


Doris Hexsel1; Patrícia Caspary2; Fernanda Oliveira Camozzato2; Aline Flor Silva3; Carolina Siega3
Introduction: Low level laser therapy has been considered a non-invasive treatment alternative to body remodeling and fat tissue reduction.
Objective: To evaluate the efficacy of low level laser therapy in reducing body circumference measures and subcutaneous adipose tissue of the abdomen and hips areas.
Methods: An open, prospective, monocentric study was performed including 25 women with localized fat on the hips and abdomen. Nine sessions of low level laser therapy were performed over 3 weeks. The participants were assessed at baseline and at 1, 4 and 12 weeks after treatment. Assessment of weight and body circumferences, lipid profile tests and MRI were performed.
Results: The abdominal circumference measurements showed a significant reduction up to 12 weeks after the treatment. Participants showed a more marked reduction in the hips region one week after the last session. Also one week after the completion of the treatment, 80% of the participants considered that the treatment improved their body contour. There was absence of reports of adverse events related to the treatment.
Conclusion: Low level laser therapy is safe and effective in reducing the circumference measurements, particularly in the abdominal region.
Keywords: LOW-LEVEL LIGHT THERAPY; SUBCUTANEOUS FAT; MAGNETIC RESONANCE IMAGING; LASER THERAPY; ABDOMINAL SUBCUTANEOUS FAT
The search for non-invasive cosmetic treatments for body remodeling has increased in recent years, due to the fact that these treatments are associated with low frequency of adverse events and complications. Many lasers have been used to treat localized fat and, more recently, low level laser therapy (LLLT) has been reported as an alternative to reduce the body's measures, by reducing the hip's, thigh's and waist's circumferences.
The mechanism of action of LLLT was the object of some studies, however it is deemed as controversial.1 The main hypothesis is linked to the formation of pores in the plasma membrane of adipocytes previously irradiated with LLLT, as demonstrated by Neira et al. 2 in an in vitro study. Electron microscopy images showed particles of fat coming out of adipocytes, while cells in the interstitial space remained untouched.2 Corroborating this hypothesis of Neira, the in vitro results obtained by Caruso-Davis et al. 3 showed that there is not lysis of adipocytes and that there is extravasation of whole triglycerides from the adipocytes' interior. Jankowski et al. 4 have questioned these hypotheses recently, suggesting an effect on lipid metabolism, possibly involving some autocrine systemic action.
Results obtained from different studies have reported LLLT's effectiveness in the reduction of body measures,3.5-8 which supports the use of this technology as a non-invasive alternative to body remodeling and reduction of subcutaneous tissue. However, up until now few studies used objective methods for determining the subcutaneous tissue's thickness before and after treatment with LLLT.4,9,10 In addition to the effects in the body's circumference, authors suggest that LLLT is able to improve the lipid profile, reducing the levels of serum cholesterol.11,12
The objective of the present study was to evaluate the effectiveness of a 635nm LLLT device (Zerona®, Erchonia Medical Inc., Melbourne, USA) in the reduction of the body's measures and subcutaneous adipose tissue in the abdomen and hips of women. Moreover, the studied individual's lipid profile was also evaluated before and after treatment with LLLT.
An open, prospective, single-center study was carried out at the Centro Brasileiro de Estudos em Dermatologia (Brazilian Center for Research in Dermatology), Porto Alegre (RS), Brazil, having been previously approved by the Research Ethics Committee of the Associação Hospitalar Moinhos de Vento. The main inclusion criteria were: female gender, aged between 18 and 60 years, body mass index (BMI) between 18.5 and 29.9kg /m2, fat accumulation located in the hip region and abdomen, and availability to maintain stable weight throughout the study period with a maximum acceptable variation of ± 5% of the total body weight. The main exclusion criteria were: pregnancy, lactation or intention to become pregnant during the study period; to have undergone other treatments to reduce body measures in the 30 days preceding the study and during the study; tanned skin or intention to expose the studied body site to the sunlight, to undergo artificial tanning or use tanning creams and / or self-tanning products during the study; to begin intensive practice of sport during the study or to go through a major change regarding the practice of sports during the study, or in the three months prior to the start of the participation in the study.
