


Eckart Haneke1; Robertha Carvalho de Nakamura2; Francin Papaiordanou3; Erika Araujo Machado4; Luiza Ferreira D'Almeida4
The subungual melanoma is considered a rare subtype of melanoma. It emerges in the ungual matrix, however can involve all components of the nail apparatus. This tumor is often underdiagnosed, which leads to a delay in proper treatment, resulting in a poorer prognosis. The final diagnosis should be confirmed by histology. Conservative surgery in the treatment of subungual melanoma (when in the early stages) is presently recognized by the international literature and offers an effective and curative treatment to the patient, preserving the functional ability. This article describes a case of subungual melanoma successfully treated with conservative surgery, with the preservation of the hallux.
Keywords: MELANOMA; NAIL DISEASES; AMBULATORY SURGICAL PROCEDURES
Cutaneous melanoma is the most dangerous skin tumor, causing 90% of deaths from skin cancers.1 Subungual melanoma (SUM) is a rare subtype of melanoma, constituting 0.7% to 3.5% of all cases.1, 2 It arises from the nail matrix, however it can involve other components of the nail unit.3 This condition is often misdiagnosed, which leads to delayed proper treatment and uncertain diagnosis, especially due to the short distance of the ungual matrix to the bone. Some epidemiological data do not confirm the existence of any reasonable predisposing factor, such as genetic characteristics, family history or exposure to UV light. According to the author, there are variations. History of trauma has been described, ranging from 25% to 55%.2 Up until 2002, the gold standard treatment was excisional biopsy followed by the amputation of the finger's distal phalanx aiming at providing a margin of at least 10mm. More recent population data suggest that the in situ melanoma (with Breslow thickness < 0.5 mm) can be adequately treated with wide local excision of the entire nail unit ("en bloc")1, 2, 4, yet there is absence of high-level evidence.4
By the year 2014, the National Cancer Institute (USA) did not have guidelines for the treatment of SUM.4 The present article aims at describing a case of SUM successfully treated with conservative surgery (resection of the nail unit, with preservation of the digit).
A 67 year-old woman sought care at the Fingernail Studies Center of the Instituto de Dermatologia Professor Rubem David Azulay, of the Santa Casa da Misericordia do Rio de Janeiro (Rio de Janeiro, RJ, Brazil), presenting a longitudinal pigmented spot on the right hallux's nail that had emerged 10 years before. There was a dark, 2mm wide streak in addition to two other (narrower and lighter in color) close the nail's lateral fold (Figure 1). There was presence of Hutchinson's sign, affecting the hyponychium and the proximal nail fold. There was no family history of melanoma or other skin cancer. The patient denied previous trauma and fungal infections. The dermoscopic examination evidenced subungual Hutchinson's sign.
A lateral longitudinal biopsy was performed, containing all elements of the nail unit: hyponychium, nail bed, nail plate, matrix, proximal and lateral folds, up until there was exposure of the bone.
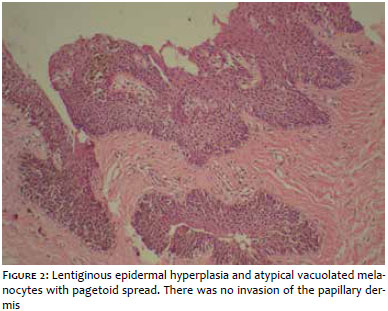
The histology revealed lentiginous epidermal hyperplasia and atypical vacuolated melanocytes spreading in a pagetoid pattern. There was no involvement of the papillary dermis. These findings were compatible with in situ lentiginous melanoma (Figure 2). After proper marking around the nail unit with a margin of 10 mm, a decision was made for the complete excision of the nail apparatus, with subsequent dissection up until the bone structure, in an attempt to preserve the patient's functional capacity. Fifteen days after the surgery, the excised site was repaired with a full thickness graft with good results. The patient was followed for 165 days, with photographic records (Figure 3). By the time the present paper was sent for publication, there were no clinical signs of recurrence.
Some differential diagnoses (benign and malignant) of SUM, should be considered by dermatologists, including: trauma, subungual keratoacanthoma, junctional nevus, warts, radio-dermatitis, squamous cell carcinoma, basal cell carcinoma, bone metastases, Bowen's disease and others.5
Levit et al. proposed a mnemonic method that facilitates diagnosis (The ABC rule for clinical detection of subungual melanoma).
Dermoscopy can be useful assisting in the differential diagnosis and facilitating the diagnosis per se however, unlike for other cutaneous sites, there are few conventional dermoscopic criteria for pigmented lesions in the nail.
