


Thales Costa Bastos1; Natalia Cabellero Uribe1; Caroline Martins Brandão1; Mario Marques de Carvalho2
The basal cell and squamous cell carcinomas are known as non-melanoma skin cancers, having amounted to 98,420 new cases in men and 83,710 in women in Brazil in 2014. The reconstruction of surgical defects in the nose is a challenge for dermatologic surgeons regarding good functional and aesthetic results, since its structure is rigid and of little mobility. The authors introduce an interesting reconstruction method of a large nasal defect after excision of a basal cell carcinoma, using auricular cartilage graft and unipedicled advancement flap from the lower cheek.
Keywords: CARCINOMA, BASAL CELL; NOSE NEOPLASMS; NASAL SURGICAL PROCEDURES; EAR CARTILAGE; SURGICAL FLAPS
Skin cancer has worldwide distribution and is the most common neoplasia in human beings. Its three main forms and frequencies are: basal cell carcinoma (BCC) (75%), squamous cell carcinoma (15%) and melanoma (4%). The basal cell and squamous cell carcinomas are known as non-melanoma skin cancers and amounted to 98,420 new cases in men and 83,710 women in Brazil in 2014. These figures correspond to an estimated risk of 100.75 new cases per 100,000 men and 82.24 per 100,000 women. 1
BCCs are most commonly located on the face, with 70% of cases in the nose and forehead. In the nose, most are located in the distal two thirds, 2 particularly in the nasal wings (33% of cases) and in the dorsum (30%). 3
Gonzalez-Ulloa et al. observed that the face had different anatomical units, with transition lines separating them, and postulated that these units could be determined by differences in histologic characteristics, including thickness, amount of subcutaneous fat, color, texture, and presence of hair. 4 Based on these concepts, Burget and Menick divided the nose in the following aesthetic sub-units: dorsum, tip, columella, nasal wings, lateral walls and soft triangles. In the nasal tip and wings, the skin is thick and sebaceous, while in the dorsum and lateral walls the skin is thin. In addition, the skin has greater mobility in the upper two thirds. 5
The reconstruction of surgical defects generated by the excision of tumors in the nose is a challenge for dermatologic surgeons regarding good functional and aesthetic results, since its structure is rigid and has low mobility. The patient's age, size and location of the surgical defect according to the aesthetic subunits are the parameters that serve as guidelines in the choice of the best reconstruction method. Numerous techniques, such as primary synthesis, advancement flaps, transposition flaps, bilobed flaps, grafts or combination of techniques can be used. 6, 7
A 78 year-old, phototype IV female patient, born in the city of São Bernardo (in the Brazilian State of São Paulo) described the appearance of a painless and progressive lesion in the nose five years before. The patient presented arterial hypertension and dyslipidemia, denying prior history of skin cancer. Dermatological examination revealed an erythematous and translucent nodule measuring 2.2 x 1.7cm, with well-defined borders and a crust in its lower portion and arboriform telangiectasias across its surface, located on the nose, covering part of its three aesthetic subunits (left nasal wing, left nasal wall and nasal tip) (Figure 1). It was clinically diagnosed as a BCC and an incisional biopsy was performed, confirming this clinical suspicion. The tumor showed nodular and micronodular histologic subtypes.
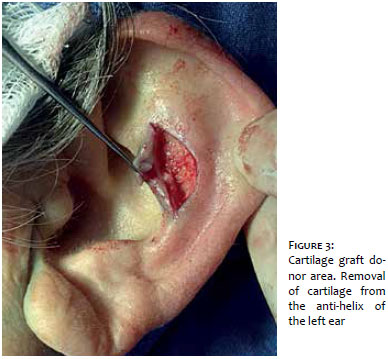
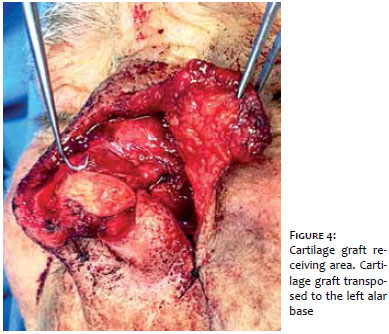
The tumor was excised with a 6.0 mm margin after tumescent anesthesia. Also, a decision was made for removing the nasal cartilage which was just beneath the tumor, due to the possibility of invasion of that structure. The surgical specimen and cartilage were sent for histological evaluation. The patient remained with a large nasal defect comprising the left nasal wing, left nasal wall, tip and dorsum (Figure 2). Initially, a cartilage graft from the anti-helix of the left ear was transposed to the left alar base aimed at supporting the rim of the nostril, preventing its upward migration during the healing of the wound, and trying to keep its contours and air passage untouched (Figures 3 and 4). Next, a unipedicled advancement flap was prepared from the cheek, with a superior base, with transfer of skin from the lower cheek towards the medial/superior direction (Figures 5 and 6). The flap was widely dissected in the subcutaneous plane, with internal sutures having been performed with 5.0 monocryl thread in order to fit it in the primary defect. Subsequently, a compensation triangle was removed from the flap aimed at rebuilding the left nasal wing, and anchoring stitches were carried out in the periosteum with 4.0 nylon thread in order to recreate the alar facial groove. Next, a small dog-ear that was formed at the superior part of the wound was corrected and the skin was sutured with 5.0 nylon thread. A compressive dressing was applied, and cephalexin and analgesic were prescribed for seven days. The patient recovered well postoperatively, with good aesthetic and functional results (Figures 7 and 8). The histology of the surgical specimen showed nodular and micronodular histologic subtypes of BCC with free lateral and deep margins. There was no evidence of tumor in the cartilage. The patient had been followed-up for a year and four months by the time the present article was approved, with no signs of recurrence.
