


Ada Regina Trindade de Almeida1; Gabriel Ângelo de Araújo Sampaio2
In recent years there has been a breakthrough in non-invasive techniques of facial rejuvenation. The greater understanding of the anatomical changes involved in the aging process was accompanied by rapid evolution in how to address these changes and the expansion of substances and technologies used in this approach. Of the arsenal of substances used for rejuvenation, the upper third of the face was before an almost exclusive territory of neuromodulators. Currently, fillers have stood out, especially those based onhyaluronic acid (HA), because they are safe and produce immediate and lasting – but reversible – results. The objective of this first article is to provide a brief literature review and update on the use of HA fillers in the rejuvenation of the upper third of the face, focusing on the forehead and glabella areas.
Keywords: DERMAL FILLERS; FOREHEAD; HYALURONIC ACID
The upper third of the face comprises the area covering the hair line or the frontal muscle extension in bald patients (upper limit), eyebrows and the nasal dorsum (lower limit) and temples (lateral limits).1-3
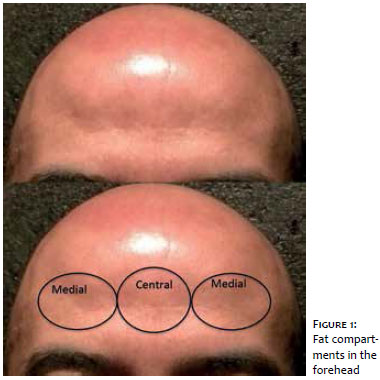
Recent studies in fresh cadavers without fixation suggest that the facial subcutaneous fat is divided into compartments separated by fibrous septa, where the vessels irrigating the skin lie. In the frontal region, there are three fat compartments: one central and two lateral (Figure 1).1-5
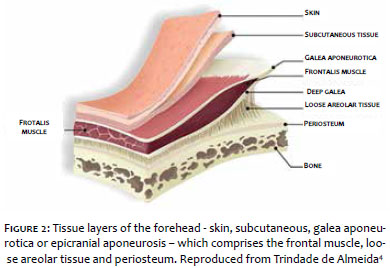
The skin in this region is thick and inelastic and in the frontal region consists of five layers: skin; subcutaneous cellular tissue; galea aponeurotica (epicranial aponeurosis, which involves the frontal muscle); loose areolar tissue and periosteum2,6– also identified by the mnemonic SCALP (Skin, Connective tissue, Aponeurosis, Loose areolar connective tissue, Pericranium). The vascular structures and nerves are mainly located in the fibrous septa connecting the subcutaneous cellular tissue with galea aponeurotica (extension of SMAS – Superficial Aponeurotic Muscle System). The loose areolar tissue is also referred to as "glide plane", as it does not provide resistance to fillers, and it is safe because does not contain vessels and nerves (Figure 2).
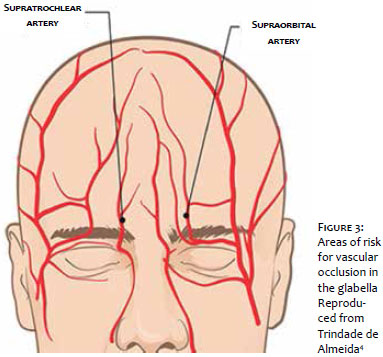
The main neurovascular bundles in this region are the supratrochlear and the supraorbital. The former is located 17-22mm away from the facial midline,7 and the latter emerges from the supraorbital foramen located in the mid-pupillary line (Figure 3).
The physical changes caused by aging are complex and not only occur in the skin – with atrophy, loss of elasticity and emergence of spots and wrinkles, but also in the soft tissues and bones, in which reabsorption and/or displacement help complete the typical characteristics of the aging process.
In the forehead and glabella aging, we can notice two main processes. Firstly, there is the emergence of lines and thin wrinkles secondary to skin thinning and repetitive muscle movements (frontal muscle and glabellar complex). Then, volume reduction takes place due to bone reabsorption, and loss or thinning of fat compartments,8 altering the youthful convexity of the forehead, which begins to show concavities in the mid third and sides. Such changes deepen the frontal wrinkles and contribute to the poor positioning of eyebrows and eyelids, which, not having the appropriate height and projection anymore, lend a tiring or aged appearance to individuals.3,9 Cosmetic dermatology specialists know that the isolated use of botulinum toxin in these cases might accentuate the eyebrow ptosis, as a result of the weakening of the frontal muscle. Volume replacement then becomes necessary for rejuvenation of the upper third of the face, recovering the natural projection and repositioning eyebrows.9
In the volume replacement of the upper third of the face, hyaluronic acid (HA) stands out as a preferred product because it is malleable and safe; produces immediate, long-lasting, although impermanent results and is reversible with the use of hyaluronidase.
