


Célia Kalil1; Valéria Campos2; Clarissa Prieto Herman Reinehr2; Christine Rachelle Prescendo Chaves3
The topical route for the delivery of drugs is essential in dermatology: it optimizes the penetration of medicaments, and when performed with the assistance of lasers, it takes place in a uniform and controlled manner. The degree of evidence of drug delivery is being investigated for many drugs. Moreover, the technique combines outstandingly with lasers for rejuvenation and treatment of skin diseases. It is therefore possible to conclude that the use of lasers for drug delivery is promising. While there are clinical studies on some substances that allow their indication and use, others require further controlled analyses, with longer follow-up periods, aimed at allowing thorough evaluations.
Keywords: LASERS; ADMINISTRATION, CUTANEOUS; SKIN ABSORPTION; DRUG DELIVERY SYSTEMS; DRUG ADMINISTRATION ROUTES
Topical delivery of drugs is essential in dermatology. Moreover, it is of paramount importance that the drug applied on the skin be capable of penetrating cutaneous layers and reaching the target structure. It has many advantages over the oral, intramuscular and intravenous systemic routes, for there is absence of first-pass metabolism, and it reduces side effects present in the systemic use, increasing patient adherence to the treatment.1 The epidermal barrier function is preserved by the stratum corneum's lipid bilayer, which is the main limiting factor for the use of drugs applied on the skin.2 The penetration of drugs across an intact stratum corneum takes place by diffusion and, to a lesser extent, through the skin's appendages, and can occur by transcellular or intracellular pathway.1 Only lipophilic and smaller than 500Da molecules are capable of penetrating an intact stratum corneum.1 Furthermore, only 1% to 5% of the product applied to the skin is absorbed and becomes bioavailable to exert its therapeutic effect.
The technique termed drug delivery consists in finding methods to optimize the penetration of drugs into the skin, and this can be achieved using chemical, mechanical and physical methods.1 The use of lasers as drug delivery agents was described in 1987 with the use of an ablative non-fractional device.3 In 2004, Anderson introduced the concept of fractional photothermolysis, in which healthy skin areas are maintained among thermally damaged areas (micro thermal zones - MTZ) generated by the ablative fractional laser, transforming the use of ablative lasers.4 The use of lasers allows the delivery of drugs in a uniform and controlled way.5
Lasers stimulate drug delivery by the means of three processes: 1- tissue ablation, which removes the stratum corneum and the most superficial layers of the epidermis; 2 - photomechanical waves, resulting from the conversion of light into mechanical energy; and 3 - non-ablative resurfacing, where thermal and physical injuries ruptures the skin barrier, promoting the delivery of medications.6 The degree of evidence of the drug delivery technique has been investigated for many drugs, resulting in different degrees of recommendation, according to the substance studied. While some drugs have already been trialed in randomized clinical tests comparing the technique with traditional methods, some still need further assessment aimed at elucidating the degree of evidence and clinical indication.
Regarding the product used for drug delivery, there are some recommendations to be observed, according to the method employed. Ablative and Q-switched lasers should be preferred when hydrophilic vehicles are used. In contrast, non-ablative lasers and intense pulsed light (IPL) should be chosen for lipophilic active principles.7 The more fluid is the used vehicle, the better the penetration of the active principles. The presence of cosolvents in the formulation significantly increases the penetration of the active principle with laser based drug delivery.7 Anhydrous formulations hinder the proliferation of microorganisms and do not cause burning sensation, sensitivity or comedones during the application.7
Although controversial, the use of sterile products is questionable, for contamination with microorganisms located on the skin's surface can occur even after proper asepsis of the treated area and with the use of sterile formulations. In addition, most studies have used non-sterile products for drug delivery, with absence of descriptions of severe complications or side effects.
The present article is aimed at reviewing the current knowledge about the drug delivery technique assisted by lasers.
The bibliographic research was performed on the MEDLINE, Cochrane and Lilacs-Scielo data bases using the following keywords: (fractional laser OR ablative fractional laser) AND (drug delivery OR transdermal delivery OR topical administration), (laser AND (drug delivery OR transdermal delivery OR topical administration) and (non ablative fractional laser) AND (drug delivery OR transdermal delivery OR topical administration) and (non ablative fractional laser) AND (drug delivery OR transdermal delivery OR topical administration).
After the selection of papers, the pieces were read based on their Titles and Abstracts, with those pertinent to the study being included. The in vivo studies were classified as randomized or non-randomized clinical trials.