Nasal reconstruction has seen great progress in the last 50 years. In the early days, the main objective was to provide tissular cover for the defect without significant concern about the cosmetic appearance. This concept began to change in 1950, when surgeons began to advocate the use of "similar tissue" to replace "similar tissue, according to the aesthetic units of the face.6, 7
In this manner, firstly the functional and breathing capacity of the nose should be restored, maintaining or recovering the structural integrity of the site of the defect. Secondly, an effort should be made aimed at achieving aesthetically pleasing results that are in harmony with the remaining of the face in terms of texture, color and shape. 7 Understanding of the stratigraphy of the nasal tissues is necessary for this, considering that, when analyzing the defect to be repaired, the surgeon must evaluate and determine the layers of the nose that are involved in the defect and those that are missing. In line with this, Manson et al. described the nasal reconstruction as a three-plane approach: cover (skin, subcutaneous tissue and muscles), structural framework (cartilage, nasal septum and bones) and lining (buccal skin and nasal mucosa), which should be individually assessed before the final decisions related to the repair are taken. 6, 7
The patient had a large defect in the cover - involving the nasal tip, wing, dorsum and lateral wall - and also in the structural framework, requiring an anti-helix cartilage graft in the left nasal wing base, aimed at maintaining the natural curvature (without flattening it), the respiratory function and the balance with the opposite side. The auricular cartilage provides good support, is readily available and can be harvested easily with minimal cosmetic deformity. The grafts can be harvested from the different areas of the ear (for example from the helical border, the upper or lower concha, the anti-helix and the triangular fossa), with the specific location depending on the defect's size and location, as well as the surgeon's preference. 8
Cutaneous flaps originary only from the nose are unfeasible due to the large dimensions of the surgical defect. The reconstruction options available for the authors of the present article were the interposition paramedian frontal flap, the interposition nasogenian flap with cutaneous pedicle, the full-thickness cutaneous graft and the unipedicled advancement cheek flap based superiorly. They chose the latter due to the facts that it could be performed in a single surgical time and the patient had a great volume of sagging and excess skin in the lower cheek. A single and long incision was carried out along the defect, running on the nasogenian fold up until the inferolateral cheek. After extensive dissection in the subcutaneous plane, the skin was advanced medially and superiorly towards the defect, with a small additional pivoting movement. 7, 9, 10
The dermatologic surgeon should recognize the different types of skin flaps since the incidence of nasal tumors has been increasing. In this manner, the authors present an interesting method for the reconstruction of a large nasal defect, with excellent functional and aesthetic results.
1. Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativa 2014 : incidência de câncer no Brasil. [Internet]. Rio de Janeiro: Inca; 2014. Disponível em: http://www.inca.gov.br/estimativa/2014/sintese-de-resultados-comentarios.asp
2. Batra RS, Kelley LC. Predictors of Extensive Subclinical Spread in Nonmelanoma Skin Cancer Treated With Mohs Micrographic Surgery. Arch Dermatol. 2002;138(8):1043-51.
3. Padoveze EH, Cernea SS. Reconstrução dos defeitos nasais após exérese de tumores pela cirurgia micrográfica de Mohs. Surg Cosmet Dermatol. 2013;5(2):116-120.
4. Gonzalez-Ulloa M, Castillo A, Stevens E, et al. Preliminary study of the total restoration of the facial skin. Plast Reconstr Surg. 1954;13(3):151-61.
5. Burget GC, Menick FJ. The subunit principle in nasal reconstruction. Plast Reconstr Surg.1985;76(2):239-47.
6. Bloom JD, Antunes MB, Becker DG. Anatomy, physiology and general concepts in nasal reconstruction. Facial Plast Surg Clin North Am. 2011;19(1):1-11.
7. Papadopoulos O, Kostopoulos E, Karypidis D, Tsantoulas Z, Moustaki M. Review of nasal reconstruction. J Craniofac Surg. 2009;20(4):1072-7.
8. Immerman S, White WM, Constantinides M. Cartilage grafting in nasal reconstruction. Facial Plast Surg Clin North Am. 2011;19(1):175-82.
9. Shan R. Baker. Retalhos de Avanço. In: Baker SR. Retalhos Locais em Reconstrução Facial. Rio de Janeiro: Di Livros, 2009. p.159-89.
10. Shan R. Baker. Reconstrução do nariz. In: Baker SR. Retalhos Locais em Reconstrução Facial. Rio de Janeiro: Di Livros, 2009. p. 417-77.
The present study was carried out at the Faculdade de Medicina do ABC (FMABC) - Santo André (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}