


Adilson Costa1; Sergio Talarico Filho2; Lucia Helena Arruda3; Carla de Sanctis Pecora4; Damaris Grohmann Ortolan5; Érica de Oliveira Monteiro6; Regia Celli Ribeiro Patriota7
Introduction: Although there are differences arising from diverse formulations, botulinum toxin type A is widely marketed in Brazil.
Objective: To compare the efficacy and tolerability of two botulinum toxin type A formulations registered in Brazil: Botulinum toxin type A (Toxin 1) and Onabotulinumtoxin A (Toxin 2), in the treatment of glabellar expression lines through a multicenter prospective, comparative, randomized, double-blind study.
Methods: One hundred fifty-seven patients were randomized at a 1:1 (Toxin 1: Toxin 2) ratio for receiving 20U toxin for the treatment of the glabella's dynamic wrinkles. Photographic records were taken at maximum frowning in five protocol visits by independent evaluators. The assessment of results included: i) percentage of patients with improvement > 1 point in the four-point facial wrinkles scale, at maximum frowning, fifteen days after the treatment; ii) improvement in the static glabellar wrinkles; iii) pain and iv) duration of effect of the toxin.
Results: According to the independent evaluators, two weeks after injection, the rate of response at maximum frowning was 98.4% in the group treated with Toxin 1 and 98.2% in the group treated with Toxin 2. For individuals who received Toxin 1, the authors found an effect's duration of 84.5 ± 38.8 days, while for those who received Toxin 2, the effect's duration was 89.9 ± 41.1 days (p = 0.4303).
Conclusions: Botulinum toxin type A (Toxin 1) and Toxin 2 have similar effectivenesses in the treatment of dynamic glabellar wrinkles. Both preparations were well tolerated.
Keywords: BOTULINUM TOXIN TYPE A; WRINKLES; PROSIGNE; BOTOX
Botulinum neurotoxin inhibits the release of acetylcholine from the nerve endings, mainly acting on the cholinergic synapses.1, 2 It is widely studied both in the basic sciences and in the medical specialties (dermatology, neurology, ophthalmology and others) for the treatment of diseases and numerous aesthetic corrections.3-23
The seven different serotypes of botulinum neurotoxin (A-G) affect the human nervous system. However, type A preparations are commonly used in the clinical practice for their immunological profile, availability, duration, safety and efficacy.18, 21 Due to the fact that they are biological products, the marketed formulations of botulinum neurotoxin type A can not be considered bioequivalent or generic. The variation among the various versions generates numerous controversies about the strengths, diffusion characteristics, pain on application, effect duration and other aspects.21-24 In this manner, many studies (experimental and/or clinical) are performed to elucidate these questions. Yet, there are not answers to all questions; Nonetheless, the studies that have already been published suggest that the toxins marketed in the medical segment are effective and safe, and despite these differences, it is possible to find conversion values between them, allowing their interchange in therapeutic practice.21-23
The present study compares the efficacy and non-inferiority of the serotype A botulinum toxin Prosigne® (Toxin 1) with that of Botox (Toxin 2), paralleling the clinical performance of two different commercial applications, using a 1:1 conversion factor (Toxin 1: Toxin 2) for the treatment of dynamic glabellar wrinkles of healthy volunteers.
Research subjects
All volunteers were recruited in three research centers: the Department of Dermatology of the Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (FMUSP); Cosmiatry, Surgery and Oncology Unit (Unicco), Department of Dermatology of the Escola Paulista de Medicina da Universidade Federal de São Paulo (EPM/Unifesp); and Kolderma Instituto de Pesquisa Clínica Ltda. After having read, understood and been clarified on doubts by the study's researcher physicians, all patients included in the study signed a Free and Informed Term of Consent (FITC) before any procedure related to the study was performed. The study protocol and all material provided to patients were submitted and approved by the Research Ethics Committee (REC) of the participating centers. The present study followed the guidelines and the principles of good clinical practice standards, Brazilian National Health Council's Resolutions 196/96, 251/97 and complementary ones, and the Helsinki Declaration of 1975, revised in 2000.
