


Cristiane Comparin1; Bruna Costa Santos2; Milena Marchini Rodrigues2; Carlos Alberto Ferreira de Freitas3; Gunter Hans Filho4
Basal cell carcinoma is the most frequent malignant skin tumor. Its incidence has been increasing, leading to the emergence of a public health problem. The common delay in seeking treatment hampers tumor removal. The objective of this paper was to report a case of two synchronous basal cell carcinomas on the face and the challenge of their surgical resolution. Good aesthetic and functional outcomes were obtained using the rotation flap technique and a complex reconstruction of the hemiface. Surgical reconstruction constitutes a challenge for the surgeon, who should prioritize the oncologic cure while preserving the functionality and aesthetic appearance, when possible.
Keywords: CARCINOMA, BASAL CELL; SURGICAL FLAPS; SKIN NEOPLASMS
Basal cell carcinoma (BCC) is the most common malignant skin tumor in the world. Its incidence is increasing and emerging as a public health problem.1,2 The search for care and treatment is often delayed, making it difficult to remove the tumor.3
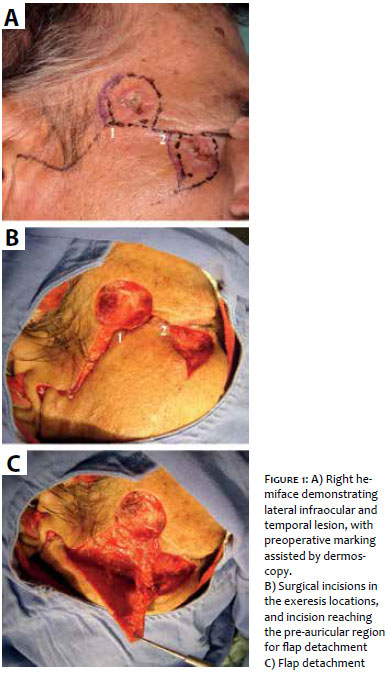
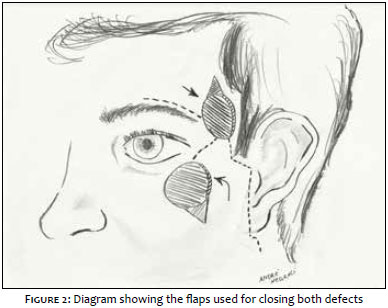
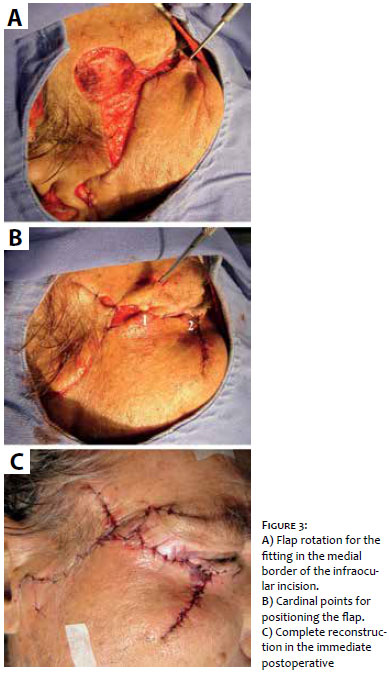
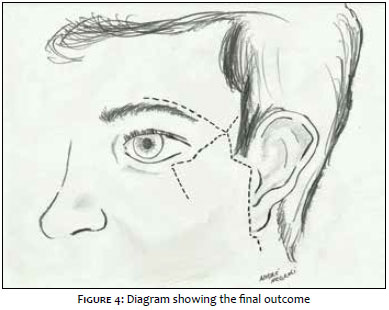
A 70 year-old male patient reported the emergence of two lesions in the right hemiface roughly three years before. The physical examination revealed two erythematous lesions with infiltrated borders, ulcerated center and inaccurate limits in the right temporal and right lateral infraorbital regions (including part of the lower eyelid), both measuring 2cm in their longest diameters. The previous biopsy revealed nodular BCC. Planning was carried out for the exeresis of both lesions in a single surgical time, with preoperative margins being demarcated with naked eye, followed by dermoscopy, which allowed the re-marking of the lateral margins of the two lesions due to the presence of arboriform telangiectasia extending beyond the previously demarcated margins. The two lesions were then excised under local tumescent anesthesia, with minimum margins of 5mm. Flaps were used for the closure using the following technique: the infraorbital defect was closed with a malar flap (Mustardé) by laterally extending the incision along the lower eyelid's line up until the temporal area's defect, uniting them in the same direction, up until the hair line; this incision then run inferiorly, passing in front of the auricular pavilion, to reach the cervical region. The detachment of this flap – as is done in rhytidectomy – and its rotation allowed the closure of the infraorbital defect and the reconstruction of the lower eyelid, in addition to covering part of the temporal area (Figure 1). The closing of the latter, was then completed with the lateral advancement of the eyebrow region's skin, which was incised in the upper line of the eyebrow (Figure 2). The immediate outcome can be seen in Figures 3 and 4. The sutures were performed in a single plane in the skin, with simple stitches and nylon threads, which were removed 10 days after. The histological examination of the parts indicated the presence of ulcerated, nodular subtype BCC, with 5mm free peripheral margins. There was total healing and tissue integration, with good aesthetic and functional results.
