


Leandra D’Orsi Metsavaht
Patients with scars often seek dermatologists for improving the symptoms (pruritus, pain), aesthetics and functionality (for example, to improve the range of motion in the joints). After anamnesis and description of the scar, the patient should be informed about the best repair techniques, based on scientific evidence and the physician's personal experience. The authors describe the main surgical techniques to treat scars, such as Z-plasty, W-plasty, dermabrasion, among others
Keywords: CICATRIX; SURGERY; DERMABRASION
After surgery or trauma, preventing the formation of abnormal scars is the priority. In the case of surgical procedures, prevention starts before surgery, extending intraoperatively.1-3
The goal is always to make the scar to become as unnoticeable as possible, paralleled to cutaneous folds and tension lines, leveled with the surrounding skin, not producing any distortion, and similar in color to the adjacent tissues. If located in the face, it should be on the periphery, in the transition area between two cosmetic units or directly on the midline.1-3
Preventing the occurrence of a pathological scar is undoubtedly more effective than treating one. To avoid any unnecessary wound, with the patient being prone or not to hypertrophic scars or keloids, seems an obvious solution, however this is not always feasible.2
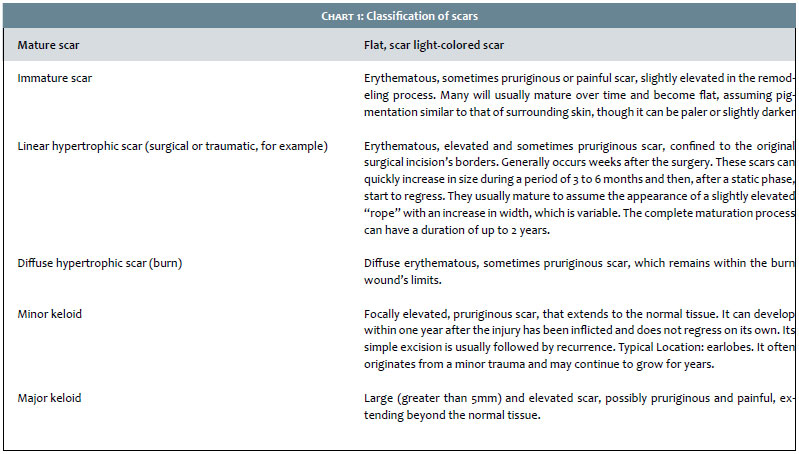
According to the International Advisory Panel on Scar Management, scars can be classified as mature, immature, linear hypertrophic, widespread hypertrophic scars, minor keloid and major keloid.1
SCAR BEARING PATIENT ANAMNESIS
Most patients are not able to define precisely what a scar is, nevertheless they know when it does not look good and has changed its physical appearance. The patient's subjective opinion arises as a standard for judging the success or failure of any procedure. Currently, some measurement scales assist physicians to gauge the degree of patient satisfaction regarding the appearance of his or her scars. The Vancouver Scar Scale (VSS) is quite complex and requires precision equipment for taking some measurements. The Visual Analog Scale (VAS) is simpler and more practical.2, 4
In cases of surgical revision of scars, it is important that the surgeon prepares patients for the surgeries' outcomes, describing the procedure as an attempt to modify, adjust, reposition, improve or repair a scar. It is also useful to clarify what is the actual patient's dissatisfaction with his or her scar: if it is linked to the aesthetics; if there is pain, pruritus, tightness or some other local discomfort; if there is dysfunction (for example in burn scars in the axillary region, where there is retraction, leading to difficulty in abducting the upper limb). Scars may also have associated emotional factors (for example, the recollection of an accident), causing patients to desire to erase unpleasant memories or even try to improve the appearance of a scar to impress a girlfriend or ask for a promotion. 2
Scars are differentiated by their size, contour deviations, tension, color, texture, pattern, direction, and by the way they blends to adjacent tissue. Among the useful descriptive terms for the clinical analysis of scars are: location, direction relative to the skin's tension lines, level (elevated, depressed or atrophic), maturation (mature, hypertrophic or keloid), color (hypo- or hyperpigmented), texture, shape (trapdoor, network, star or linear), length and width (Chart 1).5
After performing the scar's anamnesis and description, it is necessary to explain the best techniques to the patients, based on scientific evidence and surgical experience.
