


Leticia Arsie Contin
Androgenetic alopecia is a condition with an important psychological impact. Clinical treatments present variable responses and require care for long periods, a factor that decreases the chances of adhesion. Microneedling with or without minoxidil injection is a new treatment modality. This study reports cases of two male patients, aged 30 and 44 years, with satisfactory partial response to four sessions of microneedling with minoxidil and three sessions of microneedling alone, using a tattoo machine and microinfusion of drugs into the skin technique.
Keywords: ALOPECIA; MINOXIDIL; NEEDLES
Androgenetic alopecia is the most common cause of follicular miniaturization, which leads to a pattern of non-cicatricial thinning of the hair.1 It affects genetically predisposed individuals and can be associated with a major impact on quality of life.2 As a result, there is great interest in the search for viable therapeutic options to assist in treating these patients.
The classic clinical approach continues to be advocated, associated or not with surgical treatments such as hair transplant. Among the used medications, the most recommended are topical minoxidil and oral finasteride.3, 4
Recent evidence has shown a possible superiority of injectable minoxidil as compared to topically applied minoxidil, yet without indication whether the optimization would be derived from the injection of the drug at a location that is closer to the follicle or from the micro-trauma inflicted, which may have an important role. 5
Microneedling was recently included in the androgenetic alopecia's therapeutic armamentarium due to the following facts: it releases platelet-derived and epidermal growth factors, it enables regeneration through wounds, it activates stem cells in the bulb and leads to the overexpression of genes related to hair growth, such as the Wnt3a and Wnt10-b pathways, and the vascular endothelial growth factor in rats. 6
Microneedling is traditionally carried out with the use of rolling cylinders with needles, which produce 1.5mm deep punctures into the scalp (rollers). 7, 8
The recently described MMP® technique (microinfusion of drugs through the skin) promotes the infusion of medicaments (drug delivery) associated with the microneedling procedure using the device for performing tattoos and appropriate needles that meet adequate principles of equipment sterilization and disposal of piercing and cutting material.9 Even when the infusion of drugs is not intended by the physician, the orifices inflicted in the skin by the device have a similar effect to that of the rollers.
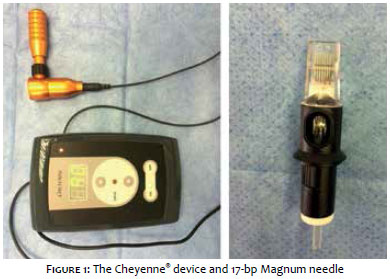
For the procedures described below the Cheyenne® brand tattoo apparatus was used (Germany, Anvisa: 80281110016). It comprises a device that allows controlling the back and forth movement's speed, and basic on and off operation buttons. The apparatus' body is connected to a power source and a tip, in which the needles cartridge (Anvisa: 80281110015) is coupled. In the present cases, the authors used 17 queued microneedles and a cartridge that allows aspiration of the medication that will be released later, during the performance of the procedure (Figure 1).
Case 1
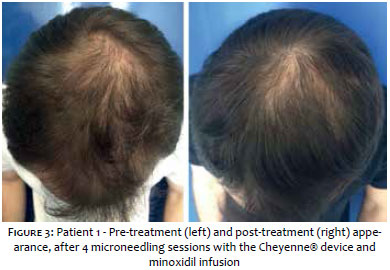
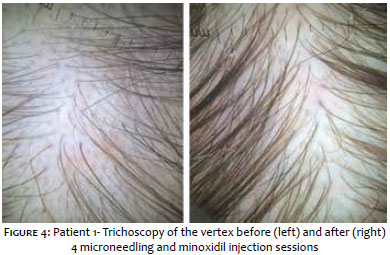
Patient "JPA": 30 years old man, with clinical and dermoscopic androgenetic alopecia diagnosis, without treatment for over a year. Has used 1mg/day finasteride for 4 years, however suspended the use of the medication 3 years before due to decreased libido and poor therapeutic response. Had previously made use of topical minoxidil for 6 months, also suspended due to the frequent forgetfulness and the poor cosmetic appearance of the medication. Does not want to undergo hair transplant at the moment. Underwent 4 monthly microneedling sessions with the infusion of minoxidil using the following technique:
- Topical anesthesia with 4% lidocaine cream (Dermomax® Laboratorio Aché, São Paulo, Brazil) was carried out 30 minutes before the procedure. After this period, the cream was removed with saline, and the antisepsis of the entire area to be treated subsequently performed with alcoholic chlorhexidine. Once the area had been completely dried, a fenestrated sterile drape was put in place delimiting the area to be treated.
- Removal of the tip from the sterilization envelope, and coupling of its distal end to the Cheyenne® apparatus, and its proximal end to the cartridge with rowed needles (model 17-bp-Magnum) (Figure 1). A small sterile container was opened for the insertion of the medication (0.5% minoxidil, injectable solution, Healthtech dispensing pharmacy, Anvisa 9003878, Rua Teresina 208/210, Vila Bertioga, São Paulo – SP, Brazil).
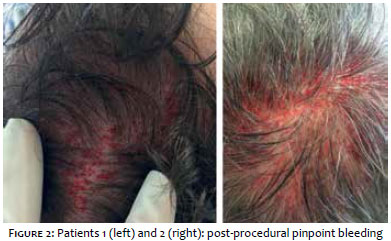
- The apparatus' speed was set at 90. The medication was aspirated from the sterile container into the cartridge just as it comes in contact with the needles by their rapid back and forth movement, when the device was turned on. The microneedling and drug delivery process was effected through the perpendicular puncturing of the epidermis, with manually adjusted depth at roughly 1.5mm. Renewed aspirations of medication are necessary when the amount in the cartridge is used up. The procedure is completed when a pinpoint bleeding is produced throughout the treated area (Figure 2). The cleansing after the procedure was performed with a gauze moistened in saline. Post-procedural care includes gentle washing with a neutral shampoo 6 hours after the procedure and the use of simple analgesics in case of local pain. Post-procedural photographs were taken 1 month after the 4th session (Figures 3 and 4).
