


Diogo Vieira Barroso1; Robertha Nakamura2
The term melanonychia refers to a brownish pigmentation produced by melanocytes in matrix, which extends from the proximal region up until the distal margin of the nail plate. This condition occurs due to the activation or hyperplasia of melanocytes, which presents benign lesions, such as nevi and lentigo or malignant lesions, such as melanoma of the nail unit. The intraoperative dermoscopic analysis of the nail matrix improves the diagnostic accuracy and guides on the best biopsy method for melanonychia. A proper biopsy technique is aimed at obtaining a good quality sample for the histological diagnosis - the gold standard - associated with a lower risk of permanent dystrophy.
Keywords: NAILS; LENTIGO; DERMOSCOPY
Longitudinal melanonychia is a term used to describe a brown band that runs from the proximal to the distal region of the nail plate. It occurs more frequently in non-Caucasians aged 50-70 years, with a higher incidence in the thumb, followed by the hallux and the forefinger, being observed in only 1.4% of the population.1 It can be classified according to two activation conditions: activation of melanocytes (racial melanonychia, inflammatory diseases, drugs) or melanocytic hyperplasia (benign, such as nevus and lentigo or malignant, like nail melanoma). Due to the possibility of the diagnosis of melanoma, biopsy of the melanonychia is necessary, since melanoma in the acral region has a reserved prognosis given the greater possibility of invasion. Intraoperative dermoscopy of the matrix, where the melanocytes responsible for the pigmentation of the nail plate are located, is seen as one of the main methods in the approach of these lesions. Regular lines with uniform pattern lend benignity to the lesion, while irregular lines with variation in color suggest malignancy. 2 Based on dermoscopic features, the surgeon can decide with greater certainty on the best biopsy technique to be adopted. 3 When performing a biopsy on the nail matrix, the proper technique is aimed at obtaining a good quality sample containing information necessary for histological analysis, associated with a lower risk of permanent dystrophy. There are 4 main surgical alternatives for biopsy of longitudinal melanonychia:4
1. tangential excision of the matrix (shaving of the matrix), which is aimed at obtaining a sample of the upper region of the matrix when dermoscopic characteristics suggest the presence of a benign lesion;
2. the use of a 3mm punch, indicated in cases where the lesion has less than 3mm;
3. longitudinal excision of the matrix, indicated for longitudinal melanonychia with medial location, aimed at removing the entire lesion;
4. lateral longitudinal excision, indicated when the melanonychia is located on the lateral part of the nail.
Above all, it is important to obtain a sample that contains the information necessary for the correct diagnosis of melanonychia. The authors present a case of simple nail benign lentigo, the adopted approach, clinical dermoscopic findings, the decision process regarding the surgical biopsy technique and the histologic aspect found.
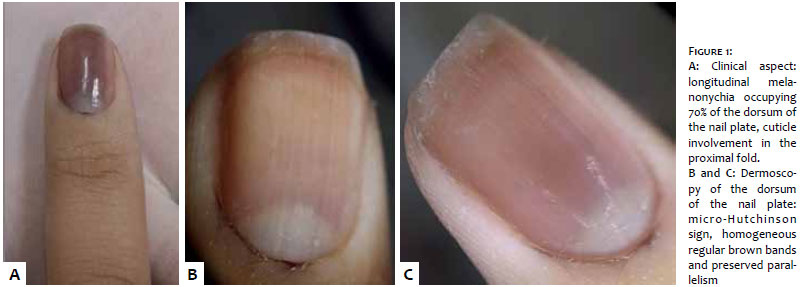
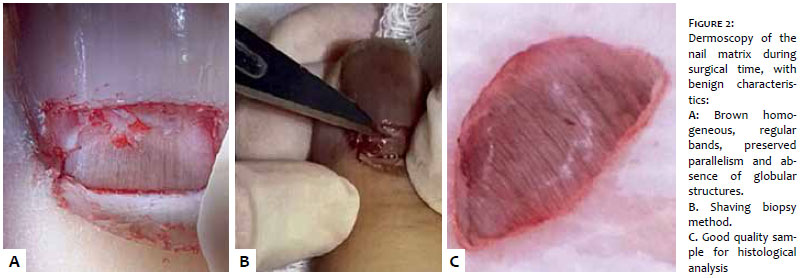
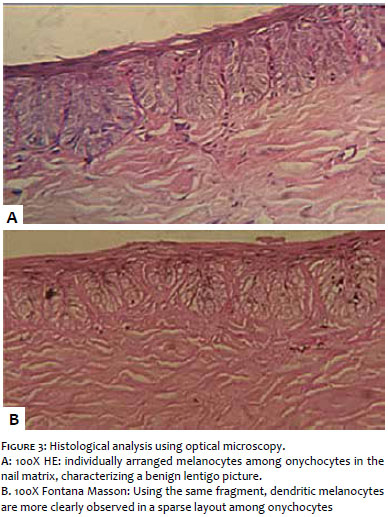
A 31 year-old female patient described the appearance of brown longitudinal, asymptomatic band, in the second left thumb two years before. She described a progressive increase in the width of the band. There was absence of history of trauma or previous use of medications. She did not made reference to family history (Figure 1A). The dermoscopy of the dorsum of the nail plate showed benign characteristics (Figures 1B and 1C). A pattern of regular brown bands, with an absence of globular structures, was observed in the intraoperative dermoscopy of the nail matrix. Due to the benign dermoscopic features, the surgical option for the biopsy was the shaving of the nail matrix. The objective was to obtain a good quality sample for the diagnosis, with the functional preservation of the nail matrix (Figure 2). Histology characterized a picture of ungual benign lentigo (Figure 3). The postoperative coursed with absence of permanent scar, such as pterygium or onychoatrophy, with the nail plate returning to its physiological growth in the 30 and 60 days follow ups (Figure 4).