Some issues should be considered during the preoperative anamnesis:
1- Patients with unrealistic expectations
It is important to highlight that the surgical revision will improve, however not erase the scar, and several surgical procedures might be necessary in order to obtain the best result, which can take months or years. 1
2- Necessary time for the surgical revision of a scar
Due to the continuous collagen remodeling, it takes roughly 12-18 months for a scar to become mature and attain between 70% and 80% in elasticity. Immature scars are prone to hypertrophy and lead to bad results after surgical revisions. Nonetheless, if an early intervention is necessary, it is most advisable that it be performed after a period of 8 to 12 weeks in adults, and 6 months for children under seven years of age.1
3- Nutritional aspects and history of medication use
A balanced diet is essential for the synthesis of proteins, which may affect the cicatrization process in vegan (lacto-egg restricted) and vegetarian individuals. In addition, patients adhere to complex anticoagulation schemes with increasing frequency. There is much controversy, however dermatologic surgery in general bears low risk, and major and fatal bleedings resulting in the reduction of the hematocrit are extremely rare. However, the consequences of thrombotic events (strokes, myocardial infarction, pulmonary embolism) in a context of discontinuation of anticoagulants are devastating. For most cutaneous procedures, the necessary anticoagulation (for secondary prophylaxis of thrombotic events) should not be discontinued perioperatively. The risk of a major bleeding or complications resulting from dermatologic surgery does not increase in patients taking aspirin or warfarin. Generally, the risk of bleeding is considered greater in the presence of antiplatelet agents than of anticoagulants. The guidance of a general practitioner or cardiologist, as well as the realization of at least one coagulogram, should always be considered.1, 2
4- Smoking habits
Tobacco causes hypoxia, thrombogenesis, vasoconstriction, aberrant cell function and delayed wound healing.
It is recommended that patients stop smoking during the four weeks prior to surgery and do not resume the habit for the following four weeks, aiming at achieving a better healing and results. 1
PHASES OF THE HEALING PROCESS AND BIOCHEMICAL ALTERATIONS
The healing process occurs in three phases: inflammatory, proliferative and repair or maturation, however some authors have suggested a more complete classification, dividing the process into five main phases: coagulation, inflammation, proliferation, wound contraction and remodeling. 6
The inflammatory phase starts immediately after the wound is inflicted, with the release of vasoconstrictor substances, especially thromboxane A2 and prostaglandins, by the cell membranes. The injured endothelium and platelets stimulate the coagulation cascade in order to attain hemostasis. The granules released by platelets contain transforming growth factor beta (TGF-β), platelet-derived growth factor (PDGF), fibroblast growth factor (FGF), epidermal growth factor (EGF), prostaglandins and thromboxanes, which attract neutrophils to the wound, helping in the bacterial destruction. They are gradually replaced by macrophages after a period of 48 to 96 hours, and figure as the main cells before fibroblasts migrate and start to replicate. They play a fundamental role in ending the debridement that was started by neutrophils, and their greatest contribution is the secretion of cytokines and growth factors, in addition to their participation in the angiogenesis and fibroplasia processes, and extracellular matrix synthesis - crucial developments regarding the transition into the proliferative phase. 6, 7
