


Elisa Mayumi Kubo1; Carolina Ghislandi1; Carolina Tomiyoshi2; Fabiane Andrade Mulinari-Brenner3; Maira Mitsue Mukai4
Primary cutaneous nodular amyloidosis is a rare form of amyloidosis. The authors report the case of a 44-year old woman with nodules and plaques on the legs with three years of development and increase in the number and size of lesions. Clinical, histological and laboratory investigation dismissed the possibility of systemic amyloidosis, and the diagnosis of nodular amyloidosis was established. A decision was made for the surgical approach, using curettage and cauterization with good response to the proposed treatment.
Keywords: AMYLOIDOSIS; CURETTAGE; CAUTERY
Amyloidosis is a condition characterized by the abnormal depositing of amyloid in the tissue. It can be limited to the skin (primary cutaneous amyloidosis) or involve other organs and tissues (systemic amyloidosis).1-4 Among the forms of primary cutaneous amyloidosis, the macular, papular and nodular amyloidosis stand out, the latter being a rare condition that affects both genders equally, with a mean age at diagnosis of 60 years and predominantly acral clinical presentation.2 The authors report a rare case of nodular amyloidosis, with good response to surgical treatment, including curettage and electrocautery.
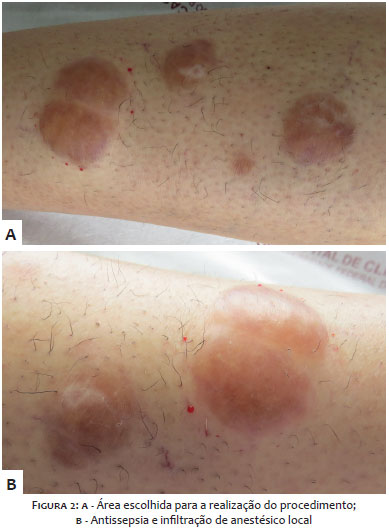
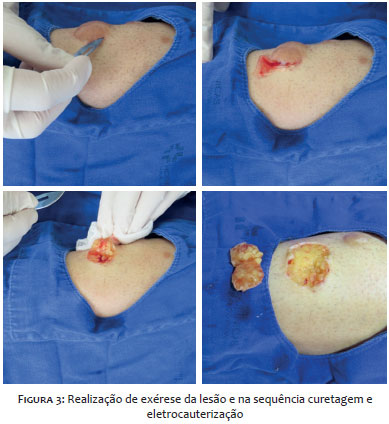
A 44 year-old, white female patient, married, housewife, originary from the city of Piraju (in the Brazilian State of São Paulo) and currently living in Curitiba (in the Brazilian State of Paraná) reported nodular lesions that emerged three years before on both legs after the use of electric epilation, progressively increasing in size and number. According to the patient description, the lesions were purplish at the onset, progressively becoming yellow-brownish at the time of the first medical consultation. She denied associated symptoms. In addition, the patient bears primary Sjögren's syndrome (diagnosed in 2010), and urinary incontinence, and uses eye drops (artificial tears) and artificial saliva. She denied the use of other medications or presence of allergies. The patient also reported having undergone cholecystectomy at twenty years of age and described two pregnancies (two normal deliveries). At clinical examination she had nodular lesions with yellow-brownish hue on the anterior side of the left and right legs, the largest measuring 5x3cm (Figure 1). Clinical hypothesis of vasculitis, Sweet's syndrome, traumatic blister and nodular amyloidosis were raised. A biopsy of the lesion on the left leg was carried out with the material being sent for histological analysis, which revealed a deposit of amyloid substance in the interstitium and around vessels (crystal violet staining) and the presence of large amounts of perivascular plasma cells. The systemic amyloidosis hypothesis was rejected after hematological investigation. Conservative treatment was initially conducted with intralesional corticosteroids interspersed with occlusive corticoid, with absence of response and dissatisfaction of the patient, who complained of local pain and discomfort. A decision was made for the surgical treatment of the lesions in the right leg (Figure 2), with curettage and electrocautery (Figure 3). The patient developed with local pain and difficult healing of the lesions (Figure 4), having been then referred to a specialized ambulatory for the nursing team care, when hydrogel, alginate and a non-adherent dressing were used locally. After the implementation of a multidisciplinary approach, the wounds presented significant improvement in the appearance, with good local healing and absence of recurrence in the primary lesions (Figures 5-7). The patient is currently receives ambulatory follow up.
In addition to being a rare entity, nodular amyloidosis is a difficult to treat condition. Therapeutic options include cryotherapy, electrocautery, curettage, CO2 laser and intralesional injection of corticosteroids,5, 6 however none of them lead to satisfactory results. The present case report describes a patient with nodular amyloidosis who progressed with difficult healing after surgical treatment. The multidisciplinary approach was crucial for the positive development of the lesions. Contrary to the results verified in the reviewed literature, the present case's outcome was satisfactory at the end of the proposed treatment.
1. Bolognia JL, Jorizzo JL, Rapini RP. Dermatologia. 2º Ed. Rio de Janeiro: Elsevier; 2011.
2. Moon AO, Calamia KT, Walsh JS. Nodular amyloidosis: review and long-term follow-up of 16 cases. Arch Dermatol. 2003;139(9):1157-9.
3. Woollons A, Black MM. Nodular localized primary cutaneous amyloidosis: a long-term follow-up study. Br J Dermatol. 2001;145(1):105-9.
4. Souza Júnior JD, Schettini RA, Tupinambá WL, Schettini AP, Chirano CA, Massone C. Localized primary cutaneous nodular amyloidosis: case report. An Bras Dermatol. 2011;86(5):987-90.
5. Konopinski JC, Seyfer SJ, Robbins KL, Hsu S. A case of nodular cutaneous amyloidosis and review of the literature. Dermatol Online J. 2013;19(4):10.
6. Zhai Z, Hao F, Song Z, Yang X. Primary localized cutaneous nodular amyloidosis of the thighs. Cutis. 2015;95(6):E24-7.
This study was performed at the Dermatology Service, Hospital de Clínicas, Universidade Federal do Paraná (UFPR) - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}