


Eduardo Figueiredo Gatti1; André Cesar Antiori Freire Pessanha2; Denise Steiner3; Gabriela Momente Miquelin1; Mariana Morais Tavares Colferai1; Camila Carneiro Marques1
Introduction: Mohs micrographic surgery is a technique that offers high cure rates for non-melanoma skin cancer.
Objective: To describe the clinical and epidemiological profile of patients who underwent Mohs micrographic surgery in a reference center in dermatologic surgery.
Methods: Medical records of patients who underwent Mohs micrographic surgery in the period 2014-2015 at a dermatology reference center, in the city of Mogi das Cruzes (SP, Brazil), were analyzed.
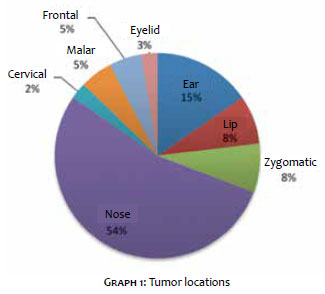
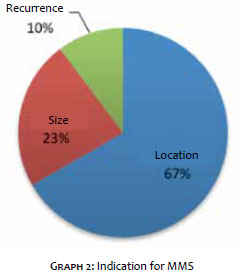
Results: The patients' ages ranged from 38 to 87 years; of these 54% were women. The most affected topography was the nose (54% of patients). Previous history of skin cancer was positive in 62% of cases. The indication driver for micrographic surgery was the lesion's location in 67% of the patients, followed by the size (23%) and tumor recurrence (10%). The most prevalent intraoperative diagnosis was basal cell carcinoma (90%).
Conclusions: Mohs micrographic surgery is an excellent therapeutic option in cases of tumors of aggressive nature, large diameter and high-risk location. This study is in line with the current literature regarding the epidemiological data linked to the occurrence of nonmelanoma skin cancer.
Keywords: MOHS SURGERY; SKIN NEOPLASMS; DERMATOLOGIC SURGICAL PROCEDURES
Mohs micrographic surgery (MMS) is the technique used to treat non melanoma cutaneous malignant neoplasias that leads to the best cure rates and is today regarded as the gold standard.1,2 In this procedure, the dermatologic surgeon performs the mapping of the neoplasia, and the removal and histological analysis of the tumor and its margins.1
Frederic Mohs developed the first concepts of micrographic surgery in 1930, studying the potential curative effect of various substances injected into different neoplasms. During an experiment, there was tissue necrosis after the injection of 20% zinc chloride solution. Microscopic analysis evidenced that the tissue maintained its microscopic structure, as if it had been excised and processed for routine histological examination. With this, Dr. Mohs observed that the in situ fixation was effective,1 enabling the development of a surgical technique in which the tumor could be removed in a staged way. After undergoing in situ fixation, the tumor was excised and then cut into tangential sections, which allowed the analysis of both the epidermis and the deep tumoral region.3 In contrast with the traditional section, which evaluates only 0.001% of the total sample's surface, the horizontal sections used in this technique allowed analysis of 100% of the sample's margins.1
Mohs tested many substances for in situ fixation, and zinc chloride was chosen due to the facts that it preserved the microscopic characteristics for analysis, had good penetration in the tissues with precise control of the fixation's depth, did not interfere with the healing of the exeresis' site by secondary intention, did not cause systemic toxicity, was safe during use and had no smell.1
Initially, Mohs named the technique as microsurgery, however this term was already employed to describe the dissection of small structures using a microscope; the term chemosurgery was then chosen, since skin tumors were chemically fixed in situ before excision.4
Although this technique had a higher healing rate than that of the traditional excision technique, it had some drawbacks: it could take days to complete, it could cause pain, fever, lymphadenopathy in tumors of large diameter, and the detachment of the fixed tissue could take days to complete, which delayed the surgical wound reconstruction.1
Due to these drawbacks, the in situ fixation was gradually replaced by the fresh tissue technique, with the use of freezing after the tumor's excision, which has been described by Theodore Tromovitch and Samuel Stegman. As a result, Mohs also adhered to it.1,4
The fresh tissue technique eliminated the need for zinc chloride, allowing the tumor's removal and reconstruction to be performed on the same day, without having to wait for the crust caused by the zinc chloride to detach from the viable underlying tissue. Thus, in situ fixation (chemosurgery) fell into disuse, giving way to the currently used technique based on fresh tissue (Mohs micrographic surgery - MMS).