The criteria for inclusion were: healthy patients, aged between 35 and 50 years, female, Fitzpatrick' skin phototypes I to IV, absence of previous use of injectable botulinum toxin, presence of dynamic glabellar wrinkles grades 2 or 3 (according to the four-point scale [0-3] glabellar wrinkles severity classification 25, and static glabellar wrinkles grades 1 or 2 at rest (using a similar rating scale). Exclusion criteria were: coagulation disorders, previous use of any formulation containing botulinum toxin, use of drugs that alter the coagulation during the seven days prior to inclusion in the study, aminoglycoside antibiotics, cyclosporine, chloroquine and hydroxychloroquine, use of D-penicillamine or any substance that interferes with neuromuscular transmission, infection at the injection site, hypersensitivity to botulinum toxin or any other component of the formulation, use of muscle relaxant medication one month before inclusion in the study, previous procedures in the glabellar region, hypermetabolism, previous neuromuscular disorder, pregnancy and lactation, history of adverse event to any drug included in this study, history of severe allergic episode, anaphylaxis, urticaria or urticaria lesion, Steven Johnson's disease, participation in a current clinical study or in the 12 months prior to inclusion, or any condition that, according to the investigator physician, rendered the volunteer inadequate to the study.
Study design
A multicentric, comparative, randomized, double-blind, non-inferiority study was performed to compare two botulinum toxins type A: Prosigne® (Toxin 1) and Botox® (Toxin 2), in the treatment of dynamic wrinkles of the glabella, in the period 2012-2014.
The primary objective was the evaluation of the improvement of at least one point in the severity scale of dynamic glabellar wrinkles, through clinical examination and photographic analysis, 15 days after the application of Toxins 1 and 2, according to three independent physicians.
As secondary objectives, the following items were evaluated:
1) duration of the toxins' effect in the treatment of glabellar dynamic wrinkles using photographic records at maximum frown, in five protocol visits (V), by independent evaluator physicians (effect duration defined as the maintenance of the improvement of at least one point on the glabellar wrinkles scale from V2 to V5);
2) evaluation of the improvement of at least one point on the severity of static glabellar wrinkles 120 days after (V5) the application of toxins 1 or 2;
3) tolerability to botulinum toxin type A using the pain visual analogue scale 26 (VAS) immediately after the application of the toxin.
The pain VAS consists in a 100mm long horizontal straight line on which the patient marks a point representing the intensity of his or her instantaneous pain. Its ends (0 and 100) correspond to the absence of and maximum pain that the patient might feel, respectively. Values less than 30mm are deemed to represent mild pain; those between 31mm to 70mm represent moderate levels of pain; values greater than 71mm correspond to severe levels of pain.
All patients underwent detailed medical history analysis and clinical examination by trained dermatologist physicians, as well as evaluation of glabellar wrinkles at rest and in motion, according to a standardized frowning scale of the region, in five visits (Day 0 [V1], day 15 [V2], day 60 [V], day 90 [V4], and day 120 [V5]). The severity assessment of dynamic glabellar wrinkles was performed using a four-point severity scale (A = 0 [absence of wrinkles], B = 1 [mild wrinkles]; C = 2 [moderate wrinkles], D = 3 [severe wrinkles]).
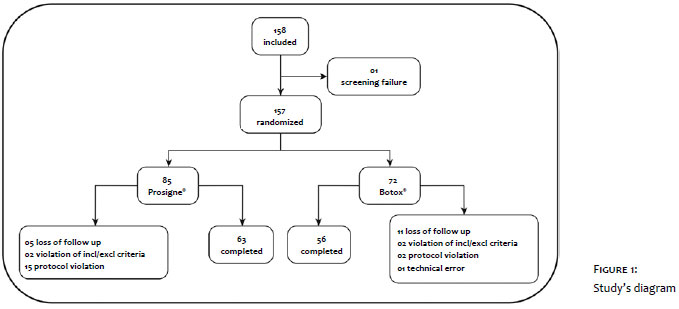
Standardized digital photographic records were taken (at rest and at maximum frowning) for each patient, before and after the treatment period and on all visits, aimed at comparing and evaluating the treatment's clinical response and side effects. The following tasks were carried out during the visits: classification of the wrinkles' severity, evaluation of the pain sensation on injection, and evaluation of patient satisfaction after the treatment. The study's flowchart is shown in Figure 1.
Randomization of patients
The patients were divided randomly into two groups, each receiving either Toxin 1 or Toxin 2, at the 1:1 ratio (one Prosigne® unit corresponding to one Botox® unit). The randomization was performed in blocks of four, using the Random Allocation Software 1.0 to allocate patients in groups.