Apart from volume replacement, HA has been used as a cutaneous remodeler, due to the observation of the persistence of the filling effect for much longer than the filler's bioavailability. Studies have shown that HA may induce an increase of collagen and elastic fiber production, restoring the extracellular matrix through direct stimulus and/or mechanic stretching of fibroblasts.10,11
There are a number of preparations of HA fillers with different levels of cohesiveness and viscosity. This ensures high versatility, allowing the use in both superficial and deep lines for volume replacement. Several preparations already have anesthetics added to the products, which makes the procedure easier because it becomes less painful and, therefore, more comfortable.3
In addition, although this practice is not a consensus as some authors fear to alter the filler composition, the products can be diluted right before use. Lidocaine (2%), lidocaine plus epinephrine (1:100,000) or 0.9% saline solution can be added to the HA at ratios of 20-50% (0.2-05ml of diluent for each 1ml of HA), using1-ml Luer-Lock syringes, connected by a two-output transfer device. This addition provides the product with some benefits: variation of HA concentration depending on the need (superficial lines or volume replacement) and injection plan (superficial or deep), easiness of injection due to lower extrusion force and higher malleability and dispersion into tissues, thereby avoiding irregularities. It is even believed that there may be edema reduction and lower chance of ecchymosis due to the action of the vasoconstrictor.2,9 The authors of this article use 30% dilutions, when needed.
Volume replacement:
To allow for higher comfort to patients, the authors apply topic formulations of anesthetic (Dermomax, Pliaglis, etc.) during 30 minutes prior to the procedure. Immediately before, and once asepsis with 4% alcoholic chlorhexidine has been performed.
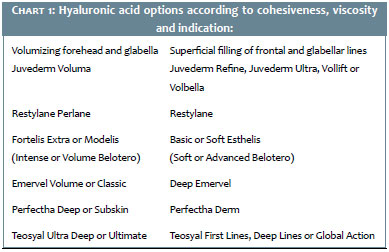
For volume replacement, a number of techniques are described. One of them is the injection of small volumes (0.2ml) into the subgaleal space (above the periosteum), where there is lower resistance to distension and absence of vessels. By using a 27G needle, we proceed with previous aspiration and deposition in perpendicular bolus in a consecutive disposition. The objective is for these deposits to work as "support towers" anteriorly projecting the forehead.2 For such, the authors prefer products with higher cohesiveness and mid viscosity that allow higher elevation of structures, lower diffusion and good tissue integration (Chart 1).
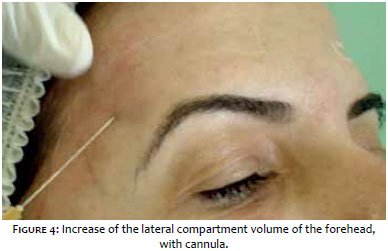
For injections into more superficial layers, the selection of a cannula, either 25G or 27G, seems to be more appropriate. The injection can be anterograde or retrograde of small volumes (0,2-0.5 ml) in both the central compartment (above the glabella) and the lateral portions (above the eyebrow), and the products may have lower viscosity and cohesiveness (Figure 4).
Massage following injection ensures better distribution of the product, elimination of irregularities and shadows, smooth recovery of the contour and forehead projection, mitigation of horizontal lines and eyebrow elevation. The required total volume ranges from 1-3ml, injected in one or more sessions and the durability of the procedure varies from 10-18 months (Figure 5).12
Another technique, known as 3D forehead reflation was described by Carruthers & Carruthers in 2015. It consists of the anterograde injection of 2-ml HA 50-100%, diluted in saline solution (total, 4ml), with cannula or needle. The total volume is divided into 1.3-ml bolus and injected into three "portals" in the forehead:1 at each outer corner of the eyebrows (next to the temporal fusion line) and 1 central, in the glabella (between the supratrochlear vessels). The higher malleability of hyperdiluted HA safely makes the massage easier and the product distribution even, with no need of multiple needle punctures or cannula movements.
In this technique, the injection is performed with a 27G or 30G needle at a 45°angle against the skin, into the superficial dermis, in small volumes (lower than 0.02 ml). In this plan, the chances of intravascular injection decrease. Because the major arteries in this region (supratrochlear, supraorbital and superficial temporal) send small branches that radially enter the deep dermis, the superficial filling should be above this layer. The best choice is products containing less reticulated, more fluid HA (Chart 1). The mean durability is 6-9 months, especially when associated with botulinum toxin (Figure 6).
Whatever filling method is used, side effects may occur, such as pain, edema and ecchymosis. Asymmetries will be corrected with massage, new HA application or hyaluronidase injections after 1 or 2 weeks, when needed.13,14
Volume replacement:
The glabella, just like other facial regions, also loses volume. This causes concavity and local wrinkle accentuation in mild cases and ptosis in more severe cases, even to the point of "collapse" of the medial eyebrow region.
