


Paulo Morais1; Paulo Santos2
W-plasty is a commonly used technique in facial cosmetic surgery to camouflage the straight line of a scar into a regularly irregular pattern. It consists of excising a series of consecutive small triangles of skin on each side of the scar, and imbricating the resultant triangular flaps, producing a "zig-zag" effect. This procedure is particularly useful on long, wide, curved, contracted, or anti-tension line scars of the forehead, cheeks, chin, and nose. We report the usefulness of this technique in an unaesthetic postsurgical facial scar.
Keywords: CICATRIX; DERMATOLOGIC SURGICAL PROCEDURES; SURGICAL FLAPS; RECONSTRUCTIVE SURGICAL PROCEDURES
Scar formation is an inevitable consequence of the healing process, which can either result from surgical procedures or trauma.1 In oncologic surgery, the complete removal of the tumor and the aesthetic appearance of the scar are critical criteria in the assessment of the surgical outcome. The surgeon's experience, a careful surgical planning and the implementation of the correct technique, combined with knowledge of anatomy and the healing process, are central to improve surgical outcomes and reduce complications risks.1-3 The revision of a scar does not eradicate it, nevertheless it helps to make it less obvious and cosmetically/functionally more acceptable through transforming several variables by: softening irregular scars; improving the color; filling depressions; reorienting, narrowing or flattening the scar; or correcting anatomic units distortions.2 Aimed at achieving those effects, different surgical techniques (Z-plasty, W-plasty, closure with geometric broken line, V-Y and Y-V advancement flaps, debulking among other) as well as non-surgical techniques can be used (corticosteroids injections, dermabrasion and treatment with ablative and non-ablative lasers), alone or combined, depending on the advantages, limitations and risks of each of them.1,3 When planning the revision of a scar, the surgeon must decide on the appropriate timing to intervene and the technique to be used in order to obtain an aesthetically agreeable outcome.1
A 38 year-old male patient had undergone excision of a basal cell carcinoma located in the mentum three years before, with a nasolabial fold transposition flap being used in the closure (Figure 1A, 1B and 1C). Two hypertrophic, elongated, wide and curved scars, perpendicular to the relaxed skin tension lines (RSTL) resulted from the procedure (Figure 1D). The scars were aesthetically unsightly, and became the cause of significant emotional stress and social impact. The patient accepted the proposal of surgical correction of the scars using the W-plasty technique. After local anesthesia with 2% lidocaine with 1:100,000 epinephrine, small triangular interdigitated skin flaps (in the shape of "Ws") were drawn on each side of the scar, so that the two sides could be interposed after the excision of the scar and detachment of the flaps (Figures 1E, 1F and 1G). The triangles' borders were approximately 5mm long (with one of them oriented parallel to the RSTL) and the vertices' angles measured less than 30°. The closure was carried out with synthetic nonabsorbable synthetic suture thread (Polyamide) 5.0 (Figure 1H). The final outcome achieved was deemed cosmetically good by both the patient and the physician, and there was absence of complications (Figure 1I).
The W-plasty is a relatively simple to plan and implement technique, consisting of the excision of the old scar and closure of the surgical wound by re-approximating the small interdigitated borders created, creating a zigzag pattern. Its concept is based on the principle that an irregular line is less visible than a straight line, which is especially advantageous when the scar is not oriented along the RSTL. It is also indicated for scars located on curved surfaces – such as the jaw – or in cavities, wide scars or in scar that have stitch marks similar to a train tracks, as well as to dissipate contracture forces and prevent further cicatricial retractions.2,4 It should be implemented in body sites where there is adjacent loose tissue – such as in the forehead, temporal regions, cheeks or mentum.2 There is no elongation of the scar and the tissue is removed, resulting in an increased tension in the area perpendicular to the scar.4
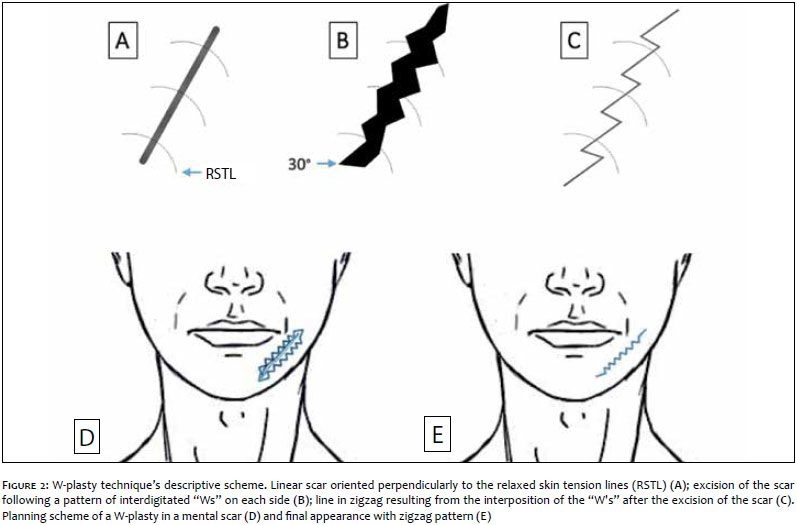
In detail, the W-plasty technique consists of (Figure 2):
1. Drawing a zig-zag ("Ws") on one side of the scar and another mirror image on the opposite side. The "Ws" will function as triangular advancement flaps, with their vertices oriented parallel to the RSTL, given that the scar is perpendicular to them.2,3,5
2. Drawing the "Ws" so that the angles measure at least 60°, and the tips of the triangles lie between 3 to 7 mm from the periphery of the scar, allowing that an irregular line be abtained.3 In order to avoid the dog-ear effect, it is essential that the end portion of the plasty be designed in a way to originate a 30° angle at each extremity (Figure 2B).2,3,5
3. Excising the scar along the drawn lines and re-approximating the borders in a way that the tips of the triangular flaps interdigitate and generate a single line in zigzag (Figure 2C).
This case highlights the W-plasty's usefulness to correct cosmetically unsatisfactory scars as well as the importance of post-surgical aesthetic outcome for the patient and the physician. The authors' experience with this scar revision technique shows that if correctly implemented in properly selected cases, it is possible to achieve a marked improvement in the scar's appearance, making it less noticeable. However, the benefit of Wplasty is reduced in long scars since the regular repetitive pattern (zig-zags) can lend enhanced evidence to the scar.2,5 In these cases it is preferable to use the geometric broken line technique of correction.
1. Garg S, Dahiya N, Gupta S. Surgical scar revision: an overview. J Cutan Aesthet Surg. 2014;7(1):3-13.
2. Shockley WW. Scar revision techniques: z-plasty, w-plasty, and geometric broken line closure. Facial Plast Surg Clin North Am. 2011;19(3):455-63.
3. Pérez-Bustillo A, González-Sixto B, Rodríguez-Prieto MA. Surgical principles for achieving a functional and cosmetically acceptable scar. Actas Dermosifiliogr. 2013;104(1):17-28.
4. Lorenz P, Bari AS. Prevenção de cicatriz, tratamento e correção. In Neligan PC, Gurtner GC (editoress). Cirurgia Plástica: princípios. 3ª ed. Rio de Janeiro: Elsevier, 2015.
5. Rodgers BJ, Williams EF, Hove CR. W-Plasty and geometric broken line closure. Facial Plast Surg. 2001;17:239-44.
The present study was performed at the Dermatovenereology Service of the Centro Hospitalar São João - Porto, Portugal.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}