Intervention
Each patient received a total dose of 20U of Toxin 1 or Toxin 2, in a random manner, in the glabella region (at V1).
Medicaments and injections
Toxin 1: Prosigne® (Cristália, SP, Brazil), 50U botulinum toxin type A with excipient (gelatin, dextran and sucrose). Toxin 2: Botox® (Allergan Inc., Irvine, CA, USA), 100U botulinum toxin type A with excipient (human albumin and sodium chloride), Both toxins were vacuum-packaged in sterile vials. Before dilution and application of the injection, the products were kept in the refrigerator at a temperature between 2ºC and 8ºC.
The toxins' vials were reconstituted immediately before the application. Toxin 1: 50U toxin 1, 0.5ml 0.9% sterile saline without preservatives, with a final dilution of 1U/0.1ml. Toxin 2: 100U toxin 2, 1ml 0.9% sterile of saline without preservatives, with a final dilution of 1U/0.1ml.
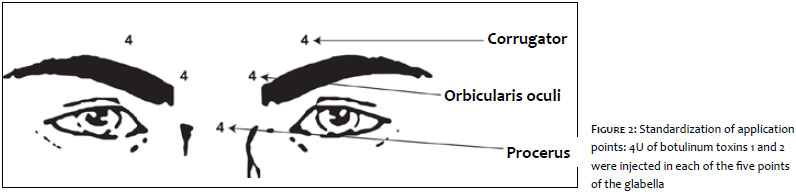
The Toxin 1 and Toxin 2 vials were reconstituted by a researcher physician, who aspirated 20 units of each product using 1ml capacity BD syringes with short needles, and delivered them to the second researcher, who performed the injections of the already diluted toxins unknowingly which product was in the syringe. The applicator physician injected the product in the volunteer's glabella according to the following protocol: 4U dose of botulinum toxin per point of injection in the treatment site (2 points in the corrugator muscles, 2 points in the orbicularis oculi muscle, and 1 point in the procerus muscle, totaling 5 points and 20U in the glabella region) (Figure 2).
Reporting adverse events
The patients were instructed to observe and report any secondary effects (duration and severity, for instance) following the injection session (V1) and at each follow-up visit (V2 to V5). They were also questioned about the presence of pain in the injection area, hematomas or any other unusual observation worth noting.
Analysis carried out by independent evaluator physicians
Three independent evaluators analyzed all photographs taken during the study and rated the severity of the glabellar wrinkles according to scale standardized for the present study. In cases of partial discrepancy in the assessment carried out by the three evaluator physicians, the patient was rated according to the majority's assessment. When there was total discrepancy between evaluations, the lowest rating was considered for the analysis of effectiveness.
Statistical study: sample size and data analysis
The sample size estimation formula for percentages of two parallel samples was used to demonstrate the non-inferiority, with a prefixed error β = 20% (Software: nQuery 4.0 PTE01a). In order to demonstrate the non-inferiority of the test substance (Toxin 1), a value was chosen that represented the greatest difference without meaning inferiority with respect to the reference product (Toxin 2), i.e. the greatest clinically acceptable difference (non-inferiority margin). Assuming that the real difference between the groups was equal to 0, with a 15% non-inferiority margin, a 5% significance and a 95% percentage of answers 15 days after the application of the products, 100 evaluable patients (50 in each group) would be enough to demonstrate Toxin 1's non-inferiority as compared to Toxin 2 for the treatment of dynamic glabellar wrinkles. Considering that possible follow up losses and other protocol violations could occur in 20% of cases, were recruited at least 120 individuals. The statistical analysis was performed with the Statistica software, using the unpaired parametric t-test and ANOVA (repeated measures' variance analysis in one factor and nonparametric Chi-square/Fisher tests, with a 5% significance level).
The homogeneity was assessed using the Levene and Tukey's unequal N HSD tests for posthoc comparisons. The sphericity was taken into account in the ANOVA calculation (Greenhouse/Geisser & Huynh/Feldt adjustments and Mauchley's test). Although this was not provided in the ANOVA's application protocol, a decision was made for using it, in order for the significance did not become inflated.
The confidence interval (95% CI) of the difference in the proportion of answerers in the two groups (improvement of at least one point in the severity of glabellar dynamic wrinkles after 15 days) was used to demonstrate the non-inferiority. The confidence interval (95% CI) for the difference in the proportion of answerers was also calculated (improvement of at least one point in the severity of static glabellar wrinkles after 120 days).