Case 2
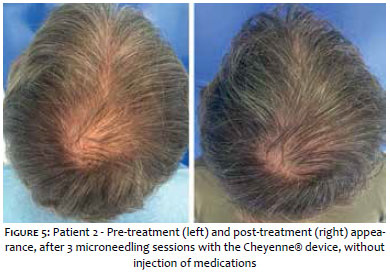
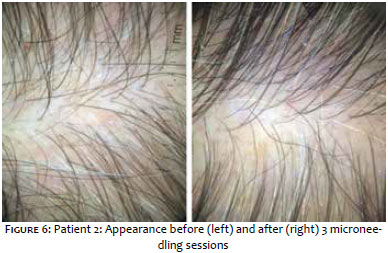
Patient "UQT": 44 years old man, with clinical and dermoscopic diagnosis of androgenetic alopecia. Regular use of minoxidil for 2 years, stable picture, with absence of improvement in the previous year. Did not tolerate the use of finasteride due to decreased libido. Underwent 3 microneedling sessions with equipment and techniques similar to those described above, however without infusion of medications. The procedure was completed when pinpoint bleeding arose (Figure 2). The post-procedural photographs were taken 1 month after the 3rd session (Figures 5 and 6).
The demand for new treatment techniques for androgenetic alopecia is growing due to the great number of patients affected and the major impact on the patients' quality of life.
The clinical treatment of the condition leads to varying – and often unsatisfactory – responses.4
The adherence to a long-term treatment can be very difficult due to the necessity of performing it daily and the medication's side effects, as in the case of the patients presented in the present study.
Options of low risk adjuvant treatments are attractive and necessary.
Pain is an important undesired side effect of the microneedling technique and MMP® in general. Although it was not significant in the present cases, it can be limiting for many patients. 10 There were no major side effects in the cases described in the present paper or in similar microneedling treatments reported previously. 7, 8
In addition to the studies that have been carried out in animals and, in lesser numbers, in humans, further evidence is necessary to prove the superiority of minoxidil injections associated with microneedling as compared to the simple topical use of the medication, to the isolated use of microneedling and to the effectiveness of the MMP® technique.
Other factors to be clarified include the required number of sessions, interval between them and maintenance.
Despite the lack of more objective evidence of improvement, there were partial and cosmetically satisfactory responses in both patients, who had few treatment options available and appropriate for their lifestyle. It is important to note that there was a considerable improvement in both cases – the one that underwent minoxidil infiltration and the other, which underwent only the microneedling process. Two sessions were necessary so that the initial improvement could be observed, therefore indicating the technique is efficient and of low complexity, with comfortable posology and that can be performed in an outpatient basis.
1. Messenger A. Male Androgenetic alopecia, In: Blume-Peytavi U, Tosti A, Whiting D, Trueb R. Hair growth and disorders. Berlin, Heidelberg: Springer, 2008. p. 159-70.
2. Torres F. Androgenetic, diffuse and senescent alopecia in men: practical evaluation and management. Curr Probl Dermatol. 2015;47:33-44.
3. Katz HI, Hien NT, Prawer SE, Goldman SJ. Long-term efficacy of topical minoxidil in male pattern baldness. J Am Acad Dermatol.1987; 16(3\ pt 2): 711-8.
4. Mella JM, Perret MC, Manzotti M, Catalano HN, Guyatt G. Efficacy and safety of finasteride therapy for androgenetic alopecia: A systematic review. Arch Dermatol. 2010;146(10):1141-50.
5. Azam MH, Morsi HM. Comparative Study Between 2% Minoxidil Topical Spray vs. Intradermal Injection (Mesotherapy) for Treatment of Androgenetic Alopecia in Female Patients: A Controlled, 4-month Randomized Trial. Egypt Dermatol Online J. 2010;6(2): 5..
6. Jeong K, Lee YJ, Kim JE, Park YM, Kim BJ, Kang H. Repeated microneedle stimulation induce the enhanced expression of hair-growth-related genes. Int J Trichology. 2012;4:117.
7. Dhurat R, Sukesh M, Avhad G, Dandale A, Pal A, Pund P. A randomized evaluator blinded study of effect of microneedling in androgenetic alopecia: a pilot study. Int J Trichology. 2013;5(1):6-11.
8. Dhurat R, Mathapati S. Response to Microneedling Treatment in Men with Androgenetic Alopecia Who Failed to Respond to Conventional Therapy. Indian J Dermatol. 2015;60(3):260-3.
9. Arbache S. Godoy CE. Microinfusão de Medicamentos na Pele através de máquina de tatuagem. Surg Cosmet Dermatol 2013;5(1):70-4.
10. Moftah N, Moftah N, Abd-Elaziz G, Ahmed N, Hamed Y, Ghannam B, et al. Mesotherapy using dutasteride-containing preparation in treatment of female pattern hair loss: photographic, morphometric and ultrustructural evaluation. J Eur Acad Dermatol Venereol. 2013;27(6):686-93.
This study was carried out at the Hospital do Servidor Público Municipal de São Paulo (HSPM) – São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}