The proliferative phase consists of four basic steps: epithelialization, angiogenesis, granulation tissue formation and collagen deposition. It starts approximately on the fourth day following the injury has been inflicted and lasts approximately up to the end of the second week. If the basal membrane is untouched, the epithelial cells migrate upwards, and the normal layers of the epidermis are restored in three days. If the basal membrane has been damaged, the epithelial cells located in the edges of the wound begin to proliferate in an attempt to restore the protective barrier.6, 7
Delayed epithelization (after 10 to 14 days) dramatically increases the incidence of hypertrophic scarring. Therefore, it is mandatory to achieve a rapid healing in order to prevent the formation of excessive scarring. 6, 7
Angiogenesis is stimulated by the tumor necrosis factor alpha (TNF-α), being characterized by endothelial cell migration and formation of capillary, processes that are fundamental for the adequate healing.6, 7
The final part of the proliferative phase is granulation tissue formation, with fibroblasts and endothelial cells being the main cells figuring in this stage. The fibroblasts migrate from the surrounding tissues to the wound; nevertheless they must be activated in order to leave their state of quiescence. The most important growth factor for the activation and proliferation of fibroblasts is the PDGF. Transforming growth factor β is then released, stimulating fibroblasts to produce collagen type I and to transform into myofibroblasts, which promote wound contraction. 6, 7
Among growth factors involved in the healing process, some are noteworthy: PDGF (induces cell proliferation, chemotaxis and matrix synthesis), EGF (stimulates epithelialization), TGF-α (transformer growth factor alpha, responsible for the angiogenesis and epithelialization), fibroblast factor (stimulates cell proliferation and angiogenesis), and TGF-β (responsible for the increase in matrix synthesis).6, 7
The fact that the deposition of collagen occurs in an organized way, turns this process into the highest clinically important step in the maturation or remodeling phase. The collagen that is initially produced is thinner than that present in normal skin and is oriented parallel to the skin. Over time, the initial collagen (collagen type III) is reabsorbed and a thicker collagen is produced and arranged along the tension lines. These changes are reflected in increased tensile strength of the wound. The reorganization of the new matrix is an important process of healing. Fibroblasts and leukocytes secrete collagenase, promoting the lysis of the old matrix. The best healing occurs when there is balance between the synthesis of new matrix and the lysis of the old one. Even one year after the wound will present less organized collagen than that of healthy skin, and the tension force will never return to 100%, reaching about 80% three months after.6, 7
FACTORS THAT INFLUENCE THE HEALING PROCESS
Wounds subject to tension as a result of movement, specific body site and loss of tissue are particularly at increased risk of hypertrophic scarring. In this manner, in case of cutaneous damage, it is important to perform the primary closure early and under low or inexistent tension. Large sized wounds have increased tension in the closure. Also, the proper debriding of contaminated wounds is crucial, for the infection hampers the healing process. Other important steps are: to promote a good hemostasis, manipulate the tissue gently, limit the presence of foreign bodies in the form of debris (washing the wound thoroughly with saline to remove all devitalized tissue and debris) and avoid using braided polyfilament suture materials like silk, which causes severe tissue reaction. Wounds that coincide with the skin's tension lines experience better healing than those that are misaligned with them. Electrocautery should be minimal near the wound's borders. Before closure, all dead space should be obliterated and the traumatized edges of the wound, excised.1-3, 8, 9