The main ablative fractional lasers are 2,940nm Er:YAG and 10,600nm CO2 laser, which operate in the infrared band and have water as chromophore.6 The 2,940nm Er:YAG laser has a higher affinity for water, being therefore absorbed by the epidermis' water, allowing a more superficial penetration and minimum generations of heat. On the other hand, the 10,600nm CO2 laser penetrates deeper and generates higher amounts of heat. Both lasers facilitate drug delivery both through MTZs and through thermal effect present on the tissue surrounding the MTZs.8,9 Ablative fractional lasers characteristically act through tissular ablation columns surrounded by coagulation tissue (the MTZs), which can be modulated according to the used laser's type and energy. These channels penetrate the stratum corneum and grant direct access to lower layers, facilitating the drug delivery of medications applied on the skin. The MTZs can be adjusted using two parameters: density (i.e. the number of micropores per given area) and depth (which is controlled by choosing the level of fluence).6 The adjustment of the wave type and pulse duration used in ablative fractional laser allow to modulate the ablation degree and the thickness of the coagulation column adjacent to the MTZ: if too thick, this coagulation column hampers the diffusion of the applied substance for drug delivery into the areas adjacent to the MTZ.10 In addition, the use of excessively high energies results in deeper lesions, which can reach the vessels, thus entailing that the active principle in question may enter the bloodstream, an unwanted effect for drugs that act on the skin. When comparing the ablative fractional CO2 laser with the 2,940nm Er:YAG, it is observed that the coagulation column is smaller in the latter due to its higher affinity for water, which favors the emergence of bleeding points in the MTZ, decreasing the permeation of active principles applied in the area. This phenomenon can be minimized using lower energy levels, specific for drug delivery, as already made available in some laser devices.10
In vitro studies assessed the influence of the number and depths of pores for ablative fractional laser based drug delivery, observing that the delivery of the drug was dependent on the number of pores in the analyzed area.11 Nevertheless, once a certain MTZ density is reached, subsequent increases in density do not promote increased permeation of the drug due to the excessive thermal damage inflicted to the tissue adjacent to the MTZ.10 In general, substances containing hydrophilic molecules depend on the MTZ's depth to be absorbed – a phenomenon that does not occur with lipophilic molecules. 6
Drug delivery of aminolevulinic acid (ala) and methyl-aminolevulinic acid (mal) assisted by ablative fractional laser
Drug delivery of ALA and MAL assisted by ablative fractional laser is one of the more intensely studied, with a great number of pre-clinical and clinical analyses comparing it with the traditional technique and with the use of other drug delivery methods. Its use has been described in actinic keratoses, Bowen's disease, basal cell carcinoma, actinic cheilitis and onychomycosis.8,10,12-19
The delivery of MAL after pre-treatment with ablative fractional CO2 laser in pig skin was studied by Haederstal et al. in 2010.10 The study's outcomes showed that pretreatment with lasers allowed a deep and uniform distribution of the drug due to radial diffusion of the product deposited on the MTZs. In 2014, the same authors evaluated the action of 10,600nm CO2 laser followed by the application of ALA and MAL, describing an increase in the protoporphyrin IX's fluorescence of up to a depth of 1,8mm in the skin pretreated with laser. In addition, centrifuge radial diffusion of MAL was observed based on the uniform fluorescence of up to 1.5mm beyond the micropores inflicted by the laser.12
In 2013, Ko et al. evaluated the use of 2,940nm Er:YAG ablative fractional laser followed by the application of MAL in the treatment of 236 facial actinic keratoses of in 45 patients who were randomized to receive either only photodynamic therapy (PDT) or PDT after pre-treatment with laser. Photodynamic therapy assisted by laser was more effective for treating the lesions, especially hyperkeratotic ones (p = 0.001).13
In 2015, the use of 2,940nm Er:YAG ablative fractional laser followed by MAL application was evaluated for the treatment of actinic cheilitis in a randomized clinical trial. The study selected 33 patients with actinic cheilitis (confirmed by histology) who were randomized to receive either one pretreatment session of 2,940nm Er:YAG ablative fractional laser immediately followed by PDT or two sessions of traditional PDT with a seven-day interval between them. The group pretreated with laser had a more effective response both in the first 3 months of follow up (92% versus 59% of complete cure, p = 0.04) and after 12 months of follow up (85% versus 29%). In addition, the method including the pretreatment led to a lower recurrence rate in the 12 months after the procedure (p = 0.029).14 Adverse effects ranged from mild to moderate, with absence of systemic effects reports. Using the same comparison techniques, the authors treated 440 facial and scalp actinic keratoses in 93 patients, in a follow on study.16 In that study, the MAL's incubation time was modulated, which lasted 2 to 3 hours. The outcomes showed the superiority of the 3-hour incubation technique associated with the laser as compared to the others. Moreover, this superiority was maintained in the 12-month follow up with statistical significance.16
A 2016 in vivo study evaluated 5 patients regarding the absorption of ALA.8 The drug was applied to each patient's arm in four areas: the first received an isolated topical application of the drug; the second received an application after pretreatment with fractional CO2 laser; in the third area, the application was combined with high pressure; and the fourth area received the application of high pressure transdermal acoustic waves. The ALA was occluded for 30 minutes for incubation in the 4 areas. After this period, biopsies were performed in all areas. The best outcomes regarding the penetration depth and lateral diffusion of ALA were derived from the combination of the two techniques (fractional CO2 laser combined with high pressure transdermal acoustic waves).
Drug delivery of diclofenac assisted by ablative fractional laser
In 2011, Bachhav et al. evaluated the use of 2,940nm Er:YAG laser applied on pig skin followed by the application of diclofenac in gel and in aqueous solution.20 Both the aqueous and the gel forms of diclofenac had their delivery enhanced by 13 times with the use of laser. Furthermore, the laser's fluence influenced permeation, but not the deposition diclofenac in the skin.
Drug delivery of lidocaine assisted by ablative fractional laser
In 2010, Bachhav et al. evaluated the application of 2,940nm Er:YAG laser on pig and human skins for the delivery of lidocaine. The delivery of the drug was dependent on the number of pores, but was not influenced by the depth of these pores.11
Drug delivery of corticoids assisted by ablative fractional laser
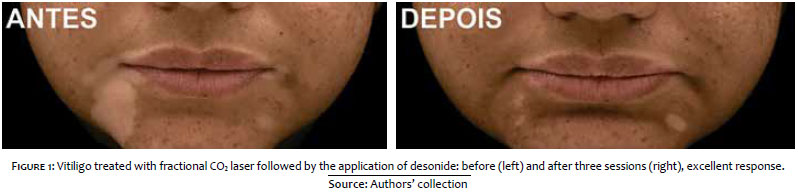
In 2015, Li et al. deemed as symmetrical and stable the effect of CO2 laser as a promoter of drug delivery for topical corticosteroids aimed at treating vitiligo in the body's extremities. Twenty-five patients underwent a split-body treatment. In on side of the body, the lesions received the laser application followed by betamethasone solution and narrowband UVB phototherapy. The other side received laser followed by phototherapy (control). The side treated with betamethasone solution immediately after the laser procedure had higher re-pigmentation as compared to the control side, with proportions of 40% (versus 8%) for patients with re-pigmentation greater than 50% (p < 0.05).21 Adverse effects were mild, and included edema, erythema and burning sensation, being were well tolerated. None of the patients experienced worsening of the vitiligo, Koebner phenomenon or local infection.
The drug delivery of 0.05% clobetasol propionate cream immediately after the application of ablative fractional CO2 laser associated with narrowband UVB phototherapy was also evaluated for the treatment of vitiligo in 26 patients.22 The average improvement scores were significantly higher than when there was association of the phototherapy with drug delivery of clobetasol. No significant adverse effects, such as the Koebner phenomenon, cutaneous atrophy, telangiectasias or hypertrophic scars, were reported.