The treatment was performed in the hip and abdomen region of all patients included in the study with the device Zerona® (Erchonia Medical Inc., Melbourne, USA). This device has been approved for cosmetic use in 2010 by the Food and Drug Administration (FDA) and in 2013 by the Agência Nacional de Vigilância Sanitária – ANVISA (the Brazilian National Health Surveillance Agency). It is composed of two fixed (central) heads and four movable (lateral) heads, each containing a source diode laser (Figure 1). The emitted wavelength is 635nm, with a potency of 17,5mW per head. The adopted protocol was three sessions per week for three weeks, totaling nine sessions. The protocol allowed the possibility of missing only one session. In each session, the patients received the laser application in the supine position for 20 minutes and in the prone position for 20 minutes. The fixed diode sources were positioned on the line of the umbilicus, while the mobile sources were positioned on the body's side: two in the flanks' region and two in the hip's region, with all being positioned parallel to the patients' body's surface.
Each participant attended four evaluation visits: a selection visit (baseline), and at 1, 4, and 12 weeks after treatment (W1, W4 and W12). In the selection visit, after obtaining the participant's consent, the researchers carried out a physical examination, including measurement of weight, clinical evaluation and checking of inclusion and exclusion criteria. The patients were then scheduled to undergo examination of lipid profile and MRI. Clinical evaluations with body circumference measurements were performed in all visits. Lipid profile tests were performed at baseline and at S1.
The MRI was performed at baseline and 12 weeks after treatment (W12).
Abdomen and hip circumferences measurement
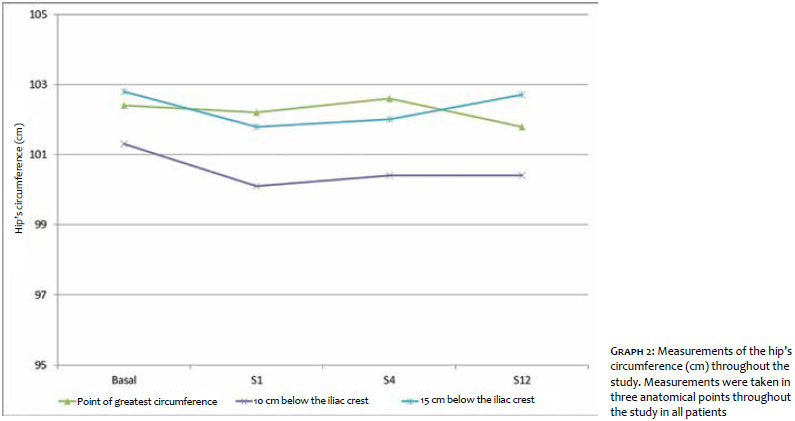
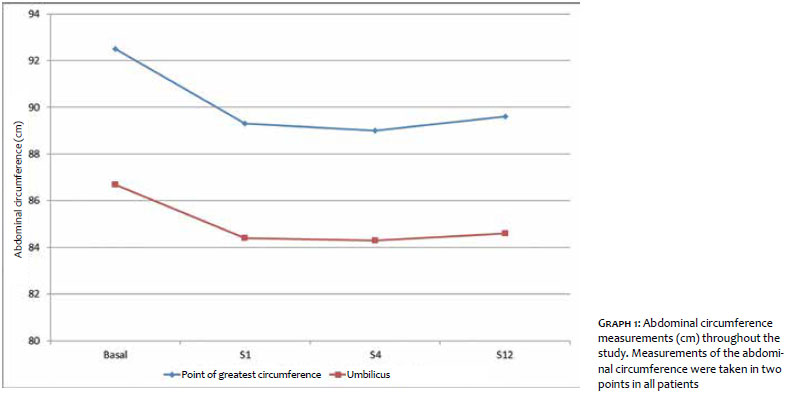
Three circumference measurements were performed in the hip: one at the point of greatest circumference and the other two 10 and 15cm below the iliac crest. Two circumference measurements were performed in the abdomen: one at the point of greatest circumference and the other at the umbilicus' height. In order to standardize the measures at the points of greatest circumference, it was decided that the point's height to the ground should be measured and recorded in the medical records at baseline, and used as a parameter in the subsequent visits.
