


Emerson de Andrade Lima
Introdução: The beneficial role of medium peelings and microneedling in photoaging and scars yield satisfactory results. Objective: A retrospective, descriptive, single-center study evaluating the results of the association of 88% phenol and microneedling for treating sagging, wrinkles and acne scars on the face. Methods: Medical records and standardized photographs, taken before and 3 months after the procedure, of 28 patients diagnosed with wrinkles, sagging or acne scars and treated with 88% phenol peeling followed by microneedling with 2.5 mm needles, were analyzed. Events and complications were recorded 15 days after the procedure. The investigator physician performed clinical and photographic assessments 3 months after the procedure, when patient satisfaction questionnaires were also applied. Results: Twelve patients had only wrinkles and sagging, 5 had only acne scars and 10 had both pictures, with skin phototypes I to III. Erythema persisted for 30 days and post-inflammatory hyperpigmentation was observed in 7 of 28 patients. Based on the clinic and photographic evaluations, the author considered the results as good and very good. 100% of patients reported satisfaction with the outcomes. Conclusions: Good results were observed with the association of 88% phenol and microneedling. Few patients experienced adverse effects, allowing the author to suggest that the procedure showed a good safety profile.
Keywords: THERAPETICS; REJUVENATION; CICATRIX S
The beneficial role of medium peelings in photoaging and facial scars has been extensively studied. 1 Evidence of the increase in collagen fibers type I and III, and restoration of elastic fibers, followed by dermal remodeling induced by caustic agent are effects already described by some authors.2, 3 Phenol has an immediate caustic action, with the ability to promote denaturation and coagulation of epidermal keratin proteins, achieving unparalleled clinical results as compared to other ablative techniques.4 The microneedling technique, applied to the skin aimed at generating multiple micropunctures, resulting in inflammatory stimulus and collagen production, has been described as being a percutaneous induction of collagen (PIC). Firstly there is loss of integrity of the skin barrier, aimed at dissociating keratinocytes and causing the release of cytokines, resulting in dermal vasodilation and keratinocytes migration in order to restore the epidermal damage.5, 6 Fibroblasts and keratinocytes are stimulated, causing the production of type III collagen, elastin, glycosaminoglycans and proteoglycans, as well the formation of fibronectin matrix, allowing the deposit of collagen just beneath the basal layer of the epidermis.7 The reviewed literature does not contain any description of the association of these two therapies, which, isolated, induce similar responses. The objective of the present retrospective, descriptive, single-center study was to evaluate the results of the association of 88% phenol peeling and microneedling in the treatment of facial sagging, wrinkles and acne scars.
Records of 28 patients diagnosed with wrinkles, sagging or acne scars in the genian regions, treated with the combination of 88% phenol peeling followed by microneedling, according to a same protocol performed by the same physician, between January 2011 and January 2015. The study complied with the ethical recommendations of the Helsinki declaration. Patients with skin infections and prone to keloids were excluded.
The following treatment protocol was applied: monitoring of heart rate record, oxygen saturation and arterial blood pressure during the procedure; degreasing of the skin with liquid soap, antisepsis with chlorhexidine and block anesthesia of the infraorbital and mentonian nerves, followed by infiltrative anesthesia with 2% lidocaine and saline (1:3) of the genian region, observing the maximum anesthetic dose according to the patient's weight. The 88% phenol was applied with gauze until obtaining a solid frosting in the skin, being immediately followed by the microneedling procedure with a cylindrical device equipped with one hundred ninety-two (192) 2.5mm long needles arranged in eight rows, sterilized by gamma irradiation (Dr. Roller®, Mooham Enterprise Co., Gyeonggi-do, South Korea, Anvisa n. 80669600001). Back and forth movements were performed up until an uniform bloody dew emerged. The contra-lateral genian region was treated with the same technique. The procedure was completed with the application of a dressing with sterile gauze, which was removed 24h after at home, during the bath, being followed by the use of a cutaneous barrier regenerator three times a day. Fifteen days after having undergone the procedure, all patients were examined and asked to answer a questionnaire about the period following the intervention. The objective was to identify expected effects as erythema and edema, or complications such as post-inflammatory hyperpigmentation or infections. On this visit, all patients were instructed to use an industrialized depigmenting substance (0.05% retinoic acid + 4% hydroquinone + 0.01% fluocinolone acetonide), alternating it with a cutaneous regenerator for 15 days and SPF 50+ industrialized tinted sunscreen. Later on, patients were instructed to use the depigmenting substance every night, which was done with good tolerability.