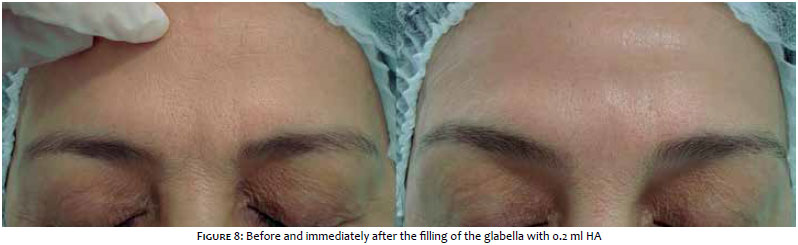
When volume replacement is the goal, the filler should be deeply deposited into the midline, into the subgaleal plane. For such, with the non-dominant hand, the skin above the procerus muscle should be clamped, forming a cutaneous fold, and the 27G needle introduced up to the supraperiosteal plane. This maneuver prevents dispersion of the filler to the sides of the nose. Aspirate before injecting. The injection is anterograde, slow, upward and then slightly lateral (radial fanning). When properly used, this technique is safe and atraumatic, as the supratrochlear arcades are 17-22mm apart from the midline at each side and angular vessels are lateral and inferior to this point. In this plane, the filler is easily spread by digital pressure toward the head, thereby preventing the formation of nodules and the need for new punctures to lessen medial frontal lines (Figures 7 and 8).
Another technique uses 25G or 27G cannulas positioned through the medial frontal compartment, craniocaudally directed or through the lateral frontal compartment up to the medial portion of the eyebrow, bypassing the orbital rim. In this step, the authors prefer products with higher cohesiveness and mid viscosity, as they allow for higher elevation of structures, lower diffusion and good tissue integration (Chart 1). The total volume used varies from 0.4-0.6ml HA, approximately, and the durability is 10-18 months.
In this procedure, the injection is performed with the use of 27G needles at a 45º angle against the skin into the superficial dermis. The application is retrograde linear or provoking whitening of the skin, known as blanching technique, with approximate total volume of 0.1ml.15 The preference is for products containing less reticulated, more fluid HA, and the mean durability is 6-9 months (when associated with botulinum toxin). Asymmetries can be corrected with massage, additional HA or hyaluronidase injections, 1 or 2 weeks later (Chart 1).
Complications that are inherent to the filling techniques have been reported, such as sporadic bleeding, ecchymosis, excessive product, superficial accumulation, formation of nodules and, more rarely, intravascular injections. Knowing the local anatomy, using careful techniques, adequate to the type of material used, with slow and resistance-free injection, in the appropriate plane may avoid such complications.
The upper third of the face is considered an area of risk, especially the glabella, due to the possibility of major vascular impairment, thereby leading to serious side effects, such as tissue necrosis and even blindness. The vascular supratrochlear and supraorbital bundles (branches of the internal carotid artery) irrigate the glabella, nasal wall, and central-inferior portion of the forehead. Tissue necrosis in these territories may occur by intravascular injection, compression by large volumes of HA and/or vascular injury, diminishing local blood supply.
Venous congestion may occur if excessive quantities are deposited in small spaces, causing persistent, disproportionate pain, as well as areas of violaceous discoloration, which might be underestimated as discomfort inherent to the procedure. The distal arterial embolization causes an immediate effect: sudden blanching of the skin with variable pain (minimum to severe), possibly followed by rectiform cutaneous darkening, formation of ulceration and eschar.
In such cases, we should immediately interrupt the procedure, massage the site and stimulate local vasodilation by applying warm compresses or nitroglycerin ointment. The use of heparin with the goal of impeding thrombotic processes or embolization has been reported in the acute phase, as well as the use of vasodilators (e.g., pentoxifylline, sildenafil, acetaminophen), antiplatelet aggregation agents, systemic corticosteroid therapy (topical and systemic) and antibiotic therapy. The abundant injection of hyaluronidase into the affected area and neighboring regions in order to reverse the process is a consensus in theliterature.16,17
Cases of blindness and amaurosis, particularly in the glabella have been reported, probably due to the retrograde diffusion of the injected material to the ophthalmic artery and its irrigation branches of the retina: central retinal artery and short posterior ciliary artery – both with documented reports in the literature.18 However, there are other hypotheses for the embolization pathway leading to blindness from (medial and lateral) forehead fillings: variation of the ophthalmic artery as a middle meningeal artery branch (branch of the external carotid), and anastomose of superficial temporal artery branches with supratrochlear or supraorbital artery. There are reports of brain ischemia due to diffusion of the injected material to the territory of the internal carotid (middle cerebral artery).