The conventional excision technique usually leaves a margin of 3 to 6mm beyond the tumor. The histological margins are then evaluated by the pathologist by sampling, which can lead to evaluation flaws. In MMS, the superficial and deep margins are fully evaluated.5
The five-year recurrence rates of primary and recurrent basal cell carcinomas (BCCs) treated with conventional surgery are 10% and 17%, respectively. When treated using MMS, those rates drop to 1% and 6%; 6 another significant advantage is that the technique allows greater conservation of normal tissue. In this manner, it is clearly indicated for tumors that are large in diameter, recurrent, have aggressive histological subtypes or are located in critical areas (periocular, periauricular and nasal regions).
In order to perform the MMS, the following pieces of surgical material are needed: dieresis, hemostasis and synthesis materials (the same used for conventional excision), pen for marking the surgical margins, histological stains, specimen processing material, a cryostat, a microscope and, in addition, the assistance of a laboratory technician to stain and perform the cuts in the specimen.
The technique has five steps:
1) Marking of the area to be excised: delineate the clinical margins of the tumor with a pen and then the surgical margins with a distance varying from 2 to 5mm from the clinical margins. Perform the markings transversally to the incision line, which will allow to locate the position of the removed fragments in the tissue surrounding the surgical wound.
2) Excision of the tumor: it is performed using a scalpel at a 45º-degree angle, which allows the epidermis and dermis to be cut straight in the cryostat, allowing microscopic analysis in the same plane.
3) Mapping of the specimen: can be carried out using a sheet of paper or digitally on devices that take photographs and allow drawing on that image (e.g. tablets). The surgical specimen and its location should be drawn in the area of the surgical defect. Its divisions and the ink markings should also be outlined. This map is crucial for the dermatologic surgeon's directing during the analysis of the tissue using the microscope and for the exeresis of the areas compromised with the tumor.
4) Processing and histological analysis of the specimen: in this phase, the specimen's marking with ink, flattening, freezing, cutting and staining must be performed.
The division of the specimen, when necessary, as well as the marking with ink must always be indicated on the map. The most frequently used ink for the specimen's marking is nankin, which comes in several colors, allowing highlighting each region.
The flattening of the surgical specimen can be performed using mechanical pressure on it, while cuts with a scalpel are required in some cases. The flattening on the slide is critical so that the whole of the epidermis and dermis can be cut in a single plane in the cryostat.
The tissue is then frozen and sectioned in the cryostat, with the slides being prepared with hematoxylin-eosin for histological evaluation.5
The surgeon evaluates the slides in order to determine whether the margins are compromised. If the tumor is completely excised, the surgical defect can be immediately reconstructed. Nevertheless, if the tumor is still present, the corresponding location is marked on the map.
5) Selective excision of the areas with residual tumor: it is necessary to go through this step in case there is compromise of any portion of the margin. If the lateral margin is compromised, a 1-2mm excision should be performed at this site. If the deep margin is compromised, an excision should be performed along the defect's interior, removing tissue from the deep base of the wound.
The tissues of the compromised areas must undergo histological analysis. These steps are repeated until the margins are considered free of tumor and the reconstruction can be performed.5
The objective of the present study was to describe the clinical and epidemiological profile of the patients who underwent MMS at a dermatological surgery referral center.
The present study was approved by the Universidade de Mogi das Cruzes – UMC (SP, Brazil) Research Ethics Committee on 22/06/2016 under the protocol number 55945216.8.0000.5497.
A retrospective, descriptive, observational cross-sectional study analyzed medical records of all patients who underwent MMS at the dermatology referral service in the city of Mogi das Cruzes, São Paulo, Brazil, in the years of 2014 and 2015.
The sampling method was non-probabilistic for convenience, and included all patients who underwent MMS during the study period.