Favorable locations for a good healing include: eyelids, pre-auricular region and forehead. Unfavorable locations include: nasal tip, mentum, chest area, shoulders, dorsum and lower limbs. The differences in the healing process are linked to the skin's level of tension and thickness, and number of sebaceous glands in the body region.1-3, 8, 9
Children develop worse scars than those of elder patients due to the presence of a higher content of elastin in the skin, which leads to increased tension on the skin's edges. Patients with systemic diseases, such as diabetes mellitus and chronic renal failure, or those using immunosuppressants are more susceptible to infections and poor wound healing.1-3, 8, 9
TECHNIQUES FOR THE SURGICAL REVISION OF SCARS
There is a great diversity of closure techniques, which can vary from a simple primary elliptical closure to a complex advancement flap. The elliptical fusiform closure can be the first choice in the repair of a scar aligned with tension lines, however it usually results in a longer scar and can lead to recurrence in the case of keloids and hypertrophic scars.1-3, 8
Z-PLASTY
The first study on the Z-plasty was published by Horner in 1837. This technique is currently the most popular for the revision of scars. It is often used to stretch scars that have contractures.1-3
Based on geometrical principles, it consists in a double transposition flap, where the scar to be excised is located along the central axis of the Z, with two peripheral parallel axes. After implementing the transposition, the central axis will become perpendicular to the original center's axis, and the scar will assume a more favorable position regarding the tension lines. Indications for the Z-plasty: scars that form angles in excess of 30º with the skin's tension lines, those presenting retraction and those with "spider web" shape. Using the Pythagorean theorem, Limberg demonstrated in 1929 the theoretical gains from Z-plasty. In practice, however, the gains in length are smaller due to the tissue's elasticity. Thus, wider angles lead to higher gains in length; however this implies in a reduction of the scar's width, entailing the creation of an inadequate transversal tension. The flaps are designed with angles ranging from 30º to 75º. Angles less than 30º might cause the necrosis of the tip while angles greater than 75º produce flaps that are difficult to rotate, leading to the formation of "dog ears" in addition to increased tension. The optimal angle to be used is 60º.1-3, 8, 10, 11
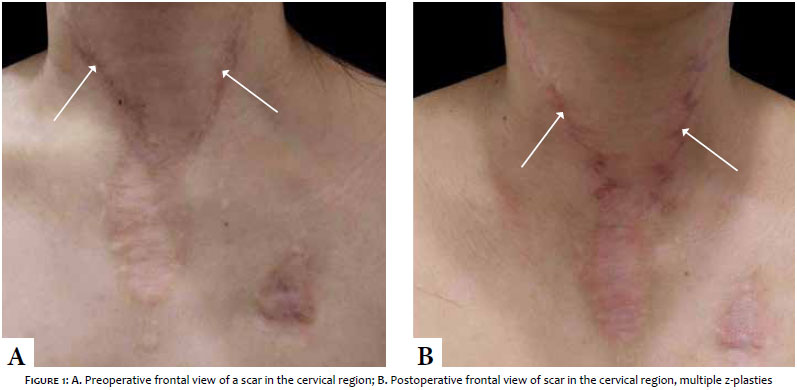
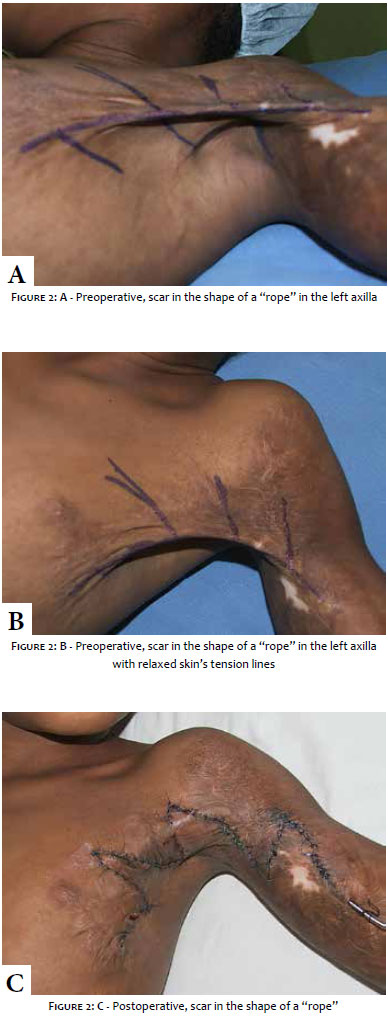
There are advantages in performing several Z-plasties - rather than a single one - along the scar's entire length (Figures 1 to 2).
Advantages
- The scar becomes irregular, therefore becoming less visible than a single straight line.
- It generates multiple different tension vectors, which helps preventing the scar's widening and contracture
- There is less need for long peripheral axes
- More length can be obtained with less transversal shortening
Disadvantages
- The scar becomes longer
- There are at least two additional scars
- At least one portion of the final scar might be positioned along the tension lines
Variations of the Z-plasty
Two opposing Z shapes, as in mirrored images. The Z shaped incisions are performed in opposite directions, and the flaps are interposed. It offers the advantage of a significant elongation in areas of limited availability of skin, release of canthal membranes or cicatricial contracture.1-3, 8 Unequal triangles (asymmetrical Z-plasty): areas of variable cutaneous elasticity, such as the scars' ends, can be revised using uneven triangular flaps by changing the angle. The Z's "arm" falling on the less elastic side is made to be longer than the other. 1-3, 8
HALF Z-PLASTY