Figure 1 shows the outcomes obtained by the authors in the treatment of a patient with vitiligo. Three ablative fractional CO2 laser sessions were carried out, followed by drug delivery of desonide.
In 2013, Waibel et al. treated 15 patients with hypertrophic scars in a case series.23 Three to 5 sessions of ablative fractional CO2 laser were performed in intervals of 2 to 3 months between the procedures. Drug delivery containing 10-20mg/ml triamcinolone acetonide was applied immediately after the laser. After six months assessing the overall improvement parameters, the improvement in the parameters scars, atrophy, dischromia and contour was 2.73, according to the Manchester modified scoring system, where the maximum score is 3. The parameter texture showed the best results, while the dischromia parameter obtained the lowest improvement scores.
Cavalié et al. assessed the drug delivery of betamethasone following the application of 2,940nm Er:YAG laser for treating 70 keloids, observing a mean improvement of 50% in the lesions, with a recurrence rate of 22% in 8 months.24
There is a case report of a dermatofibroma treated with fractional CO2 laser and drug delivery of 0.05% fluocinolone ointment with good outcome.25
Figure 2 illustrates the treatment of keloids with ablative fractional 2,940nm Er:YAG laser associated with drug delivery of triamcinolone with good results after only one treatment session.
Drug delivery of tranexamic acid assisted by ablative fractional laser
An in vitro study in pig skin evaluated the delivery of tranexamic acid after pretreatment with fractional or conventional CO2 laser. The fractional variant was as effective as the traditional in delivering the drug, however it inflicted less damage to the epidermis.26
Drug delivery of methotrexate assisted by ablative fractional laser
In 2008, Lee et al. carried out an in vitro evaluation of the methotrexate's permeation assisted by either 2,940nm Er:YAG laser or electroporation in rodents' healthy skin (nude mouse), observing that the use of laser led to increased absorption of the drug by 3 to 80 times, the according to used fluence.27 A later study – in vitro, in pig skin – demonstrated that 2,940nm Er:YAG laser treatment for delivering methotrexate depended upon the MTZ's depth: the absorption of the drug increased by 6, 9 and 11 times when the MTZ reached the epidermis, the superficial dermis and the medium dermis, respectively.28
Drug delivery of vitamin C assisted by ablative fractional laser
In vitro studies have evaluated the uses of 10,600nm CO2 and 2,940nm Er:YAG lasers in the pretreatment of the skin, with different formulations containing vitamin C. Increases of up to 277 times were evidenced in the skin's permeation as compared to the to untreated skin.29
Hsiao et al. evaluated the permeation of ascorbic acid after the application of ablative fractional or conventional CO2 laser, observing similar results irrespective of the laser used.29 In 2013, a similar study was conducted by Huang et al., with three different forms of stabilized vitamin C.30
In 2016, in a split-face study co-authored by one of the present article's authors, Waibel et al., evaluated the use of CO2 laser in the drug delivery of a non-sterile formulation containing vitamin 15% vitamin C, 1% vitamin E and 0.5% ferulic acid in serum vehicle, demonstrating acceleration in the healing of the hemiface that received the formula, despite the fact that this outcome was not statistically significantly different.5 The molecular analysis of biopsy specimens harvested five days after the treatment showed the presence of increased fibroblast growth factor – which stimulates tissue repair – in the hemiface that underwent the drug delivery method. There were no descriptions of irritative effects resulting from the applied formulation.
Figure 3 shows the results obtained by the authors of the present article in the rejuvenation treatment of a patient with one ablative fractional CO2 laser session followed by drug delivery with vitamin C.
Drug delivery of 5-fluorouracil (5-FU) assisted by ablative fractional laser
Nguyen et al. evaluated the use of ablative fractional CO2 laser associated with the drug delivery of 5% 5-fluorouracil (5-FU) under occlusion for the in situ treatment of in 30 lesions of superficial basal cell carcinoma and squamous cell carcinoma in the trunk and extremities. Five-fluorouracil was administered daily during the first seven days after the treatment, under occlusion. Biopsies of the treated area harvested from 4 to 8 weeks after the treatment confirmed histologic healing in 87% of the treated lesions. Adverse effects were mild and included erythema and erosion, with absence of local infections.31
The use of drug delivery in 5% 5-FU was also evaluated in the treatment of non-segmental vitiligo pretreated with ablative fractional 2,940nm Er:YAG laser, and post-treated (subsequently to the application of 5-FU) with narrow band UVB phototherapy, in a prospective right/left comparative study.32 The association of laser assisted drug delivery with phototherapy resulted in repigmentation in 78% of the patients (versus 23.4% in the group that received only phototherapy).
Drug delivery of imiquimod assisted by ablative fractional laser
Lee et al. performed an in vitro study with 2,940nm Er:YAG and drug delivery of imiquimod, where there was an increase in the skin's permeability of imiquimod after pretreatment with laser, dependent upon the fluence and of number of passes in the treated area.33
Drug delivery of ingenol mebutate assisted by ablative fractional laser
According to an in vitro study, pretreatment of the skin with 2,940nm Er:YAG laser increased dermal permeation of ingenol mebutate. This penetration was influenced by the density set on the laser device, but not by the MTZ's depth.34 Braun et al. evaluated this finding in a case report based on a split-face study of field cancerization treatment. After pretreatment with 2,940nm Er:YAG, 0.015% ingenol mebutate was applied and maintained for three consecutive days. Despite the fact that both sides of the face showed an expected inflammatory reaction to the product, it was more intense on the side pretreated with laser.35
Drug delivery of tretinoin assisted by ablative fractional laser
An in vitro study evaluating the drug delivery of tretinoin evidenced that there was increased permeation after the application of ablative fractional laser. In addition, it demonstrated that this permeation was dependent upon the laser's fluence and density.36
Drug delivery of topical antifungals assisted by ablative fractional laser
Studies described the treatment of onychomycosis with an association of ablative fractional lasers and topical antifungals, such as terbinafine and amorolfine cream. The MTZs allowed the conformation of channels on the nail that removed the ungual tissue containing fungi and promote the drug delivery of products applied on the nail plate.37-39
A study by Yang et al. evaluating the use of ablative fractional laser for drug delivery on the nail plate employed optical coherence tomography aimed at identifying the optimal parameters in order not to damage the tissues located beneath the nail plate. They concluded that the use of tomography is effective in performing this analysis and ensures the procedure's safety.40
Drug delivery of polylactic acid assisted by ablative fractional lasers
Rkein et al. assessed the topical application of poly-L-lactic acid after fractional CO2 laser for the treatment of atrophic scars in 10 patients.41 Three months after, 95% of the scars received a improvement score of 2.18, on a scale ranging from 0 to 3.
