, plaque with telangiectasia and measuring 1cm emerged in the medial region of the scar. The diagnosis of recurred BCC was hypothesized and a three-point incisional biopsy was performed. The anatomopathological examination showed an infiltrative BCC reaching the deep skeleton muscle tissue (Figure 4A). Due to the fact that deep tissues were found to be affected, MMS was performed in two stages, for the margins A, C and F were compromised in deep planes, demanding expansion. Immunohistochemistry was carried out with enolase aiming at evidencing the nerve bundle, which was found to be free of neoplastic involvement (Figure 4B). The surgical defect was corrected by direct closure.
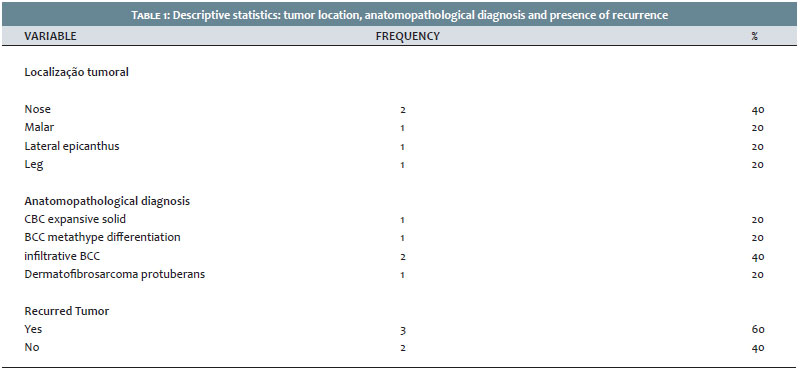
Five male and female patients aged between 33 and 74 years old, were treated due to different skin neoplasms. It was possible to observe a higher prevalence in females with over 60 years of age (Graph 1). The most frequent location was the nose, with 80% of the neoplasms being located in the face and absence of postoperative complications in all cases. Histological diagnosis of infiltrative BCC was the most common, with 3 recurrent and 2 primary neoplasms (Table 1). The only surgery that required two MMS stages was that of a recurrent tumor, with most cases undergoing primary closure in the first stage. Regarding the immunohistochemical markers, decisions were made for the use of AE1/AE3, CD34 and enolase (Table 2). The possibility of using different immunohistochemical markers in the frozen specimens was demonstrated in the present pilot study, demonstrating the possibility of further increasing the sensitivity and effectiveness of free margins.
Mohs micrographic surgery is a surgical technique consisting in initially delimiting the clinical margins of the tumor, subsequently delimiting those of the surgical margins, with a distance equal or greater than 2mm. The surgical specimen is divided in fragments and mapped for correct spatial orientation during its analysis. The fragment undergoes flattening in a way to allow the complete visualization of the epidermis and dermis in a single plane. Next, the tissues are frozen and the slides are prepared for histological evaluation, stained with HE, which is used for all cutaneous neoplasms. 3.7
Once these procedures have been carried out, the dermatologic surgeon evaluates the slides in order to access the involvement of the margins. If the margins are found to be free of neoplasia, the reconstruction of the surgical defect can be performed immediately. In case the margins (both lateral and deep) are found to be compromised, new expansions are progressively performed up until all margins can be considered free of neoplasia. In this manner, the MMS technique allows complete histological control, with the evaluation of 100% of the margins. 3.7
Indications for MMS are: recurrent tumors; incompletely excised tumors; non melanoma skin tumors greater than 0.4 cm located in areas with high risk of local recurrence (central facial, periocular, periauricular); tumors located in areas where tissular preservation and high cure rates are important; tumors with poorly defined clinical margins; tumors with aggressive histological subtypes (micronodular, infiltrative, squamous or sclerodermiform BCCs, and SCC) or with evidence of perineural and perivascular invasion; tumors located over irradiated areas or scars; tumors in prime areas such as genital, anal, hands and feet; expanding tumors in immunosuppressed patients; in patients genetically predisposed to develop multiple skin cancers (xeroderma pigmentosum, Gorlin-Goltz syndrome). 3,4,7
Immunohistochemistry is a laboratory technique used to detect specific antigens in tissue sections that can be performed in two ways. The original or direct method allows that a single antibody, previously conjugated to an enzyme, interact with the antigen present in the target cell. A substrate is then added, which reacts with fluorescence when in contact with the enzyme. This method requires high concentrations of antibodies, which decreases sensitivity. In the indirect method, the primary antibody binds to a specific antigen. A second antibody previously conjugated to an enzyme is then added and subsequently bound to the primary complex. A substrate is then added and, when in contact with the enzyme, fluoresces. As a result, a smaller concentration of antibodies is required, which increases the method's sensitivity and efficacy. 