One hundred and fifty-eight female patients, aged from 35 to 50 years (median = 45 years) were included. Of these, one was excluded before the randomization and did not receive the application due to the fact she was younger than 35. As a result, 157 research subjects were randomized to receive treatment with Toxin 1 or 2. There were six losses of follow up on Visit 2 (V2) (1 linked to Toxin 1 and 5 linked to Toxin 2), because of the patients' difficulty to attend visits on the dates preset in the protocol. From V2 (15 days) to V6 (120 days), there were 16 follow up losses due to missed visits (patients were unreachable or could not follow the study's schedule). One hundred nineteen patients completed the study (56 and 63 in the research arms Toxin 1 and Toxin 2, respectively). (Figure 1)
The sample was homogeneous regarding the biodemographic data, with absence of differences between the two groups. The average age was 43.9 years for group Toxin 1 and 43.7 years for group Toxin 2.
Primary objective's results
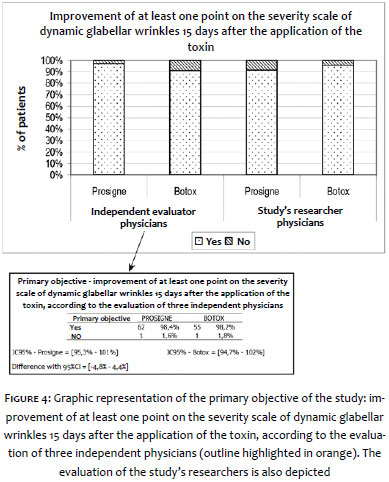
According to the opinion of the independent evaluators, both Toxin 1 and Toxin 2 were significantly effective in improving at least one point in the severity of the dynamic glabellar wrinkles 15 days after the application (Figure 3). In the present study, 98.4% and 98.2% of individuals achieved this goal in the groups Toxin 1 and Toxin 2, respectively, according to the per protocol (PP) analysis, 95% CI = [-4.8% to 4.4%]; and 97.1% and 91.0%, 95% CI = [-13.9 to 1.9%], respectively, according to the intent to treat (ITT) analysis. It was already expected that the difference between answerers of the two products would be less than 15%, which in fact was observed with the 95% CI in the PP and ITT analyses, meaning that Toxin 1 was not inferior to Toxin 2, regarding their effect on dynamic glabellar wrinkles. Likewise, the evaluation of the study's investigators found 98.4% 95 and 95.5% of patients, regarding Toxins 1 and 2 respectively, with an improvement of at least one point on the severity of dynamic glabellar wrinkles. The opinions of the independent evaluators and study's researchers coincided in 89.7% of cases receiving Toxin 1 and in 92% of those receiving Toxin 2 (Figure 4).
Secondary objectives' results
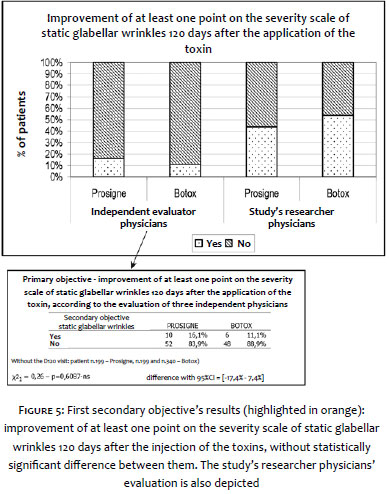
One of the secondary objectives was to evaluate the improvement of at least one point on the scale of severity of static glabellar wrinkles 120 days after the application of the toxin, according to the evaluation of three independent evaluator physicians. Only 7 patients (10, 8%) in the Toxin 1 group and 12 (17.9%) in Toxin 2 group had this level of improvement, with absence of statistically significant differences between them. In the opinion of the study's researchers, this improvement was 44.9% and 53.9% in Toxin 1 and 2 groups, respectively, with absence of statistical difference between the groups. The opinions of the study's researchers and those of the independent evaluators coincided in 58.2% of cases receiving Toxin 1 and in 46.2% of those receiving Toxin 2 (Figure 5).