Drug delivery of botulinum toxin assisted by ablative fractional laser
In 2015, Mahmoud et al. described the use of fractional CO2 laser followed by the application of topical botulinum toxin (drug delivery) in the periorbital area in a split-face study in 10 patients. The 30-day follow up evidenced significant improvement on the side associated with botulinum toxin (p = 0.027).42 Similar results were reported by Zhu et al. in 2016, when the topical application of botulinum toxin (drug delivery) was compared to the application of saline solution, both after pretreatment with fractional CO2 laser, in randomly chosen facial areas.43 Twelve weeks after, the combined treatment received an improvement score of 2.70 in wrinkles, hydration and elasticity, on a scale ranging from 0 to 3 (p ≤ 0.05).
Drug delivery of platelet-rich plasma (PRP) and adipose tissue stem cells assisted by ablative fractional laser
In a 2016 split-face study, Zhou et al. compared the effect of the application of stem cells from adipose tissue following pretreatment with ablative fractional CO2 laser, to the isolated application of laser. The combined treatment increased the patient's satisfaction, improved the elasticity and hydration, and reduced the transepidermal water loss, rhytids and melanin index. These results were observed both in the group treated for rejuvenation and in the group treated for acne scars.44
An assessment of the use of PRP in drug delivery after ablative fractional laser was performed in 2012 by Shin et al. Platelet rich plasma combined with laser increased the elasticity and decreased the erythema index. Increased thickness of the dermal-epidermal junction, collagen content and number of fibroblasts were also observed.45
Drug delivery of minoxidil and diphencyprone assisted by ablative fractional laser
Ablative fractional Er:YAG laser was used to accelerate the topical permeation of minoxidil, diphencyprone and peptides in rat and pig skins. There was increased permeation of all active principles, including into hair follicles. Drug delivery was evidenced by micrography in the hair follicles and intercellular space.46
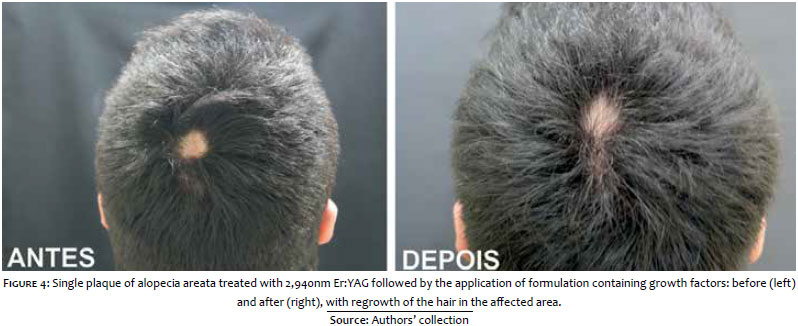
Drug delivery of growth factors assisted by ablative fractional laser
Figure 4 shows the outcome obtained by the authors of the present paper in the treatment of a patient bearing a single plaque of alopecia areata treated with 2,940nm Er:YAG lasr, followed by the application of a formula containing growth factors.
Other uses
Other uses of ablative lasers for drug delivery include the delivery of antibodies, vaccines, oligonucleotides and analgesics.
Ideal requirements for drug delivery formulations assisted by ablative fractional lasers.7
- Low viscosity vehicles are superior to emulsions, gels, or serums.
- The presence of cosolvents in the formulation promotes lateral diffusion (adjacent to MTZs) and increases deposition of the drug.
- Occlusion (which can be one of the vehicle's characteristics) increases the drug delivery effect.
- The permeation of hydrophilic active principles is facilitated by ablative fractional laser. The same is valid for active principles contained in nanocapsules, or those that are lipossomed or vectorized.
- Avoid the use of propylene glycol and alcohol in the formulations, for they reduce the active principles' penetration.
- Permeation of active principles occurs continuously up until the skin's barrier function is completely restored, even though it decreases over this process of recovery. For this reason, the patient can use the drug delivery formulation for 2 or 3 days after the procedure.
- Vehicles of anhydrous nature or mineral origin that do not contain preservatives and dyes, reduce the risk of allergic reactions and do not generate discomfort (burning sensation) during the immediate post-procedure application.