It is used when the adjacent skin in one of the scar's sides is elastic while the other is not. The inelastic side is removed via an incision aimed at releasing the scar, while a triangular flap on the normal side is transposed in order to fill the defect created. It is particularly useful to release scar contractures at the interface between normal and cicatricial skin.1-3, 8
FOUR-FLAP Z-PLASTY (Limberg FLAP)
The angles of the Z on both of the scar's ends are kept at 90º and then each flap is sub-divided into 45º flaps. The four-flap Z-plasty has the advantage of a providing a significant gain in length and is particularly interesting for the release of severe scar contractures that hamper or limit the normal flexing, such as in the case of the first interdigital space's skin or in axillary contractures after burns.1-3, 8
PLANIMETRIC Z-PLASTY
In this case, the central Z-plasty's incision is prolonged, and the technique is used to interrupt the scar and stretch the skin into a flatter surface. The triangle created by the Z shape is dissected and undermined in order to be used as a graft.1-3, 8
S-PLASTY
It is used for the treatment of oval contracted scars when large triangular transposition flaps are required - for example, in tracheostomy sequels. The final rounding of the flap ensures a better outcome for the scar.1-3, 8, 11
W-PLASTY
It was created in 1937 - 100 years after Z-plasty emerged - by Ombrédanne aimed at improving irregular linear scars, in which most of the axes are aligned with the tension lines. In W-plasty, a certain amount of normal tissue is excised with the scar. The final outcome consists of an irregular scar, so that multiple Ws are aligned side by side.1-3, 8, 11, 12
Indications
- Short scars perpendicular to the tension lines
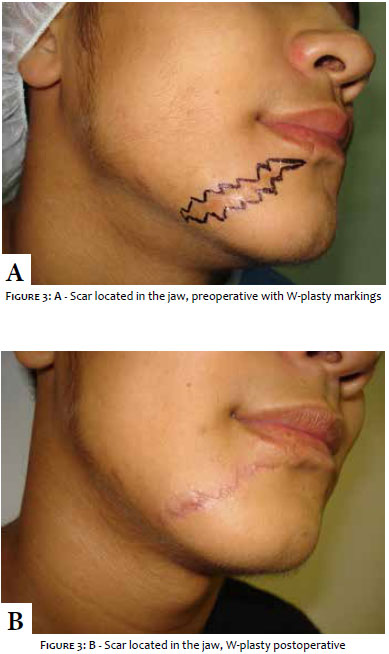
- Scars/incisions on curved surfaces like the jaw
- Scars/incisions in concave areas
W-plasty should only be performed in areas where there is no lateral laxity of tissues, for example on the forehead, temples, chin, cheeks etc (Figure 3).
W-plasty consists of several small triangular advancement flaps on both sides of the scar so that the closure occurs by interposition, projecting the "W" shaped flaps in a way to prevent the formation of "dog ears", which can be difficult to execute. Shortening the "W"'s axes as it gets closer to the excision's ends contributes for a good closure. The terminal portion should be conceived in a way to produce a 30º angle on each extremity. Alternatively, a fusiform excision can be performed perpendicularly to the terminal "arm" of the W at each end.1-3, 8, 11, 12
ADVANTAGES
- Easy to plan and execute
- Breaks down a straight scar in several small segments, many of which are located along the lines of tension
DISADVANTAGES
- A surplus of surrounding tissue is necessary
- The regular repetitive pattern causes the scar to be visible
- The scar may become longer
GEOMETRIC BROKEN LINES
Designed to convert a long linear scar into a randomly irregular scar. Interdigitating geometric lines are drawn so that the triangles, rectangles, squares and even semicircles are created on both sides of the scar at random. Most of the lines should be along the tension lines. After excision along these lines, the advancement flaps on both sides interdigitate to create a randomly irregular scar. As it should be made in W-plasty, the ends must be closed using a 30º angle in order to avoid the formation of "dog ears", which may occur if wider angles are used. Alternatively a fusiform excision can be carried out at the end, perpendicular to the terminal axis of the excision.1-3, 8, 11
Advantages
- It has all the advantages mentioned above, which are linked to the break down of a linear scar into several small segments
- Furthermore, the random irregular pattern causes the scar to be less visible than one that underwent W-plasty or multiple Z-plasties.