In that case, the patient had indication for biopsy for it was an acquired lesion, in the index finger, with progression in width for two years. 5 The clinical and dermoscopic analysis of the nail plate is a widely used, simple to perform and cost effective method that provides a better diagnostic accuracy of longitudinal melanonychia. Using this method in the present case, it was possible to verify the melanonychia's benign pattern - regularity and parallelism of brown lines and homogeneous color. The intraoperative dermoscopy of the matrix allows direct examination of the pigmentation's origin and, according to the characteristics found, assists in the choice of the best biopsy technique to be adopted. In the present clinical case, the intraoperative analysis of the matrix, which yielded benign characteristics, pointed towards the adoption of the shaving biopsy technique. The good quality of the sample allowed the histological diagnosis of simple lentigo type melanocytic hyperplasia. The choice of biopsy technique depends on factors such as location, origin (proximal or distal matrix) and width of the melanocytic band, as well as on the presence of periungual pigmentation (Hutchinson's sign). 6_9 The tangential excision of the matrix captures a sample of less than 1mm 10 in depth with good quality length. This technique was chosen due to the location of the pigmentation (distal matrix) and the absence of malignant features. It is important to note that the shaving of the matrix is indicated for lesions with more than 3mm, especially those located in the distal matrix. One disadvantage of this method is that the precision degree of the evaluation of the dermal layer may be limited.
The present case illustrates the importance of using varied and relevant tools available for the approach of melanonychia. It is important to track cases suggestive of malignancy. The choice of the appropriate biopsy technique aims at obtaining a good quality sample for histological study, preserving the matrix's functionality, with decreased possibility of onychodystrophy.
The present case demonstrates the use of dermoscopy of the nail matrix during surgical time, assisting in the semiotic and management of melanonychia. Although the clinical and dermoscopic aspects are of great propaedeutic assistance in a great number of cases, anatomical pathological examination is crucial to confirm the diagnosis.
1. Hiroshi K, Toshiaki S, Hisashi U. Key point in dermoscopic differentiation between early nail apparatus melanoma and benign longitudinal melanonychia. J Dermatol. 2011;38(1):45-52.
2. Di Chiacchio N, Cadore de Farias D, Piraccini BM, Hirata SH, Richert B, Zaiac M, et al. Consenso sobre dermatoscopia da placa ungueal em melanoniquias. An Bras Dermatol. 2013;88(2):309-13.
3. Hirata SH, Yamada S, Enokihara MY, Di Chiacchio N, de Almeida FA, Enokihara MM, et al. Patterns of nail matrix and bed of longitudinal melanonychia by intraoperative dermatoscopy. J Am Acad Dermatol. 2011;65(2):297-303
4. Collins SC, Cordova KB, Jellinek, NJ. Midline/paramedian longitudinal matrix excision with flap reconstruction: Alternative surgical techniques for evaluation of longitudinal melanonychia. J Am Acad Dermatol. 2010;62(4):627-36.
5. Braun RP, Baran R, Le Gal FA, Dalle S, Ronger S. Diagnosis and management of nail pigmentations. J Am Acad Dermatol. 2007;56(5):835-47.
6. Baran R, Dawber RPR, De Berker DAR, Haneke E, Tosti A. Diseases of the nail and their management. 3rd ed. Oxford: Blackwell Science; 2001.
7. Baran R, Perrin C, Braun RP, Thomas L. The melanocyte system of the nails and its disorders. 2nd ed. New York: Oxford University Press; 2005.
8. Baran R, Haneke E. Diagnose und Behandlung von longitudinalen Nagel pigmentierungen. Hautarzt. 1984;35:359-65.
9. Baran R, Kechijian P. Longitudinal melanonychia (melanonychia striata): diagnosis and management. J Am Acad Dermatol. 1989;21(6):1165-7.
The present study was conducted at the Hospital Universitário Pedro Ernesto da Universidade Estadual do Rio de Janeiro (Hupe/Uerj) – Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}