Non-ablative laser promotes drug delivery via thermal effect – as in the cases of 1,064nm long-pulse Nd:YAG laser, non-ablative fractional Erbium laser, and intense pulsed light (IPL) – or via photomechanical waves due to the high magnitude of the transient pressure – as in the case of Q (quality)-switched lasers.47 In 1998, Lee at al. demonstrated (in animal models) that even 40kDa macromolecules (dextran, for instance) could permeate into a cutaneous depth of 400µm, in vivo. Exposure of the skin to photomechanical waves leads to the expansion of the extracellular space up until the deeper layers of the stratum corneum, nevertheless the stratum granulosum remains unchanged. The addition of a cosolvent to the vehicle results in the large-scale expansion of the extracellular space, including intercellular ruptures in the stratum granulosum. The addition of a cosolvent to the vehicle used for drug delivery selectively acts on the lamellar lipids.48
Long-pulse lasers, non-ablative fractional Erbium laser and IPL increases the skin's temperature by up to 13ºC, with transient disruption of keratin, making corneocytes to become brittle and exfoliative. In contrast, 532nm and 1,064nm Q-switched lasers completely rupture the keratin and corneocytes with minimal increases of temperature, generating micropores in the stratum corneum.47 Q-switched lasers increase by 12 times the skin's permeability, which can remain at that level for up to one week, without risk of infection. In addition, it increases the permeation of hydrophilic molecules.47 On the other hand, the order of magnitude of the increase in the skin's permeability promoted by long-pulse Nd:YAG laser, non-ablative fractional Erbium laser and IPL is roughly 6.8 times, which lasts for 15 to 30 minutes.7
Different sources of light were studied in diverse doses as drug delivery promoters. The results demonstrated that all methods used to increase permeation of glycerol – lasers, such as CO2, 532nm and 1,064nm Nd:YAG; and 400-700nmn and 560-950nm IPL – significantly increased the transdermal delivery of the studied active principle as compared to the control group.49 The increase in transepidermal water loss (TEWL) after the treatment with non-ablative fractional laser demonstrates that the use of this type of device induced an increase in the skin's permeability. 50
Non-ablative fractional laser promotes dermal heating in a columns layout similar to the MTZs, however without causing significant damage to the overlying epidermis, being therefore associated with less discomfort and shorter recovery time than that of ablative fractional laser.51,52
Drug delivery of aminolevulinic acid (ALA) and methyl-aminolevulinic acid (MAL) assisted by non-ablative laser
Lim et al. evaluated 10 patients pretreated with non-ablative fractional 1,550nm Er:glass laser followed by PDT with ALA, left to incubate for 30, 60 or 180 minutes under occlusion. Each patient was treated in 12 areas in his or her dorsum. The study's results demonstrated increased penetration of ALA in the areas laser pretreated with laser. In addition, viewed under fluorescence, ALA absorption was proportional to the incubation's duration.51 In 2016, Lee et al. showed an increase of up to 1,200 times in the skin's permeability to ALA after pretreatment non-ablative fractional 1,550nm Er:Glass laser, as compared with the untouched skin.50
Drug delivery of topical antifungals assisted by non-ablative lasers
Kim et al. assessed the efficacy of 1,064nm Nd:YAG in the treatment of onychomycosis dividing the patients into 3 groups: Group 1 (treated only with laser); Group 2 (treated with laser and topical antifungal); Group 3 (treated only with antifungal). Laser was performed monthly, in a total of 3 or 4 sessions. Clinical and mycological outcomes demonstrated superiority of results in the laser treatment, isolated or combined with topical treatment, as compared to the treatment with topical antifungals. Furthermore, the addition of topical antifungal seemed to be capable of preventing reinfection in patients who received the combination treatment.53
Drug delivery of tretinoin assisted by non-ablative lasers
In 2016, Lee et al. evaluated in vitro the permeation of tretinoin into the skin pretreated with non-ablative fractional 1,550nm Er:glass laser. They observed a two-fold increase in the permeation of the active principle as compared with the untouched skin.50
Drug delivery of 5-fluorouracil (5-FU) assisted by Q-switched laser
The use of 1,064nm Q-switched Nd:YAG laser for drug delivery of 5-FU was effective in promote the permeation of the active principle in a study with animals.54
Drug delivery of vitamin C assisted by Q-switched laser
Zhou et al. evaluated the use of 694nm Q-switched ruby laser associated with sonophoresis and drug delivery of vitamin C lotion, for the treatment of melasma in 26 patients. They observed an initial reduction of 35% in the MASI Index (Melasma Area and Severity Index) after 3 months of follow up.55 In 2013, Lee at al. also evaluated the use 20% vitamin C with ultrasound after pretreatment with Q-switched laser. The results showed a significant improvement in the hemiface where the drug delivery was performed, according to the visual analog scale for the treatment of melasma.56
Drug delivery of cosmeceuticals assisted by Q-switched lasers (laser toning)
Kalil et al. reported improvement of acne, spots, pores, texture and UV index using a formula containing Hyaxel®, Hidroxiprolisilane®, DMAE Pidolato®, Nano Vit C® and Matrixyl 3000® as compared to a placebo group.57
Drug delivery of cosmeceuticals assisted by non-ablative laser
The authors of the present paper experienced excellent outcomes using non-ablative fractional 1,340nm Er:YAG laser associated with drug delivery containing growth factors (IGF – insulin growth factor, and EGF – epidermal growth factor) for the treatment of perioral scarring (Figure 5).
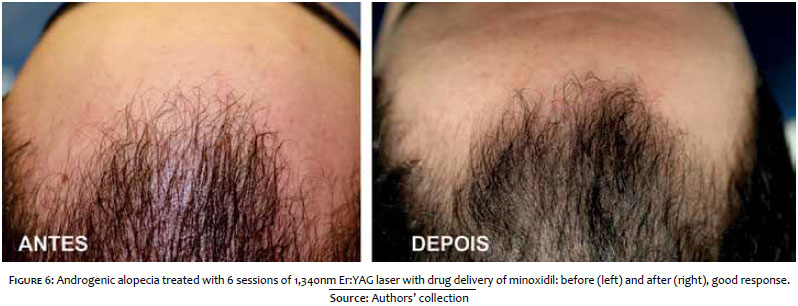
Drug delivery of minoxidil assisted by non-ablative laser
The authors of the present paper experienced excellent outcomes using non-ablative fractional 1,340nm Er:YAG laser associated with drug delivery of minoxidil for the treatment of androgenetic alopecia (Figure 6).
Ideal requirements for drug delivery formulations assisted by Q-switched lasers. 7, 48
- Vehicles with low viscosity and of hydrophilic nature are better than emulsions, gels, or serums.
- The presence of co-solvents in the formulation promotes the extracellular space dilation by increasing the diffusion of active principles throughout the skin. It also increases the skin barrier's restoration time.
- Hydrophilic active principles have their permeation facilitated by Q-switched lasers.
- The use of propylene glycol and alcohol in the formulations should be avoided for they reduce the active principle's penetration.
- The active principles' permeation is increased by at least 12 times, and this effect lasts for up to 1 week. In this manner, the drug delivery formulation can be used by the patient throughout this period.
Ideal requirements for drug delivery formulations assisted by non-ablative fractional lasers and IPL. 7, 49
- Low viscosity vehicles are better than emulsions, gels, or serums.
- The presence of co-solvents in the formulation promotes greater transient disruption of keratin and increases intercellular spaces.
- Lipophilic active principles have their permeation facilitated by long-pulse Nd:YAG laser, non-ablative fractional Erbium laser and IPL.