Aimed at grouping the study data into clinical, epidemiologic and histologic categories, the following items were analyzed for each case: gender, age, preoperative biopsy diagnosis, intraoperative biopsy diagnosis, MMS indication, tumor location, previous history of skin cancer, photodamage degree (mild, moderate or severe), Fitzpatrick phototype (I, II, III, IV, V, VI), number of phases in each surgery, number of fragments of each tumor excised during surgery, and final surgical defect reconstruction type.
The obtained data were recorded on Microsoft Excel® spreadsheets, with descriptive analysis of percentages and graphs.
During the study period, 39 patients were treated and operated using MMS, and had their medical records analyzed. Of these, 54% were female. The participants' ages ranged from 38 years to 87 years, with an average of 60.8 years.
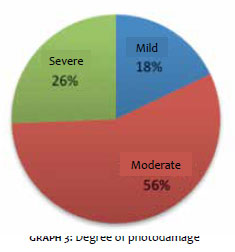
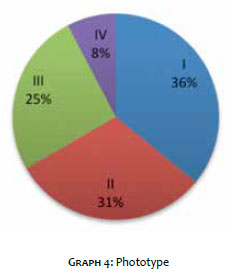
Regarding the lesion's topography, the most affected body sites were the nose (54%) and the ear (15%), as depicted in Graph 1. Previous personal history of skin cancer was present in 62% of the patients. The indication for MMS was due to the lesion's location in 67% of patients, as shown in Graph 2. The degree of photodamage was classified as moderate or severe in most patients, as shown in Graph 3. Graph 4 illustrates the treated patients' phototypes' percentages, according to the Fitzpatrick Scale. Most of the sample's individuals had phototypes I and II (i.e. fair skin).
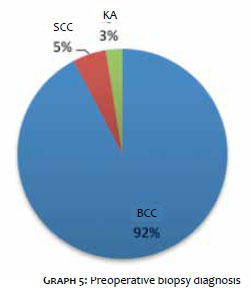
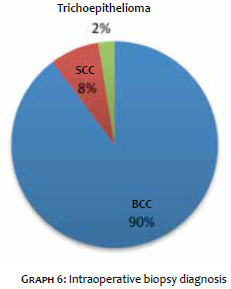
Thirty-nine lesions – one of each studied patient – were excised. Of these, 92% were diagnosed with preoperative BCC biopsy; squamous cell carcinoma (SCC) and actinic keratosis (AK) were present in a much lower proportion (Graph 5). In the intraoperative diagnosis, 90% of the lesions were confirmed as BCCs, 8% SCC and 2% were trichoepitheliomas (Graph 6), indicating diagnostic disagreement in 2 lesions of the 39 evaluated. A lesion preoperatively diagnosed as an AK was proven a clearly differentiated SCC in the intraoperative biopsy. Another initially diagnosed as a BCC, was proven a trichoepithelioma in the intraoperative biopsy.
Surgeries had one, two or a maximum of three operative phases, with an average of three phases. Each surgery yielded on average 4.4 tissue fragments during the excisions, having been prepared and analyzed intraoperatively.
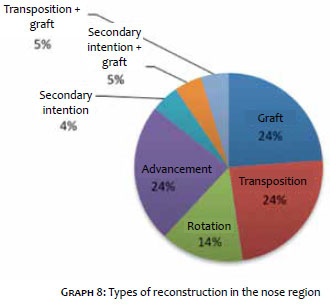
In the nose region, 90% of the tumors were BCCs, 5% SCCs, and 5% trichoepitheliomas (Graph 7), and most reconstructions in this area were performed with transposition flaps (Graph 8).
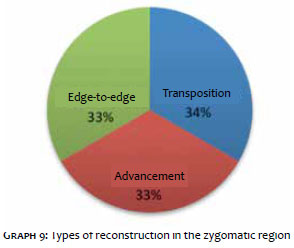
In the zygomatic region, 67% of the tumors were SCCs and 33% were BCCs; 34% of the reconstructions were performed with transposition flaps, and edge-to-edge closures and advancement flaps were performed in 33% of the cases in this area (Graph 9).