Adipose tissue's thickness
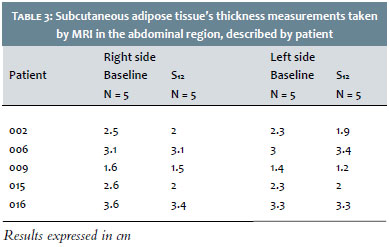
Ten of the 25 patients were invited to sequentially undergo the MRI, with five undergoing the scan in the abdominal region and the other five, in the hip region. The device 1.5 Tesla closed bore scanner (Magnetom Essenza, Siemens, Erlangen, Germany) was used to obtain the MRI images in T1. The measurement of the subcutaneous adipose tissue's thickness was performed on the images with the assistance of pre-defined anatomical markers. In the hip region, the anatomical point defined for the reproduction of images was the femur's head at its greatest circumference. In the abdomen, the chosen point was the umbilicus.
The thickness of the subcutaneous adipose tissue was measured on the right and left sides, in millimeters (mm), using the Syngo software (Siemens, Erlangen, Germany). An independent radiologist physician performed the evaluations before and after the treatment.
Statistical analysis
Demographic descriptive data for the population with intention to treat were analyzed.
The results obtained with the evaluations regarded the population from a protocol standpoint. The categorical variables were expressed as percentages, while the quantitative variables were expressed in mean ± standard deviation. The differences between cholesterol and triglyceride levels pre and post-treatment were tested with the t-test for paired samples, while the differences in body weight and corporal circumference measurements were tested with ANOVA for repeated measurements.
Having signed the Consent Term, 32 patients were evaluated, and 25 were included. Twenty patients completed the study, with 4 having dropped out due to lack of availability to attend all visits, and 1 participant was excluded for exceeding the limit of the allowed body weight variation (± 5%).
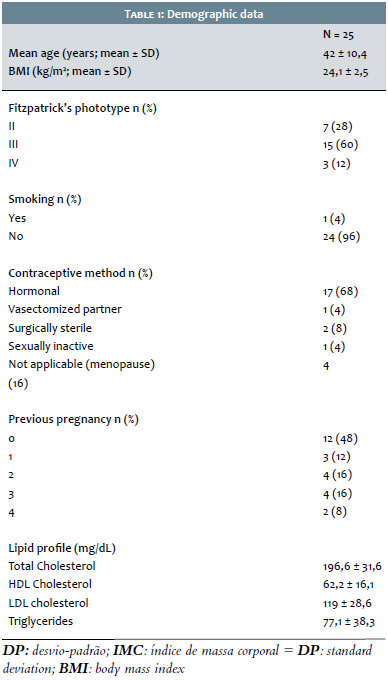
Demographic data of the included patients are described in Table 1. The patients' average age was 42 ± 10.4 years [variation: 22-59] while their BMI was 24.1 ± 2.5kg /m2. Most of the patients had Fitzpatrick skin phototype III (60%) and reported the use of hormonal contraception (68%). On average, the weight of the patients who completed the study remained stable over the assessment timepoints, with a maximum variation of 0.4kg between the baseline and the last evaluation (p> 0.05).
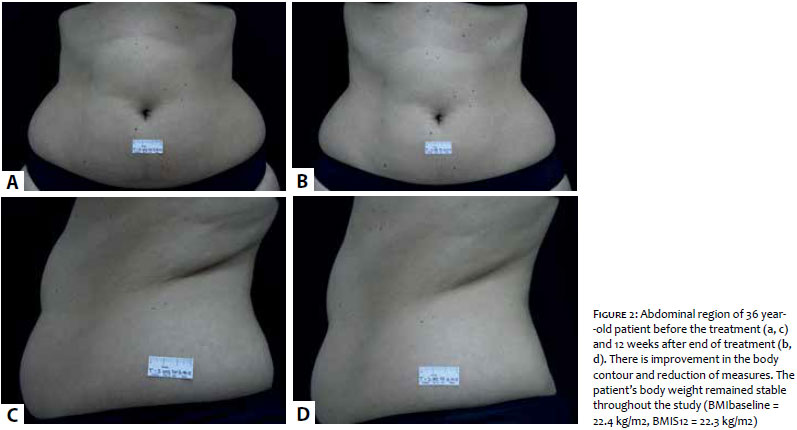
The abdominal circumference measurements at the greatest circumference and the umbilicus' height were significantly reduced in up to 12 weeks after the treatment (p = 0.001 and p <0.001, respectively), as shown in Graph 1. In addition to the statistical improvement, clinical and aesthetics improvement with visually perceptible reduction of measures, was observed in W12 as compared to the baseline (Figures 2 and 3). Nevertheless, analyzing the hip's measures, it was possible to observe a reduction trend in the body circumference at the points located at 10cm and 15cm below the iliac crest, only between the baseline and S1 (Figure 2). This reduction was not maintained throughout the study period.