The clinical evaluations (according to the categories very good, good, regular and poor) and photographic assessment (immediately before and three months after the procedure, with the same digital camera) were performed by the investigator physician three months after the procedure, when patient satisfaction questionnaires regarding the results were also applied.
The device used to perform the microneedling comprises a polyethylene cylinder studded with stainless steel sterile needles symmetrically aligned in rows, totaling 192 units. The length of the needles is constant throughout the instrument's structure. For this needle length, anesthetic blocks complemented by infiltrative anesthesia are recommended. Microneedling is a technician-dependent procedure, and familiarization with the device used and technical mastery are factors that directly influence the final result. It is recommended to position the device between the thumb and index finger, as if holding a hashi, controlling the force with the thumb. The back and forth movements must be guided by a uniform pattern of petechiae throughout the treated area, and can be mild to intense. Theoretically, a number of passes between 10 and 15 in the same region yield 250-300 punctures / cm2. The time elapsed before the emergence of the petechiae varies according to the thickness of the treated skin and the length of the selected needle. In this manner, a thinner and looser, commonly photodamaged skin will present a uniform petechiae pattern earlier than thicker skins, observed in patients with acne scars, for example. Lima et al. 8 proposed a classification relating the length of the needles of microneedling devices with the expected damage's depth, terming the severity of the inflicted injury as mild, moderate and deep. The patients evaluated in the present study underwent a deep injury degree as they were treated with 2.5mm long needles.
Among the 28 patients treated, 12 had only wrinkles and sagging, 5 had only acne scars, and 10 had wrinkles, sagging and acne scars.
The patients' skin phototypes ranged from I to III, according to the Fitzpatrick classification.
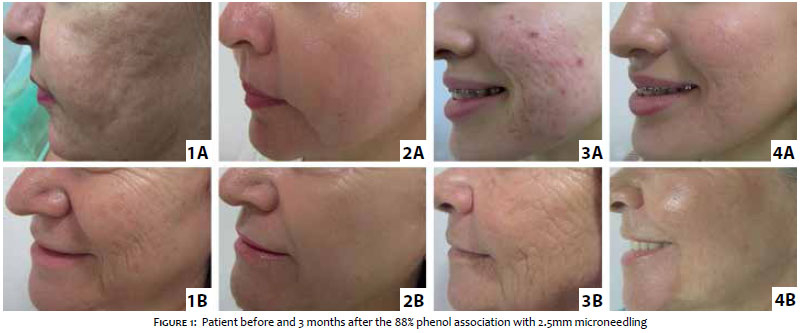
In the clinical and photographic evaluation, the author rated the results from good to very good on a scale that included the categories very good, good, regular and poor. (Figure 1)
In the patient satisfaction questionnaire, 100% of patients reported satisfaction with the results. All informed they would undergo the procedure again, if necessary.
The degree of pain and discomfort during the procedure was considered tolerable by the patients. The heart rate, oxygen saturation and arterial blood pressure records presented very little fluctuation during the intervention.