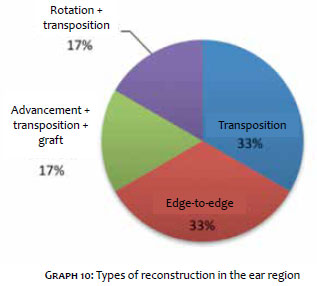
In the ear region, 83% were BCCs, and 17% SCCs, with edge-to-edge reconstruction and transposition flaps being the most frequent, each performed in 33% of cases in this area (Graph 10).
In the cervical and malar regions, all cases were BCCs, with edge-to-edge reconstructions.
In the palpebral and labial regions, all cases were also diagnosed as BCCs, with the advancement flap being the most commonly used reconstruction method.
Non-melanoma skin tumors in advanced stages have high morbidity. Prevention, early diagnosis and an effective treatment that leads to a decreased risk of recurrence – such as MMS – are crucial for the reduction of morbidity.
According to a recent publication on MMS in Brazil, the technique has been performed in the country for at least 30 years, and is restricted to less than 1% of dermatologists, being mainly concentrated in the Southeast Region. Training in this technique takes about one year and is offered by only six accredited services.7
The lack of data on the epidemiology of non-melanoma skin cancer in the Brazilian population also justifies the present study.
There was a greater involvement of women as compared to men, while most of the literature suggests men are more affected by skin cancer.8-10 Recent studies, however, have demonstrated this change in the disease's profile.11-13
The literature indicates that lower phototypes, advanced age and photodamage are risk factors for skin cancer such as BCC and SCC,8,9 a fact that was confirmed by the present study, in which 67% of the patients had Fitzpatrick phototypes I or II. The mean age was 60.8 years, and 82% of the patients bore important photodamage (moderate or severe).
Regarding the location, it is known that lesions are more aggressive in the centrofacial region,13 which is a common area of recurrence. Among the tumors analyzed in the present study, 72% were located in an area of risk (nose, eyelid and ear), confirming their indication for MMS. Previous history of skin cancer was present in 62% of patients and, according to the literature, patients who have had skin cancer are at increased risk of new cutaneous neoplasms.14,15 This data also includes patients who had recurrence of a tumor previously removed with the traditional surgical method, having later been referred for MMS, which constituted 10% of the cases. Rowe .. presented data regarding recurrences of BCCs that had been treated with traditional therapies and had cure rates of roughly 82% after surgical excision, and 60% with electrocoagulation and curettage. The use of cryotherapy resulted in an 87% cure rate in time series of less than five years. The application of MMS in recurrent BCCs increased these cure rates to 94.4%.14
Other indications for MMS are extensive dimensions and tumor location aiming at preserving healthy tissue that is free of the neoplasia, which would not be possible with the conventional excision. In the present study, the tumor's large size and its location led to indication for MMS in 23% and 67% of the cases, respectively.
In the present study, BCCs and SCCs represented 90% and 8% of the tumors, respectively. The literature describes BCC as the most common type of skin cancer.8,9 In addition, BCCs that are extensive or recurred, or are located in areas with increased risk, is the main indication for MMS, justifying its high prevalence in the studied sample.
There was also one case of trichoepithelioma that was initially diagnosed as BCC, being correctly diagnosed during intraoperative biopsy. Trichoepithelioma is a benign skin tumor that differentiates from the hair follicle and arises as a usually solitary, erythematous, usually facial tumor that resembles BCC both clinically and histologically, constituting an important differential diagnosis.
In the present study, the authors observed an average number of three operative phases per surgery, demonstrating the prevalence of aggressive tumors, given that the actual invasion was more extensive than that detected clinically.
The studied patients did not experience recurrence of the operated tumors, with the majority being followed up for more than one year (6 to 18 months). Although the follow-up duration can still be deemed as short, these data show the effectiveness of the MMS technique.
The study has some limitations (i.e. small number of patients and short follow-up time), which are justified by the fact that the sampling method was based on convenience, using a technique that still not largely performed in Brazil, at a dermatologic surgery referral service that has only been using the MMS technique for two years.