- The use of propylene glycol and alcohol in the formulations should be avoided for they reduce the active principle's penetration.
- The active principles' permeation is increased by at least 6.8 times, nevertheless this effect is ephemeral and lasts for roughly a 15 to 30 minutes, entailing that the drug delivery should be performed immediately after the procedure.
To date, there has been absence of descriptions of infections secondary to drug delivery procedure performed with lasers.
Soltani-Arabshahi et al. described two cases of foreign body reaction after microneedling and drug delivery with a commercial product for use at home containing vitamin C (Vita C Serum, Sanitas Skincare, PAÍS), confirmed by biopsy and with negative cultures for the biopsied sample.58 Another study described foreign body reactions after electroporation.59 Although the reports did not describe the use of lasers, attention should be given to the formula employed for drug delivery; some readymade formulas for daily use at home contain preservatives and dyes, which may be related to the observed adverse effects.
In a 2016 study, Lee et al. evaluated the risk of permeation of the bacteria Staphylococcus aureus and Pseudomonas aeruginosa after treatment of the skin with non-ablative fractional 1,550nm Er:glass laser observing absence of increase in the risk of bacterial infection after the laser application , as compared to the untouched skin.50
The use of lasers for promoting drug delivery is promising, however a greater number of controlled studies with longer follow-up periods are necessary in order to allow the evaluation some of the studied substances, which still do not have the adequate degree of evidence for indication. The standardization of the energy and density used in the laser applications, as well as the standardization of the concentration of each substance to be applied via drug delivery processes, call for a greater number of studies, since many articles discuss the use of lower concentrations of the active principles since there is increased permeability.6,9 The use of lower concentrations of active principles increases the safety of the procedure and reduces the risk of side effects.
Notwithstanding, issues linked to the procedure's safety, such as the potential risk of adverse effects secondary to the systemic absorption of the drugs and the risk of infection and immune sensitization, require a greater number of studies aimed at clarifying whether the use of sterile formulas for drug delivery is necessary, although a 2016 study by Lee et al. has demonstrated that the use of non-sterile formulas with non-ablative fractional laser is safe.50 Despite the fact that there are many topical formulations, it is necessary to determine which are appropriate or not for use in drug delivery.6 The cost of the procedure represents a constraint for its implementation in the daily practice, and it is necessary to discuss the cost/benefit of the procedure with the patient.9
The knowledge currently available demonstrated that the substances studied for the combined use of lasers are safe in the promotion of drug delivery, provided that the procedures are performed in medical environment, according to appropriate pre-procedure antisepsis protocols. The technique is promising and promotes a new application for lasers, allowing to expand its use not only in rejuvenation treatments, but also in the treatment of dermatological diseases, reducing the toxicity of the active principle and the costs of more expensive drugs, and increasing the therapeutic response.
1. Leite-Silva VR, de Almeida MM, Fradin A, Grice JE, Roberts MS. Delivery of drugs applied topically to the skin. Expert Rev Dermatol. 2012;7(4):383-97.
2. Purdon CH, Azzi CG, Zhang J, Smith EW, Maibach HI. Penetration enhancement of transdermal delivery--current permutations and limitations. Crit Rev Ther Drug Carrier Syst. 2004;21(2):97-132.
3. Jacques SL, McAuliffe DJ, Blank IH, Parrish JA. Controlled removal of human stratum corneum by pulsed laser. J Invest Dermatol. 1987;88(1):88-93.
4. Manstein D, Herron GS, Sink RK, Tanner H, Anderson RR. Fractional Photothermolysis: A New Concept for Cutaneous Remodeling Using Microscopic Patterns of Thermal Injury. Lasers Surg Med. 2004;34(5):426-38.
5. Waibel JS, Mi Q-S, Ozog D, Qu L, Zhou L, Rudnick A, et al. Laser-assisted delivery of vitamin C, vitamin E, and ferulic acid formula serum decreases fractional laser postoperative recovery by increased beta fibroblast growth factor expression. Lasers Surg Med. 2016;48(3):238-44.
6. Haedersdal M, Erlendsson AM, Paasch U, Anderson RR. Translational medicine in the field of ablative fractional laser (AFXL)-assisted drug delivery: A critical review from basics to current clinical status. J Am Acad Dermatol. 2016;74(5):981-1004.
7. Lin C-H, Aljuffali IA, Fang J-Y. Lasers as an approach for promoting drug delivery via skin. Expert Opin Drug Deliv. 2014;11(4):599-614.
8. Waibel JS, Rudnick A, Nousari C, Bhanusali DG. Fractional Ablative Laser Followed by Transdermal Acoustic Pressure Wave Device to Enhance the Drug Delivery of Aminolevulinic Acid: In Vivo Fluorescence Microscopy Study. J Drugs Dermatol. 2016;15(1):14-21.
9. Sklar LR, Burnett CT, Waibel JS, Moy RL, Ozog DM. Laser assisted drug delivery: a review of an evolving technology. Lasers Surg Med. 2014;46(4):249-62.
10. Haedersdal M, Sakamoto FH, Farinelli WA, Doukas AG, Tam J, Anderson RR. Fractional CO2 laser-assisted drug delivery. Lasers Surg Med. 2010;42(2):113-22.
11. Bachhav YG, Summer S, Heinrich A, Bragagna T, Böhler C, Kalia YN. Effect of controlled laser microporation on drug transport kinetics into and across the skin. J Controlled Release. 2010;146(1):31-6.
12. Haedersdal M, Sakamoto FH, Farinelli WA, Doukas AG, Tam J, Anderson RR. Pretreatment with ablative fractional laser changes kinetics and biodistribution of topical 5-aminolevulinic acid (ALA) and methyl aminolevulinate (MAL). Lasers Surg Med. 2014;46(6):462-9.
13. Ko D-Y, Jeon S-Y, Kim K-H, Song K-H. Fractional erbium: YAG laser-assisted photodynamic therapy for facial actinic keratoses: a randomized, comparative, prospective study. J Eur Acad Dermatol Venereol. 2014;28(11):1529-39.