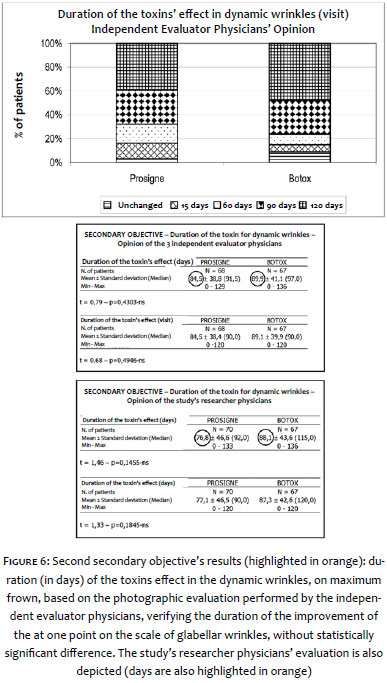
The second secondary objective was to evaluate the duration of the botulinum toxin's effect in dynamic wrinkles on maximum frown, according the evaluation of photographs carried out by the independent evaluators, verifying for how long the improvement of at least one point on the scale of glabellar wrinkles remained. For the patients who received Toxin 1, the present study found that toxin's effect duration was 84.5 ± 38.8 days, and 89.9 ± 41.1 days for those who received Toxin 2, with no statistically significant difference (p = 0.4303). In the opinion of the study's researchers, the toxin duration for dynamic wrinkles was 76.8 ± 46.6 and 88.1 ± 43.6 days for Toxin 1 and 2 groups, also with absence of statistically significant difference between the groups (p = 0.1455-nS) (Figure 6).
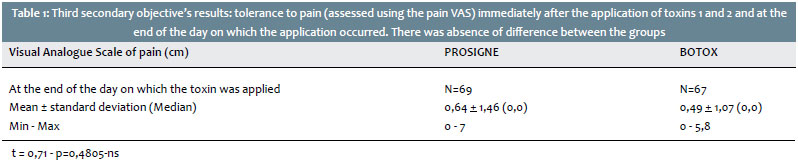
Aiming at achieving the third secondary objective, the authors of the present article studied the tolerability of the medication during the injection of Toxins 1 and 2, using a visual analogue scale (VAS) of pain immediately after the toxin application. There was absence of difference between the groups (p = 0.2839-ns). Likewise, there was no difference between the two products (p = 0.4805-ns) regarding pain at the end of the day on which the toxin was applied (Table 1).
Adverse events experienced by individuals in both groups did not differ significantly (p = 0.4507-ns) and 44.4% and 66.7% were of mild intensity, while 54.2% and 33.3% were moderate, in Toxin 1 and Toxin 2 groups, respectively. Most adverse events, such as mild pain, erythema and self-limited bleeding at the injection site, were not serious and improved spontaneously.
Serotype A botulinum toxin is a well-established option for the treatment of dynamic wrinkles of the face. The crystalline form of botulinum toxin type A has been introduced in the medical practice in 1980, for the treatment of strabismus. Since then numerous other indications have arisen, including blepharospasm, facial spasm, spasticity and diverse cosmetic uses such as dynamic facial wrinkles and hyperhidrosis (axillae, palms and other locations). 1, 3-11, 15-18
Botox® (onabotulinumtoxina A - BoNT/A) is produced in Ireland by Allergan Pharmaceuticals Ireland. In Brazil, it is imported and distributed by Allergan Produtos Farmacêuticos Ltda., São Paulo. It was the first toxin type to be marketed for cosmetic purposes and serves as a baseline in the comparison of efficacy among toxins type A. In 1988, the research team at the Lanzhou Institute of Biological Products produced and made available a highly pure and stable Chinese botulinum toxin type A, under the trade name BTX-A®.
In 1997, after pre-clinical and clinical studies, the People's Republic of China's National Committee for Drug Evaluation approved its use for medical treatment, specifically for: hemifacial spasm, blepharospasm and strabismus. 5-9 In Brazil, the National Health Surveillance Agency (ANVISA) approved BTX-A® for clinical use in 2003, and for cosmetic use in 2005, under the trade name Prosigne®. The product is currently marketed in Brazil (by Cristália Produtos Químicos Farmacêuticos Ltda., São Paulo) and in many European countries, Asia and America.
Botulinum toxins are biological products, meaning that the concept of bioequivalence of different formulations does not apply; nevertheless it is possible to interchange commercial formulations among them in light of the results of comparative clinical trials of these different products. In this manner, the present study provided valuable data for the understanding of the botulinum toxin type A Prosigne® (Toxin 1) in comparison to that marketed under the trade name Botox® (Toxin 2).