The accumulation of melanin in the nail plate hampers the direct observation of the underlying nail matrix and bed. Dermatoscopes with polarized lights should not be used to examine nails due to the optical properties of the nail plate (convex shape). The use of a specific immersion gel to fill the cavities is required. Hirata et al. propose the dermoscopic examination of the nail bed and matrix, without the nail plate (assisted by a dermatoscope with polarized light) that allows the direct visualization of the pigment, revealing characteristics that can not be observed when the nail plate is interposed. As a result, this facilitates the selection of the adequate location for excisional biopsy. Nevertheless, this procedure does not substitute the dermoscopic examination of the nail plate6 and is not usually used in all dermatology services. A subtle nonetheless important dermoscopic characteristic is the triangular longitudinal streak, since the proximal end is wider than the distal end. This fact implies that the lesion is growing, which strongly suggests the presence of SUM. Other findings that lead to the suspicion of SUM are:
- pigmented streaks with more than 6mm in width7
- presence of Hutchinson's sign7
- dystrophy and ulceration of the nail plate (it is always important to bear in mind that the melanoma can be an amelanocytic lesion, thus all lesions of the nail unit must undergo histologic study)7
- brown color background and presence of irregular longitudinal lines with interruptions in its parallelism8
- blood spots observed mainly in nail bleeding (they do not rule out the presence of melanoma)8
- micro-Hutchinson sign (pigmentation with color ranging from brown to black, in the cuticle and proximal nail fold)8, 9
- irregular brown to black pigmentation and irregular thickness10
The final diagnosis should be confirmed by an appropriate histological examination. Excisional biopsies are considered the "gold standard" and are aimed at avoiding sampling errors. 2 In 2001, Clarkson et al. first described the treatment of subungual melanoma using the wide excision of the nail unit and repair with skin grafts. 6 Since then, some cases were published demonstrating the absence of recurrence after a minimum follow-up period of 2 years.1, 4, 10
The results of a histological analysis study of subungual melanomas justify that the conservative surgical treatment of early-stage lesion is possible due to the fact that the nail matrix seems to be more resistant to invasion than other structures, with late tendency of dermal invasion. Conservative resections are justified when the margins obtained are histologically free.
In conclusion, the surgical treatment of early stage subungual melanomas with wide excision of the nail unit, without amputation of the toe and followed by grafting is currently recognized by the international literature and offers safety, efficacy and resolution to the patient, preserving his or her functional capacity.
1. Garbe C et al. Diagnosis and treatment of melanoma. European consensus- based interdisciplinar guideline¬ update 2012, Eur J Cancer (2012)
2. De Giorgi et al. Specific challenges in the management of subungual melanoma. Expert Rev. Anticancer Ther. 2011: 11(5), 749¬761.
3. Sureda N, Phan A, Poulalhon N, Balme B, Dalle S, Thomas L. Conservative surgical management of subungual (matrix derived) melanona: reporto f seven cases and literature review. Br J Dermatol. 2011; 165(4): 852¬-8.
4. Cochran AM, Buchanan PJ, Bueno RA Jr, Neumeister MW. Subungual melanoma: a review of current treatment. Plast Reconstr Surg. 2014;134(2):259-¬73.
5. Levit EK, Kagen MH, Scher RK, Grossman M, Altman E. The ABC rule for clinical detection of subungual melanoma. J Am Acad Dermatol. 2000; 42(2 pt 1): 269-73.
6. Hirata SH, Yamada S, Almeida FA, Enokihara MY, Rosa IP, Enokihara MM, et al. Dermoscopic examination of the nail bed and matrix. Int J Dermatol. 2006 ;45(1):28-30.
7. Banfield CC, Dawber RPR. Nail Melanoma: A review of the literature with recommendations to improve patient management. Br J Dermatol. 1999; 141(4): 628¬-32.
8. Ronger S, Touzet S, Ligeron C, Balme B, Viallard AM, Barrut D, et al. Dermoscopic examination of nail pigmentation. Arch Dermatol. 2002;138(10):1327-33.
9. Bello DM, Chou JF, Panageas KS, Brady MS, Coit DG, Carvajal RD, et al. Prognosis of acral melanoma: a series of 281 patients. Ann Surg Oncol. 2013;20(11): 3618¬-25.
10. Bilemjian APJ, Maceira JP, Barcaui CB, Pereira FB. Melanoníquia: importância da avaliação dermatoscópica e da observação da matriz / leito ungueal. An Bras Dermatol. 2009;84(2):185¬-9.
This study was performed at the Center for the Studies of the Nail, Instituto de Dermatologia Prof. Rubem David Azulay, Santa Casa da Misericórdia do Rio de Janeiro - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}