14. Choi SH, Kim KH, Song K-H. Efficacy of ablative fractional laser-assisted photodynamic therapy for the treatment of actinic cheilitis: 12-month follow-up results of a prospective, randomized, comparative trial. Br J Dermatol. 2015;173(1):184-91.
15. Cai H, Wang Y, Zheng J-C, Sun P, Yang Z, Li Y, et al. Photodynamic therapy in combination with CO2 laser for the treatment of Bowen's disease. Lasers Med Sci. 2015;30(5):1505-10.
16. Choi SH, Kim KH, Song KH. Efficacy of ablative fractional laser-assisted photodynamic therapy with short-incubation time for the treatment of facial and scalp actinic keratosis: 12-month follow-up results of a randomized, prospective, comparative trial. J Eur Acad Dermatol Venereol. 2015;29(8):1598-605.
17. Oliveira GB de, Antonio JR, Antonio CR, Tomé FA. The association of fractional CO2 laser 10.600nm and photodynamic therapy in the treatment of onychomycosis. An Bras Dermatol. 2015;90(4):468-71.
18. Haak CS, Christiansen K, Erlendsson AM, Taudorf EH, Thaysen-Petersen D, Wulf HC, et al. Ablative fractional laser enhances MAL-induced PpIX accumulation: Impact of laser channel density, incubation time and drug concentration. J Photochem Photobiol B. 2016;159:42-8.
19. Fang J-Y, Lee W-R, Shen S-C, Fang Y-P, Hu C-H. Enhancement of topical 5-aminolaevulinic acid delivery by erbium:YAG laser and microdermabrasion: a comparison with iontophoresis and electroporation. Br J Dermatol. 2004;151(1):132-40.
20. Bachhav YG, Heinrich A, Kalia YN. Using laser microporation to improve transdermal delivery of diclofenac: Increasing bioavailability and the range of therapeutic applications. Eur J Pharm Biopharm. 2011;78(3):408-14.
21. Li L, Wu Y, Li L, Sun Y, Qiu L, Gao X-H. Triple combination treatment with fractional CO2 laser plus topical betamethasone solution and narrowband ultraviolet B for refractory vitiligo: a prospective, randomized half-body, comparative study. Dermatol Ther. 2015;28(3):131-4.
22. Vachiramon V, Chaiyabutr C, Rattanaumpawan P, Kanokrungsee S. Effects of a preceding fractional carbon dioxide laser on the outcome of combined local narrowband ultraviolet B and topical steroids in patients with vitiligo in difficult-to-treat areas. Lasers Surg Med. 2016;48(2):197-202.
23. Waibel JS, Wulkan AJ, Shumaker PR. Treatment of hypertrophic scars using laser and laser assisted corticosteroid delivery. Lasers Surg Med. 2013;45(3):135-40.
24. Cavalié M, Sillard L, Montaudié H, Bahadoran P, Lacour J-P, Passeron T. Treatment of keloids with laser-assisted topical steroid delivery: a retrospective study of 23 cases: A retrospective study of 23 cases. Dermatol Ther. 2015;28(2):74-8.
25. Wang AS, Larsen L, Chang S, Phan T, Jagdeo J. Treatment of a symptomatic dermatofibroma with fractionated carbon dioxide laser and topical corticosteroids. J Drugs Dermatol. 2013;12(12):1483-4.
26. Hsiao C-Y, Sung H-C, Hu S, Huang C-H. Fractional CO2 Laser Treatment to Enhance Skin Permeation of Tranexamic Acid with Minimal Skin Disruption. Dermatology. 2015;230(3):269-75.
27. Lee W-R, Shen S-C, Fang C-L, Zhuo R-Z, Fang J-Y. Topical delivery of methotrexate via skin pretreated with physical enhancement techniques: low-fluence erbium:YAG laser and electroporation. Lasers Surg Med. 2008;40(7):468-76.
28. Taudorf EH, Lerche CM, Erlendsson AM, Philipsen PA, Hansen SH, Janfelt C, et al. Fractional laser-assisted drug delivery: Laser channel depth influences biodistribution and skin deposition of methotrexate. Lasers Surg Med. 2016;48(5):519-29.
29. Hsiao C-Y, Huang C-H, Hu S, Ko Y-S, Sung H-C, Huang S-Y. Skin pretreatment with lasers promotes the transdermal delivery of vitamin C derivatives. Lasers Med Sci. 2011;26(3):369-76.
30. Huang C-H, Sung H-C, Hsiao C-Y, Hu S, Ko Y-S. Transdermal delivery of three vitamin C derivatives by Er:YAG and carbon dioxide laser pretreatment. Lasers Med Sci. 2013;28(3):807-14.
31. Nguyen BT, Gan SD, Konnikov N, Liang CA. Treatment of superficial basal cell carcinoma and squamous cell carcinoma in situ on the trunk and extremities with ablative fractional laser-assisted delivery of topical fluorouracil. J Am Acad Dermatol. 2015;72(3):558-60.
32. Anbar TS, Westerhof W, Abdel-Rahman AT, Ewis AA, El-Khayyat MA. Effect of one session of ER:YAG laser ablation plus topical 5Fluorouracil on the outcome of short-term NB-UVB phototherapy in the treatment of non-segmental vitiligo: a left-right comparative study. Photodermatol Photoimmunol Photomed. 2008;24(6):322-9.
33. Lee W-R, Shen S-C, Al-Suwayeh SA, Yang H-H, Yuan C-Y, Fang J-Y. Laser-assisted topical drug delivery by using a low-fluence fractional laser: Imiquimod and macromolecules. J Controlled Release. 2011;153(3):240-8.
34. Cozzi S-J, Ogbourne SM, James C, Rebel HG, de Gruijl FR, Ferguson B, et al. Ingenol mebutate field-directed treatment of UVB-damaged skin reduces lesion formation and removes mutant p53 patches. J Invest Dermatol. 2012;132(4):1263-71.
35. Braun SA, Hevezi P, Homey B, Gerber PA. Laser-assisted drug delivery: Enhanced response to ingenol mebutate after ablative fractional laser treatment. J Am Acad Dermatol. 2015;72(2):364-5.