The body site with greatest incidence of BCCs is the face, and the first choice treatment is exeresis.1,4 In this location, not only the cure is necessary but also the attempt to preserve the facial aesthetics.1 In some cases, the tumor's size or the presence of more than one lesion close to one another turns oncologic surgery into a challenging procedure.1
The surgical margins were demarcated using dermoscopy – which is a trend in dermatologic surgery – and may have contributed to the excision of both lesions with free margins, since studies suggest that the rate of complete excision of BCCs increases to 98.5% from 95% when dermoscopy is employed.5,6
On a smaller scale, the surgery described resembles the east west flap, mainly used in resections of nasal tumors.5 The temporal region is a risk area, where the resection should be careful and aimed at preventing that the surgical plan be deepened, thus avoiding damage to the temporal nerve.3 The infraocular area is delicate implying that there should be concern with ectropion formation in the postoperative period, especially in the case of extensive flaps in this region.3 It is possible to perform advancement flaps or lateral rotations so that this complication be minimized or avoided, as was done in the case described.3
Surgical reconstruction is challenging for the surgeon, who should prioritize the oncologic cure while preserving the functionality and aesthetic appearance when possible. The choice of technique should be adequate and individualized for each tumor type, location, skin elasticity and overall condition of the patient. In the authors' experience, the combination of techniques allowed the complex combined excision of two synchronous BCC lesions of large dimensions, in areas next to each other in the face. The excisions were performed in the same surgical time, providing satisfactory functional and aesthetic outcomes, in addition to allowing the prompt return of the patient to his social life.
1. Telfer NR, Colver GB, Morton CA. Guidelines for management of basal cell carcinoma. Br J Dermatol. 2008;159(1):35-48.
2. Pereira PMR, Rodrigues CAC, Lima LL, Romero SAR, Mariano AVO. Reconstruction of the lower lip with Camille Bernard's technique after excision of infiltrative basal cell carcinoma. Surg Cosmet Dermatol. 2013;5(1):81-3.
3. Caresana G, Giardini R. Dermoscopy-guided surgery in basal cell carcinoma. J Eur Acad Dermatol Venereol. 2010;24(12):1395-99.
4. León H,Lima A, Rojas JC, Ramirez M. Colgajos en la reconstrucción facial en dospacientes con carcinoma basocelular. Rev Venez Oncol. 2011;23(2):100-1.
5. Geist DE, Maloney ME. The "east-west" advancement flap for nasal defects: reexamined and extended. Dermatol Surg. 2012 ;38(9):1529-34.
6. Comparin C, Freitas CAF, Hans-Filho G. Dermatoscopy as a tool in the detection of presurgical margins of basal cell carcinomas. Rev Bras Cir. Cabeça Pescoço. 2013;42(1):47-52.
The present study was performed the Dermatology Service of the Hospital Universitário de Taubaté -Taubaté (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}