The return to professional activities occurred within seven to ten days. Moderate edema and erythema persisted during a period ranging from 25 to 35 days, having been well camouflaged by the use of tinted sunscreen. Moderate post-inflammatory hyperpigmentation was observed in 7 patients (from a total of 28 patients), having been reversed with the use of the depigmenting substance within 30 to 45 days. It was also found that all 28 patients were responsive to the technique used and would undergo the same procedure in other cases with similar indication. At the time the present article was submitted for approval, 13 of the 28 patients evaluated were already being followed-up for 24 months after the procedure, with satisfactory maintenance of the results. (Figure 1)
It is known that the penetration of needles into the epidermis and dermis, resulting in multiple punctures, triggers the stimulus for the activation of fibroblasts and keratinocytes and consequent release of growth factors, collagen proliferation and renewal of the perforated epidermis, 9, 10 while the effects of medium peelings, particularly those of the 88% phenol, were already well ratified by the literature.1_4 In the present retrospective review of 28 patients, it can be assumed that both techniques would isolatedly yield good results in the studied cases. Nevertheless, the objective of the present study is to present new therapeutic approach that is based on the simultaneous use of these two procedures. Despite being a retrospective investigation, the results allow to present some conclusions:
1. The international literature attests that microneedling with 2.5mm long needles as an isolated technique is able to produce improvement in the quality of the skin, reduction of wrinkles and correction of depressed acne scars.
2. In the author's experience, the recovery time of microneedling as an isolated technique is shorter than that when 88% phenol is associated.
3. Few patients experienced adverse effects; the post-inflammatory hyperpigmentation was reversed in a short time, allowing the author to suggest that the procedure showed a good safety profile in the group assessed.
4. When the author compares his experience with the cases evaluated in the present study with those previously treated only with microneedling, he notices a substantial further improvement in the results of the first, which prompts him to conclude that the addition of 88% phenol before microneedling potentiates the results.
5. Based on the experience presented, the author recommends the association of 88% phenol before surgical microneedling with 2.5mm long needles in the treatment of depressed acne scars, sagging and rhytids as an additional approach in the already existing broad therapeutic armamentarium.
Further studies are needed aimed at assessing a greater number of patients, and checking for the incidence of adverse effects, with a view to obtaining more accurate conclusions about the safety profile of the intervention, as well as evaluating the addition of the results of this association.
1. Bagatin E, Hassun K, Talarico S. Revisão sistemática sobre peelings. Surg Cosmet Dermatol. 2009;1(1):37-46.
2. Nelson BR, Fader DJ, Gillard M, Majmudar G, Johnson TM. Pilot histologicand ultrastructural study of the effects of medium-depth chemical facial peels on dermal collagen in patients with actinically damaged skin. J Am Acad Dermatol. 1995;32(3): 472-8.
3. Fulton JE, Porumb S. Chemical peels - Their place within the range of resurfacing techniques . Am J Clin Dermatol. 2004;5(3):179-87.
4. Kadunc BV, Vanti AA. Avaliação da toxicidade sistêmica do fenol em peelings faciais. Surg Cosmet Dermatol. 2009;1(1):10-4.
5. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2006;17(1):51-63.
6. Bal SM, Caussian J, Pavel S, Bouwstra J A. In vivo assessment of safety of microneedle arrays in human skin. Eur J of Pharm Sci. 2008;35(3):193-202.
7. Lima E, Lima M, Takano D. Microagulhamento: estudo experimental e classificação da injúria provocada. Surg Cosmet Dermatol. 2013;5(2):110-4.
8. Vasconcelos NB, Figueira GM, Fonseca JCM. Estudo comparativo de hemifaces entre 2 peelings de fenol (fórmulas de BakerGordon e de Hetter), para a correção de rítides faciais. Surg Cosmet Dermatol 2013;5(1):40-4.
9. Lv YG, Liu J, Gao YH. Xu B. Modeling of transdermal drug delivery with a microneedle array. J Micromech Microengim. 2006;16(11):151-4.
10. Vandervoort L, Ludwig A. Microneedles for transdermal drug delivery;- minireview. Frontiers in Biocience. 2008;13(5)1711-5.
The present study was carried out at Santa Casa de Misericórdia do Recife - Recife (PE), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}