The data analyzed allow indicating MMS as an excellent therapeutic option in cases of tumors that are aggressive, have large dimensions, and are located in areas of high risk or recurrence. When performed by professionals with adequate training, this technique is safe and reliable, with a tendency to become increasingly frequent in the practice of the dermatologist physician. The present study is in line with most of the current literature regarding the epidemiological data of non-melanoma skin cancer.
1. Trost LB, Bailin PL. History of Mohs surgery. Dermatol Clin. 2011;29(2):135-9.
2. Mohs FE. Chemosurgery for skin cancer: fixed tissue and fresh tissue techniques. Arch Dermatol. 1976;112(2):211-5.
3. Reis NA, Azevedo LCM, Stolf HO, Nouri K, Kimyai-Asadi A, Goldberg LH. Cirurgia micrográfica de Mohs. Surg Cosmet Dermatol (Impr). 2011;3(3):227-31.
4. Mohs FE. Origin and progress of Mohs micrographic surgery. In: Snow SN, Mikhail GR, editors. Mohs micrographic surgery. 2nd edition. Madison: University of Wisconsin Press; 2004. p. 3-14.
5. Arnon O, Rapini RP, Mamelak AJ, Goldberg LH. Mohs micrographic surgery: current techniques. Isr Med Assoc J. 2010;12(7):431-5.
6. 6. Karampoiki V, Flores FJ, Altinoz H, Chojnacka M, Karentzou I, Dambrosio M, et al. Screening Evaluation System--Europe (SESy_Europe) met skin cancer screening. Cent Eur J Public Health. 2007;15(2):71-3.
7. Pessanha AC, Cernea SS. Perfil da Cirurgia Micrográfica de Mohs no Brasil. Jornal da Sociedade Brasileira de Dermatologia. Available from: http://www.sbd.org.br/publicacao/n%cb%9a-1-janeiro-fevereiro-de-2016/. Accessed in 2016 (Jul 11).
8. Mahmoud SF, Azadeh B. Basal cell carcinoma in Qatar. Int J Dermatol. 1996;35(1):704-6.
9. Chuang TY, Popescu A, Su WP, Chute CG. Basal cell carcinoma. A population- based incidence study in Rochester, Minnesota. J Am Acad Dermatol. 1990;22(3):413-7.
10. Leffell DJ, Fitzgerald DA. Basal cell carcinoma. In: Freedberg IM, Eisen AZ, Wolff K, Austin KF, Goldsmith LA, Katz SL, et al., editors. Fitzpatrick's dermatology in general medicine. 5th ed. New York: McGraw-Hill; 1999. p. 857-64.
11. Nigro MHMF, Brandão LSG, Coelho APCP, Motta LM, Bastazini Júnior I. Estudo epidemiológico do carcinoma ba¬socelular no período de 2010 a 2013 em um hospital de referência em dermatologia na cidade de Bauru. Surg Cosmet Dermatol. 2015;7(3):232-5
12. Mantese SAO, Berbert ALCV, Gomides MDA, Rocha A. Carcinoma basocelular - Análise de 300 casos observados em Uberlândia – MG. An Bras Dermatol. 2006;81(2):136-42.
13. Ruiz Lascano A, Kuznitzky R, Garay I, Ducasse C, Albertini R. Factores de riesgo para carcinoma basocelular. Estudio de casos-controles em Cordoba. Medicina (B. Aires). 2005;65(6):495-500.
14. Rowe DE, Carroll RJ, Day CL Jr. Prognostic factors for local recurrence, metastasis, and survival rates in squamous cell carcinoma of the skin, ear, and lip. Implications for treatment modality selection. J Am Acad Dermatol. 1992;26(6):976-90.
15. Marcil I, Stern RS. Risk of developing a subsequent nonmelanoma skin cancer in patients with a history of nonmelanoma skin cancer: a critical review of the literature and meta-analysis. Arch Dermatol. 2000 Dec;136(12):1524-30.
The present study was performed at the Universidade de Mogi das Cruzes - Mogi das Cruzes (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}