Disadvantages
- It is difficult to plan and implement
- The excision of normal tissue implies that it must be performed in areas where there is excess sagging from peripheral tissues
V-Y PLASTY AND V-Y ADVANCEMENT FLAP
These techniques are indicated for stretching scars in cases of small contracted scars, improving the "trap door" type deformities, and the elevation or depression of the free margin - as in the eyes and mouth - in case a scar causes ectropion or eclabium, respectively. An anatomical point can be raised or depressed using the V-Y repair.1-3, 8, 11
A V shaped incision is made along the contracted scar, followed by an extensive dissection aimed at releasing the scar and aid in the contraction of the wound's base. The V shaped flap is pulled toward the open portion of the V and the defect is closed side-to-side in the shape of a Y.1-3, 8, 11
Another use for the V-Y plasty is wound closure after excision of circular or oval defects, especially in hairy areas, such as the scalp and brow. In these areas, the Y's "arms" are camouflaged by the presence of hair.1-3, 8, 11
SUBCISION AND CUTANEOUS FILLING
Some scars become very depressed due to loss of subcutaneous tissue or fibrosis. In such cases, the rupture of fibrous septa with a 16 or 18G or Nokor needle can be a good option.1-3, 8, 11
Cutaneous filling with autologous fat or hyaluronic acid can be performed subsequently.1-3, 8, 11
THE TREATMENT OF EXTENSIVE SCARS IN MULTIPLE STAGES
Wide scars, such as those resulting from burns, might not improve with a procedure carried out in single step, like a primary closure. These scars need to be treated with a number of excisions or with cutaneous expanders.1-3, 8, 11
DERMABRASION
Dermabrasion dates from 1,500 B.C., when sandstone was used to revise scars in Egypt. Its use for correcting acne scars was very popular, when Yarborough demonstrated it could also be used in the surgical treatment of scars. The ideal Fitzpatrick skin phototypes for this procedure are I to III. Modern dermabrasion is performed using a power source, and a handpiece, where a diamond fraise or a brush is coupled. Manual dermabrasion can be performed with sterile wet sandpaper. It removes the epidermis and superficial dermis, leading to the re-orientation of collagen fibers, which become parallel to the wound's tension lines, with improvement of the scar's contour after the procedure.1-3, 8, 11
The ideal timing for undergoing dermabrasion is 6 to 12 weeks after the injury has been inflicted. At this timepoint, the wound will have adequate tensile strength, and collagen remodeling will still be taking place.1-3, 8, 11
Isotretinoin should be suspended from 6 to 12 months prior dermabrasion aimed at preventing the formation of hypertrophic scars and keloid. Topical tretinoin can be used 2 weeks before (to expedite re-epithelialization) and continued postoperatively (to prevent postoperative hyperpigmentation). History of tendency hypertrophic scarring and keloids should also be discarded.1-3, 8, 11
The skin should be kept tensioned both by tumescent anesthesia injections and mechanical stretching. The area undergoing dermabrasion should be painted with gentian violet. The dermabrasion tool must be held unidirectionally and perpendicularly to the handpiece's rotation plane. The first pass should be performed at an angle of 45º from the axis of the scar, and subsequent passes must be carried out at right angles regarding the first pass' direction. The presence of diffuse and bleeding means that the papillary dermis has been reached. The presence of a yellow coloring arranged in parallel strands indicates that the superficial reticular dermis has been reached, while the presence of eroded strands indicates that the deep dermis has been reached, which must be avoided at all cost, since the result is an unacceptable scarring.1-3, 8, 11
In the postoperative, the surgical wound must be maintained in a moist environment, which helps re-epithelialization that will complete in 7 to 10 days. This can be done using wet dressings or by frequently washing and application of inert ointments. Post-inflammatory hyperpigmentation can be prevented with the prescription of retinoic acid (0.05% cream, once a day) and hydroquinone (4% cream, twice daily). Avoiding the exposure to sunlight and using sunscreen are very important measures. The erythema lasts from a few weeks to months, and can be mitigated with the use of local or systemic corticosteroids.1-3, 8, 11
POST-OPERATIVE CARE
Nutrition
Suture dehiscence and other complications are common in patients with malnutrition and can be detected based on low levels of serum albumin. Several micronutrients (vitamins A, C, B complex, zinc and other antioxidants) are essential for a proper healing and their supplementation can accelerate this process, eventually affecting the appearance of the scar. It is prudent to verify whether the patient is nutritionally prepared, in order not to experience this complication type during the healing process.3
Dressings
Wounds should be kept in a moist and hydrated environment, protected with occlusive or semi-occlusive dressings up until epithelialization is complete, which requires up to 48 hours in a sutured wound.2, 3
Pruritus can be managed with the use of antihistamines, such as fexofenadine or loratadine, with fewer effects on the CNS. Antihistamines also have antifibrotic effects on scars.2, 3
Sutures should be removed in a timely manner in order to prevent "train track"-like suture marks. For facial wounds, sutures must be removed within five days and, if necessary, adhesive tapes can be used on the borders. Patients should be instructed to use sunscreen on exposed areas of the body aimed at preventing hypertrophic scars.2, 3
Silicone
The latest guidelines for the treatment of scars advocate the use of therapy with silicone as prevention and first-line treatment for keloids and hypertrophic scars. Silicone tapes, sheets and gels are currently the noninvasive, gold standard treatment in such cases. Silicone tapes have the disadvantages of needing to be fixed and annoying some patients with the fact that they sometimes remain visible in certain body parts. The treatment should start soon after the removal of the suture, for it is more effective in the scar's dynamic immature phase and not as effective in older scars. The suggested mechanisms of action are: hydration of the tissue, increasing the scar's temperature, induction of tissular hypoxia or production of a local static field. Silicone also reduces the activity of mast cells, the levels of interleukin 1 and the production of extracellular matrix, all leading to decreased collagen synthesis. Silicone gel has also proven to be effective in the prevention of hypertrophic scars. A recent review by Cochrane quotes thirteen studies involving 559 patients concluding that there is evidence of benefits with the use of silicone tape, which prevents abnormal wound healing in high risk individuals.13, 14
The use of silicone in topical gel or sheets requires that the entire scar is covered for at least 12 hours per day - ideally for 24 hours per day, except for when the skin is being cleansed. It can be used isolatedly or as an adjuvant therapy after excisions and is effective for a treatment period of 4 to 6 months.13, 14
Massaging the scars can improve the patients' pain, pruritus and anxiety, however there is not enough evidence that can isolatedly improve scars' results.