The present study achieved its primary objective of improvement of at least one point on the severity scale of glabellar dynamic wrinkles, 15 days after the injection of Toxin 1 or 2, according to the evaluation of three independent physician evaluators. In this way, 15 days after the treatment, both toxins were significantly effective in improving at least one point on the severity scale of dynamic glabellar wrinkles, according to the opinion of the independent evaluators and the study's researchers. It was expected that the difference between answerers in the two groups would be less than 15%, a fact that materialized in light of the 95% CI, both in the PP and in the ITT populations. In addition, the fact that there was agreement between the evaluations of the independent evaluators and that of the study's researchers stands out.
Moreover, the study brought other relevant information to light linked to the fact that one of the secondary objectives was to evaluate the improvement of at least one point on the severity scale of static glabellar wrinkles, 120 days after the toxin application, according to the evaluation of three independent physician evaluators.
The second secondary objective was to evaluate the duration of the botulinum toxin effect in dynamic wrinkles on maximum frown through the independent analysis of photographs by independent physicians, verifying the duration of the improvement of at least one point on the severity scale of glabellar wrinkles. On this front, there was no statistically significant difference, in the opinion of both the study's researchers and the independent evaluators.
The third secondary objective was to evaluate the tolerability to the medications during the injection of Toxins 1 and 2, according to a pain VAS, immediately after the application of the toxin. No difference was observed between the groups. Also, no difference was evidenced between the two products regarding the pain sensation at the end of the day on which the application of the toxin was performed.
Adverse events experienced by individuals did not differ significantly between the two groups. Most were not serious, being of mild or moderate intensity. Among them were mild pain, erythema and self-limiting bleeding in the injection site, which improved with local manual compression. This is aligned with events that have been observed in several studies, in which the intramuscular injection of any substance possibly caused local pain, abnormal sensitivity to compression, hematoma or ecchymosis formation and/or local injury. These are all mild and expected events.
The present study's findings, together replicate the results of other controlled clinical studies comparing Botox® and Prosigne®, showing that the formulations are equivalent in the treatment of blepharospasm and hemifacial spasm, cervical dystonia, hyperactivity of the detrusor muscle and spasticity. 18, 20, 22-24
Te results of the comparative analyses have shown that Toxins 1 and 2 are equally effective and safe in improving at least one point on the severity scale of dynamic glabellar wrinkles 15 days after the application, in the opinion of both the study researchers and the independent evaluator physicians.
We would like to thank the sub-investigators who participated in this study: Edileia Bagatin, Karime Hassun, Renata Valente Carneiro, Ana Paula Mayumi Takeuchi, Camila Anna Hofbauer Parra and Vivian Barzi Loureiro.
1. Scott AB, Rosembaum A, Collins CC. Pharmacologic weakening of extraocular muscles. Invest Ophthalmol. 1973;12(12):924-27.
2. Wang YC, Zhuang H, Huang BG, Dai Z. Preparation of type A botulinum crystalline toxin for the therapeutic and establishment of an experimental animal model. Chinese J Biologicals. 1990;3(3):121-5.
3. Scott AB. Botulinum toxin injection into extraocular muscles as an alternative to strabismus surgery. Ophthalmology. 1980;87(10):1044-9.
4. Carruthers JD, Carruthers JA. Treatment of glabellar frown lines with C. botulinum-A exotoxin. J Dermatol Surg Oncol. 1992;18(1):17-21.
5. Schantz EJ, Johnson EA. Properties and use of botulinum toxin and other microbial neurotoxins in medicine. Microbiol Rev. 1992;56(1):80-99.
6. Dai Z, Wang YC. Treatment of blepharospasm, hemifacial spasm and strabismus with botulinum A toxin. Chin Med J. 1992;105(6):476-8.
7. Dai Z, Lu W, Wu X, Li ZH, Zhang FH, Wang YC. Phase II Clinical Trial of Treatment of Blepherospasm, Hemifacial Spasm with Botulinum Toxin Type A for injection. Chin J Ophthalmology. 1993;29(3):144-145.
8. Zhao CD, Chen HX, Nie ZM. A clinical study of botulinum toxin type A in treatment of blepharospasm and facial spasm. Chinese J Nervous Mental Diseases. 1996;22(2):83-85.
9. Zhang LJ, Feng XL, Zhang SM, Shen ZL, Shi SY. A study on botulinum toxin A in treatment of blepharospasm and facial spasm. Shaanxi Medical Journal. 1998;27(1):50-1.