4.5 From 1980, IH was incorporated into MMS, since it allowed recognizing neoplastic cells more easily. Its applicability is however limited due to its protracted preparation, requiring longer surgical times. Moreover, it is expensive, there are few trained professionals who are able to perform it, and the literature about it is scarce. 6 This theme has been increasingly studied by many researches over the past 20 years, and more medical schools have gained know-how in order to provide training on the technique. As a result, the role of IH in MMS has been established, with the number of procedures in which it is used having doubled during the last decade. In addition, it has been proved that the freezing technique preserves the antigenic content, increasing the antibodies' ability to identify and trace antigens (tumoral cells). 5.6
Currently, a number of markers can be used in the IH technique depending on the type of tumor in question. Examples are: Melan-A, S100, HMB45, cytokeratins, among others. 2,4,5
The advantages of immunohistochemistry in MMS are linked to the increased ability to identify tumor cells, including more difficult cases, such as those whose neoplasms mimic normal structures or are intertwined with the dense inflammatory process or fibrotic tissue, and those with perineural invasion. It also provides a more accurate identification of free and compromised surgical margins, leading to a decrease in recurrence rates and unnecessary removal of healthy tissue. 2.5
Disadvantages include a longer implementation time and multiple steps required in the process of staining the tissues, in addition to the high cost and short shelf life that common reagents have. Increasing the number and improving the expertise of professionals in Mohs laboratories, including technicians and surgeons, as well as expanded waiting times for patients also are limiting factors. 2 Trimble et al 6 conducted a study in which accredited Mohs surgeons listed the main reasons for not using IH, which were, in order of appearance: increased surgical time, lack of training and high cost.
Nowadays, one of the main focuses of research in this field has been the reduction the time required by the staining process and of the surgery as a whole. Research show that swift protocols (up to 30 minutes) have already been developed and offer effectiveness levels similar to those of more traditional protocols (one hour on average), without compromising the method's reliability. 8.9
The use of IH in MMS is unquestionably expanding, however more studies are still needed. The use of staining in frozen sections has been shown useful in the various types of cutaneous neoplasias, leading to an increase in the number of detections of tumor cells, nevertheless this in turn calls for an increase in the number of teams that are proficient in the technique.
Immunohistochemistry allows expansion and growth in the applicability of MMS, especially in tumors of difficult histological delimitation. As a result, it increases the sensitivity for the identification of tumor cells, making it possible to preserve a greater amount of healthy tissue and decrease recurrences, offering a higher quality treatment to patients.
1. Trost LB, Bailin PL. History of Mohs Surgery. Dermatol Clin. 2011;29(2):135-9
2. Stranahan D, Cherpelis BS, Glass LF, Ladd S, Fenske NA. Immunohistochemical stains in Mohs surgery: a review. Dermatol Surg. 2009;35(7):1023-34.
3. Benedetto PX, Poblete-Lopez C. Mohs micrographic surgery technique. Dermatol Clin. 2011;29(2):141-51.
4. El Tal AK, Abrou AE, Stiff MA, Mehregan DA. Immunostaining in Mohs micrographic surgery: a review. Dermatol Surg. 2010;36(3):275-90.
5. Thosani MK, Marghoob A, Chen CS. Current progress of immunostains in Mohs micrographic surgery: a review. Dermatol Surg. 2008;34(12):1621-36.
6. Trimble JS, Cherpelis BS. Rapid immunostainig in Mohs: current applications and attitudes. Dermatol Surg. 2013;39(1 Pt 1):56-63.
7. Reis NA, Azevedo LCM, Stolf HO, Nouri K, Kimyai-Asadi A, Goldberg LH. Cirurgia micrográfica de Mohs. Surg Cosmet Dermatol. 2011;3(3):227-31.
8. Cherpelis BS, Turner L, Ladd S, Glass LF, Fenske NA. Innovative 19-minute rapid cytokeratin immunostaining of nonmelanoma skin cancer in Mohs micrographic surgery. Dermatol Surg. 2009;35(7):1050-56.
9. Cherpelis BS, Moore R, Ladd S, Chen R, Glass LF. Comparison of MART-1 frozen sections to permanent sections using a rapid 19-minute protocol. Dermatol Surg. 2009;35(2):207-13
This study was performed at the Pontifícia Universidade Católica de Campinas (PUC-Camp) – Campinas (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}