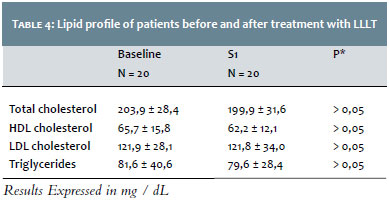
The 4 patients whom had their hip regions evaluated by MRI and have completed the study showed a decrease in the subcutaneous adipose tissue's thickness in the point measured on the right side. On the left side, 2 patients showed a decrease in the subcutaneous adipose tissue's thickness and other 2 presented the same measurements pre- and post-treatment (Table 2). In the abdomen region, 3 of the 5 patients evaluated had a decrease in the thickness of the subcutaneous adipose tissue in both sides (Table 3). There was absence of reports of adverse events linked to the treatment by the patients, whose lipid profile did not significantly change after the treatment (Table 4).
A week after the completion of the treatment, 80% of the patients felt that it improved their body contour, 75% noticed reductions in their measures and would undergo the treatment again, and 65% said they were satisfied. Twelve weeks after the end of the treatment, 55% of the patients noticed improvement in their body contour, 50% observed a reduction in the measures and were satisfied with the treatment, and 75% would undergo it again.
The present study evaluated the effects of a LLLT nine-session protocol for improving the body contour, reducing measures and the fat thickness in the abdominal and hip regions. The patients showed a significant decrease in abdominal measures after the treatment, with permanence of the outcome for up to 12 weeks after the last session. In the hip region, however, it was not possible to observe the same pattern in the reduction of measures: the patients had a more marked reduction one week after the last session, maintaining it throughout the study period.
Reductions in the body's circumference measurements have already been described by other researchers.3,5-8,13 Most authors have reported the use of the treatment in question in the abdominal region3,5,6,8 with significant effects in up to 2 weeks after its completion. In the present study, the outcomes were maintained for a considerably longer period in the abdominal region than previously described, while results in the hip region was similar to those found in the literature. Previous publications3,5,6,8,13 describe the use of protocols with fewer treatment sessions.
McRae and Boris assessed the correlation of weight variation with decreases in body circumference measurements. Although the reduction in weight was significant, the authors describe a weak correlation between changes in weight and body circumference measurements.13 In the present study, the weight variation observed in the evaluated patients was not statistically significant.
The decrease in the thickness of subcutaneous adipose tissue measured by MRI was observed in most of the evaluated anatomical points in both the abdominal and hip regions. Due to the small number of patients assessed, these data were not statistically evaluated. Magnetic resonance imaging is a safe, effective and reproducible method for the evaluation and quantification of body fat.14-16 This technique creates a good contrast between the body's diverse soft tissues, providing accurate images for measuring the adipose tissue's thickness.
Jankowski et al.4 carried out a double-blind randomized study, which included the assessment of the subcutaneous adipose tissue's thickness after treatment with LLLT (6 sessions over 2 weeks). Nonetheless, these authors used ultrasonography as the assessment methodology. The found data suggest that the decrease in the tissue's thickness would be related to the patients' different physical activity habits, however the study is inconclusive since this factor was not controled.4 In addition, the presence of physical activity was not controlled in the present study, where the criterion established for patients was that changes in health habits should not occur.
In line with the data reported by other authors3,6,7,13, the occurrence of adverse events linked to the treatment was not verified in the present study. Like Savoia et al.10 observed, there were not significant changes in serum cholesterol and triglycerides in the present study. Savoia et al. suggest that the combination of LLLT with vibration therapy can have led to an increase in the basal metabolism and ensuing consumption of the lipids mobilized from the adipose tissue.10 In the present study, however, LLLT was not associated with any other procedure or therapy. The results obtained reinforce the hypothesis that mobilization of LLLT activated fat does not result in higher cholesterol levels. Likewise, the treatment did not result in the reduction of these levels, as suggested by different autores.11,12
In the present study, it was possible to observe that LLLT was effective in reducing the body's circumference measurements, particularly in the abdominal region. The treatment was proven safe according to the used protocol, without changes in the cholesterol and triglyceride levels, with absence of other adverse events linked to the treatment. Other studies with controlled parameters – including the daily practice of physical activity – are needed to confirm the effectiveness of LLLT in reducing body measures.