10. Wan X, Tang X, Cui L. Remote effects of local injection of botulinum toxin type A. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 1999;21(5):362-7.
11. Keen M, Blitzer A, Aviv J, et al. Botulinum toxin A for hyperkinetic facial lines: results of a double-blind, placebo-controlled study. Plast Reconstr Surg. 1994;94(1):94-9.
12. Foster JA, Barnhorst D, Papay F, Oh PM, Wulc AE. The use of botulinum A toxin to ameliorate facial kinetic frown lines. Ophthalmology. 1996;103:618-22.
13. Klein AW. Complications, Adverse Reactions, and Insights with the use of botulinum toxin. Dermatol Surg. 2003;29(5):549-56.
14. Kimura J. Disorders of neuromuscular junction, myophaties and abnormal muscle activity. In: Kimura J. Electrodiagnosis in Diseases of Nerve and Muscle - principles and practice. Philadelphia: FA Davis; 1985. p.511-26.
15. Dimitrova DM, Shall MS, Golderg SJ. Short-term effects of botulinum toxin on lateral rectus muscle of the cat. Exp Brain Res. 2002;147(4):449-55.
16. Monteiro EO. Uso avançado da toxina botulínica do tipo A na face. RBM Rev Bras Med. 2009; 66(Supl 4).
17. Talarico-Filho S, Bagatin E, Monteiro EO, Pinheiro MVB, Hassun KM. Eficácia e segurança da neurotoxina botulínica tipo A no tratamento de linhas de expressão glabelares. RBM Rev Bras Med. 2008;65(esp), 28-33.
18. Ferreira LM, Talarico-Filho S, Costa RO, Godoy A, Steiner D, Fleissig L, et al. Eficácia e tolerabilidade de uma nova toxina botulínica tipo A para tratamento estético de rugas faciais dinâmicas: estudo multicêntrico prospectivo de fase III. Surg Cosmet Dermatol. 2009;1(2):58-63.
19. Quagliato EM, Carelli EF, Viana MA. Prospective, randomized, double-blind study, comparing botulinum toxins type a botox and prosigne for blepharospasm and hemifacial spasm treatment. Clin Neuropharmacol. 2010; 33(1): 27-31.
20. Lacy DB, Tepp W, Cohen AC, DasGupta BR, Stevens RC. Crystal structure of botulinum neurotoxin type A and implications for toxicity. Nat Struct Biol. 1998; 5(10): 898-902.
21. Peng L, Berntsson RP, Tepp WH, Pitkin RM, Johnson EA, Stenmark P, et al. Botulinum neurotoxin DC uses synaptotagmin I and II as receptors, and human synaptotagmin II is not an effective receptor for type B, DC and G toxins. J Cell Sci. 2012; 125(13):3233-42.
22. Sattler G, Callander MJ, Grablowitz D, et al. Noninferiority of incobotulinumtoxinA, free from complexing proteins, compared with another botulinum toxin type A in the treatment of glabellar frown lines. Dermatol Surg. 2010; 36(Supl 4):2146-54.
23. Yoon JS, Kim JC, Lee SY. Double-Blind, Randomized, Comparative Study of Meditoxin® Versus Botox® in the Treatment of Essential Blepharospasm. Korean J Ophthalmol. 2009; 23(3):137-141.
24. Rieder CR, Schestatsky P, Socal MP, Monte TL, Fricke D, Costa J, et al. A double-blind, randomized, crossover study of prosigne versus botox in patients with blepharospasm and hemifacial spasm. Clin Neuropharmacol. 2007; 30(1):39-42.
25. Honeck, P, Weiss C, Sterry W, Rzany B. Clinical and Laboratory Investigations Reproducibility of a four-point clinical severity score for glabellar frown lines. Br J Dermatol. 2003; 149(2): 306-10.
26. Jensen MP, Miller L, Fisher LD. Assessment of pain during medical procedures: a comparison of three scales. Clin J Pain. 1998;14(4):343-9.
This study was performed at the following entities: Kolderma Instituto de Pesquisa Clínica Ltda; Cosmiatry, Surgery, Oncology and Laser Unit (Unicco), Dermatology Departament of the Escola Paulista de Medicina da Universidade Federal de São Paulo; Dermatology Departament, Hospital das Clínicas, Faculdade de Medicina da Universidade de São Paulo (FMUSP) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}