Other treatments, such as onion extract, vitamin E and cream containing imiquimod have insufficient evidence proving their benefits or cause side effects, meaning that they are not recommended for routine use.13, 14
EMERGING TRENDS IN THE SURGICAL REEVISION OF SCARS
Autologous fat grafting
Adipose stem cells have a regenerating potential that can improve scars and the overlying tissue's quality. Studies in animals have shown improvement in the scar's coloration and texture, increased by the vascular endothelial growth factor, in addition to a reduction of fibrosis markers. 1
We would like to thank Dr. Carlos Rios, who kindly provided the photographs used in the present study.
1. Garg S, Dahiya N, Gupta S. Surgical Scar Revision. J Cutan Aesthet Surg. 2014;7(1): 3-13.
2. Robinson JK, Hanke WC, Siegel DM, Fratila A. Surgery of the Skin. Philadelphia: Elsevier; 2010.
3. Sharma M, Wakure A. Scar revision. Indian J Plast Surg. 2013;46(2): 408-18.
4. Nedelec B, Shankowsky HA, Tredget EE. Rating the resolving hypertrophic scar: Comparison of the Vancouver Scar Scale and scar volume. J Burn Care Rehabil. 2000;21(3):205-12.
5. Mustoe TA, Cooter RD, Gold MH. International Clinical Recommendations on Scar Management. Plast. Reconstr. Surg. 2002; 110(2):560-71.
6. Mandelbaum S, Di Santis EP Mandelbaum MH. Cicatrization: current concepts and auxiliary resources - Part I. An Bras Dermatol. 2003; 78(4):393-410.
7. Profyrins C, Tziotzios C, Do Vale I. Cutaneous scarring: Pathophysiology, molecular mechanisms, and scar reduction therapeutics Part I. The molecular basis of scar formation. J Am Acad Dermatol. 2012;66(1):1-10.
8. Kadunc B, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, et al. Tratado de cirurgia dermatológica, cosmiatria e laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2012.
9. Tziotzios C, Profyris C, Sterling J. Cutaneous scarring: Pathophysiology, molecular mechanisms, and scar reduction therapeutics. Part II. Strategies to reduce scar formation after dermatologic procedures J Am Acad Dermatol. 2012;66(1):13-24.
10. Barreiros H, Goulão J. Z-Plasty: useful uses in dermatologic surgery. An Bras Dermatol.2014;89(1):187-8.
11. Wheeland RG. Cutaneous Surgery - Textbook. New York: Saunders; 1994.
12. Park SS. Scar revision through W-plasty. Facial Plast Surg Clin North Am. 1998;6:157-61.
13. Zurada JM, Kriegel D, C. Davis IC Topical treatments for hypertrophic scars J Am Acad Dermatol. 2006;55(6):1024-31
14. Monstrey S, Middelkoop E, Vranckx JJ, Bassetto F, Ziegler UE, Meaume S, et al. Updated Scar Management Practical Guidelines: Non-invasive and invasive measures. J Plast Reconstr Aesthet Surg. 2014;67(8):1017-25.
This study was performedat Instituto Brasil de Tecnologias em Saúde - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}