36. Chen W-Y, Fang C-L, Al-Suwayeh SA, Yang H-H, Li Y-C, Fang J-Y. Risk assessment of excess drug and sunscreen absorption via skin with ablative fractional laser resurfacing : optimization of the applied dose for postoperative care. Lasers Med Sci. 2013;28(5):1363-74.
37. Bhatta AK, Keyal U, Huang X, Zhao JJ. Fractional carbon-dioxide (CO2) laser-assisted topical therapy for the treatment of onychomycosis. J Am Acad Dermatol. 2016;74(5):916-23.
38. Lim E-H, Kim H, Park Y-O, Lee Y, Seo Y-J, Kim C-D, et al. Toenail onychomycosis treated with a fractional carbon-dioxide laser and topical antifungal cream. J Am Acad Dermatol. 2014;70(5):918-23.
39. Zhang J, Lu S, Huang H, Li X, Cai W, Ma J, et al. Combination therapy for onychomycosis using a fractional 2940-nm Er:YAG laser and 5 % amorolfine lacquer. Lasers Med Sci. 2016 Jun 23. [Epub ahead of print].
40. Yang C-H, Tsai M-T, Shen S-C, Ng CY, Jung S-M. Feasibility of ablative fractional laser-assisted drug delivery with optical coherence tomography. Biomed Opt Express. 2014;5(11):3949-59.
41. Rkein A, Ozog D, Waibel JS. Treatment of atrophic scars with fractionated CO2 laser facilitating delivery of topically applied poly-L-lactic acid. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 2014;40(6):624-31.
42. Mahmoud BH, Burnett C, Ozog D. Prospective randomized controlled study to determine the effect of topical application of botulinum toxin A for crow's feet after treatment with ablative fractional CO2 laser. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 2015;41( Suppl 1):S75-81.
43. Zhu J, Ji X, Li M, Chen X, Liu J, Zhang J, et al. The Efficacy and Safety of Fractional CO 2 Laser Combined with Topical Type A Botulinum Toxin for Facial Rejuvenation: A Randomized Controlled Split-Face Study. BioMed Res Int. 2016; 2016:3853754.
44. Zhou B, Zhang T, Bin Jameel AA, Xu Y, Xu Y, Guo S, et al. The efficacy of conditioned media of adipose-derived stem cells combined with ablative carbon dioxide fractional resurfacing for atrophic acne scars and skin rejuvenation. J Cosmet Laser Ther. 2016;18(3):138-48.
45. Shin M-K, Lee J-H, Lee S-J, Kim N-I. Platelet-Rich Plasma Combined with Fractional Laser Therapy for Skin Rejuvenation: Dermatol Surg. 2012;38(4):623-30.
46. Lee W, Shen S, Aljuffali IA, Li Y, Fang J. Erbium-Yttrium-Aluminum-Garnet Laser Irradiation Ameliorates Skin Permeation and Follicular Delivery of Antialopecia Drugs. J Pharm Sci. 2014;103(11):3542-52.
47. Liu C, Zhang J, Yue Y, Luo Q, Zhu D. 1064 nm-Nd:YAG lasers with different output modes enhancing transdermal delivery: physical and physiological mechanisms. J Biomed Opt. 2013;18(6):61228.
48. Menon GK, Kollias N, Doukas AG. Ultrastructural evidence of stratum corneum permeabilization induced by photomechanical waves. J Invest Dermatol. 2003;121(1):104-9.
49. Liu C, Zhi Z, Tuchin VV, Luo Q, Zhu D. Enhancement of skin optical clearing efficacy using photo-irradiation. Lasers Surg Med. 2010;42(2):132-40.
50. Lee W-R, Shen S-C, Aljuffali IA, Lin Y-K, Huang C-W, Fang J-Y. Non-ablative fractional laser assists cutaneous delivery of small- and macro-molecules with minimal bacterial infection risk. Eur J Pharm Sci. 2016;92:1-10.
51. Lim HK, Jeong KH, Kim NI, Shin MK. Nonablative fractional laser as a tool to facilitate skin penetration of 5-aminolaevulinic acid with minimal skin disruption: a preliminary study. Br J Dermatol. 2014;170(6):1336-40.
52. Bloom BS. Laser-assisted drug delivery: beyond ablative devices. Br J Dermatol. 2014;170(6):1217-8.
53. Kim TI, Shin MK, Jeong K-H, Suh DH, Lee SJ, Oh I-H, et al. A randomised comparative study of 1064 nm Neodymium-doped yttrium aluminium garnet (Nd:YAG) laser and topical antifungal treatment of onychomycosis. Mycoses. 2016. [Epub ahead of print]
54. Gómez C, Costela A, García-Moreno I, Llanes F, Teijón JM, Blanco D. Laser treatments on skin enhancing and controlling transdermal delivery of 5-fluorouracil. Lasers Surg Med. 2008;40(1):6-12.
55. Zhou HL, Hu B, Zhang C. Efficacy of 694-nm fractional Q-switched ruby laser (QSRL) combined with sonophoresis on levorotatory vitamin C for treatment of melasma in Chinese patients. Lasers Med Sci. 2016;31(5):991-5.
56. Lee M-C, Chang C-S, Huang Y-L, Chang S-L, Chang C-H, Lin Y-F, et al. Treatment of melasma with mixed parameters of 1,064-nm Q-switched Nd:YAG laser toning and an enhanced effect of ultrasonic application of vitamin C: a split-face study. Lasers Med Sci. 2015;30(1):159-63.
57. Kalil CL, Campos V, Reinehr CPH, Chaves CRP. Laser toning and drug delivery: a pilot study using laser Q-switched laser 1064nm. Surg Cosmet Dermatol. 2016; 8(2):142-6
58. Soltani-Arabshahi R, Wong JW, Duffy KL, Powell DL. Facial Allergic Granulomatous Reaction and Systemic Hypersensitivity Associated With Microneedle Therapy for Skin Rejuvenation. JAMA Dermatol. 2014;150(1):68-72.
59. De Simone C, Sisto T, Vallone S, Carbone A, Rotoli M, Amerio P. Granulomatous reaction after an aesthetic electroporation procedure. Eur J Dermatol. 2010; 20(1):135-6.
The present study was conducted at the authors' private practices in Porto Alegre (RS), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}