1. Avci P, Nyame TT, Gupta GK, Sadasivam M, Hamblin MR. Low-level laser therapy for fat layer reduction: a comprehensive review. Lasers Surg Med.2013;45(6):349-57.
2. Neira R, Arroyave J, Ramirez H, Ortiz CL, Solarte E, Sequeda F, et al. Fat liquefaction: effect of low-level laser energy on adipose tissue. Plast Reconstr Surg. 2002;110(3):912-22.
3. Caruso-Davis MK, Guillot TS, Podichetty VK, Mashtalir N, Dhurandhar NV, Dubuisson O, et al. Efficacy of Low-Level Laser Therapy for body contouring and spot fat reduction. Obes Surg. 2011;21(6):722-9.
4. Jankowski M, Gawrych M, Adamska U, Ciescinski J, Serafin Z, Czajkowski R. Low-level laser therapy (LLLT) does not reduce subcutaneous adipose tissue by local adipocyte injury but rather by modulation of systemic lipid metabolism. Lasers Med Sci. 2016 Jul 6. In Press. doi:10.1007/s10103-016-2021-9.
5. Jackson RF, Stern FA, Neira R, Ortiz-Neira CL, Maloney J. Application of low-level laser therapy for noninvasive body contouring. Lasers Surg Med. 2012;44(3):211-7.
6. Jackson RF, Dedo DD, Roche GC, Turok DI, Maloney RJ. Low-level laser therapy as a non-invasive approach for body contouring: a randomized, controlled study. Lasers Surg Med. 2009;41(10):799-809.
7. Nestor MS, Zarraga MB, Park H. Effect of 635nm low-level laser therapy on upper arm circumference reduction A double-blind, randomized, sham-controlled trial. J Clin Aesthet Dermatol. 2012;5(2):42-8.
8. Thornfeldt CR, Thaxton PM, Hornfeldt CS. A six-week low-level laser therapy protocol is effective for reducing waist, hip, thigh, and upper abdomen circumference. J Clin Aesthet Dermatol. 2016;9(6):31-5.
9. Elm CM, Wallander ID, Endrizzi B, Zelickson BD. Efficacy of a multiple diode laser system for body contouring. Lasers Surg Med. 2011;43(2):114-21.
10. Savoia A, Landi S, Vannini F, Baldi A. Low-level laser therapy and vibration therapy for the treatment of localized adiposity and fibrous cellulite. Dermatol Ther (Heidelb). 2013;3(1):41-52.
11. Jackson RF, Roche GC, Wisler K. Reduction in cholesterol and triglyceride serum levels following low-level laser irradiation: a noncontrolled, nonrandomized pilot study. Am J Cosmet Surg. 2010;27(4):177-84.
12. Aquino AE Jr, Sene-Fiorese M, Paolillo FR, Duarte FO, Oishi JC, Pena AA Jr, et al. Low-level laser therapy (LLLT) combined with swimming training improved the lipid profile in rats fed with high-fat diet. Lasers Med Sci. 2013;28(5):1271-80.
13. McRae E, Boris J. Independent Evaluation of Low-Level Laser Therapy at 635 nm for Non-Invasive Body Contouring of the Waist, Hips, and Thighs. Lasers Surg Med. 2013;45(1):1-7.
14. Zhou A, Murillo H, PengNovel Q. Segmentation Method for Abdominal Fat Quantification by MRI. J Magn Reson Imaging. 2011;34(4):852-60.
15. Querleux B. Cellulite characterisation by high-frequency ultrasound and high-resolution magnetic resonance imaging. In: Goldman MP, Bacci PA, Leibaschoff G, Hexsel D, editors. Cellulite Pathophysiology and Treatment. New York: Informa Taylor & Francis; 2006. p.105-14.
16. Hexsel D, Siega C, Schilling-Souza J, Porto MD, Rodrigues TC. A Comparative Study of the Anatomy of Adipose Tissue in Areas with and without Raised Lesions of Cellulite Using Magnetic Resonance Imaging. Dermatol Surg. 2013;39(12):1877-86.
The present study was conducted at the Centro Brasileiro de Estudos em Dermatologia. - Porto Alegre (RS), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}