Virtually, vascular occlusions may occur at any anatomic location of the face.17 To prevent or minimize complications, the main recommendations are: deep knowledge of the local anatomy, adequate training on techniques and filling materials, attention to color variations at the treated site and complaints of pain by patients and the availability of products and drugs for immediate use, such as hyaluronidase and vasodilators.
Volume replacement allows the recovery of the natural convexity and projection of the upper third of the face, eliminating innate or acquired with aging depressions and repositioning eyebrows. Procedures are quick, on an outpatient basis, without need for tests or having to stop daily life activities. Results are effective, natural and long lasting; however, they not are risk-free and major side effects may occur. An adequate training should be recommended before any procedure.
1. Sykes JM. Applied anatomy of the temporal region and forehead for injectable fillers. J Drugs Dermatol. 2009;8(10): 24 – 27.
2. Sykes JM, Cotofana S, Trevidic P, Solish N, Carruthers J, Carruthers A, et al. Upper face: Clinical anatomy and regional approaches with injectable fillers. Plast Reconstr Surg. 2015;136(5S): 204S-218S.
3. Trindade de Almeida AR, Sampaio GAA. Preenchimentos e técnicas para o terço superior da face. In: Kadunc B, Palermo E, Addor F, editores et al. Tratado de Cirurgia Dermatológica, Cosmiatria e Laser da Sociedade Brasileira de Dermatologia; Rio de Janeiro: Elsevier, 2012. p. 355 – 60.
4. Trindade de Almeida AR, Sampaio GAA. Região frontal e Glabela. In: Sandoval MHL, Ayres E editores. Preenchedores: guia prático de técnicas e produtos. 1. Ed. São Paulo: AC Farmacêutica, 2013. p. 176-82.
5. Ramanadham SR, Rohrich RJ. Newer Understanding of Specific Anatomic Targets in the Aging Face as Applied to Injectables: Superficial and Deep Facial Fat Compartments-An Evolving Target for Site-Specific Facial Augmentation. .Plast Reconstr Surg. 2015 Nov;136(5):49S-55S.
6. Rohrich RJ, Pessa JE. The fat compartments of the face: Anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007; 119(7):2219-31.
7. Tamura BM. Anatomia da face aplicada aos preenchedores e à toxina botulínica – Parte I. Surg Cosmet Dermatol. 2010;2(3):195-204.
8. Carruthers J, Carruthers A. Volumizing the glabella and forehead. Dermatol Surg. 2010; 36(3): 1905-9.
9. Sadick NS, Dorizas AS, Krueger N, Nassar AH. The Facial Adipose System: Its Role in Facial Aging and Approaches to Volume Restoration. Dermatol Surg. 2015;4 (1):S333-9.
10. Carruthers J, Carrtuhers A. Three-dimensional forehead reflation. Dermatol Surg. 2015;41(Suppl 1):S321-S324.
11. Landau M, Fagien S. Science of Hyaluronic Acid Beyond Filling: Fibroblasts and Their Response to the Extracellular Matrix. Plast Reconstr Surg. 2015;136(5):188S-195S.
12. França Wanick FB, Almeida Issa MC, Luiz RR, Soares Filho PJ, Olej B. Skin Remodeling Using Hyaluronic Acid Filler Injections in Photo-Aged Faces. Dermatol Surg. 2016;42(3):352-9.
13. Goodman GJ, Swift A, Remington BK. Current Concepts in the Use of Voluma, Volift, and Volbella.Plast Reconstr Surg.2015 Nov;136(5):139S-148S.
14. Balassiano L, Bravo B. Hialuronidase: uma necessidade de todo dermatologista que aplica ácido hialurônico injetável. Surg Cosmet Dermatol. 2014;6(4):33843.
15. Trindade de Almeida AR. Saliba AF. Hialuronidase na cosmiatria: o que devemos saber? Surg Cosmet Dermatol 2015;7(3):197-204.
16. Sundaram H, Fagien S. Cohesive polydensified Matrix HA for fine lines. Plast Recontr Surg. 2015;136(5 Suppl):149S-163S.
17. Glaich AS, Cohen JL, Goldberg LH. Injection necrosis of the glabella: protocol for prevention and treatment after use of dermal fillers. Dermatol Surg. 2006;32(2):276-81.
18. Beleznay K, Carruthers J, Humphrey S, Jones D. Avoiding and Treating Blindness From Fillers: A Review of the World Literatur. Dermatol Surg. 2015;41(10):1097-1117.
19. Bachmann F, Erdmann R, Hartmann V, Wiest L, Rzany B. The spectrum of adverse reactions after treatment with injectable fillers in the glabellar region: results from the Injectable Filler Safety Study. Dermatol Surg. 2009;35(2):1629-34.
This study was carried out at the Dermatologic Service of the Hospital do Servidor Público Municipal de São Paulo – São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}