


Daniel Dal'Asta Coimbra1; Betina Stefanello de Oliveira2; Natalia Caballero Uribe3
Introdução: Nasal filling can be used as an alternative to traditional rhinoplasty aiming at correcting small nasal defects and for complementation or correction after surgical procedures. Objective: To describe the profile of patients who underwent nasal filling and demonstrate the efficacy and safety of a new hyaluronic acid based filling substance. Methods: Retrospective analysis with statistical study of nasal filling procedures conducted in 280 patients. Results: The sample was composed mostly of Caucasian women with a mean age of 43 years. The nasal regions more commonly treated with the filler were the nasal root, tip and septum. Patients showed significant improvement and expressed satisfaction with the results. 17.1% of the patients were re-treated, and 7.2% had easy to resolve complications. Conclusion: The results were long lasting and natural, especially those related to thinning of the nasal tip.
Keywords: NOSE; HYALURONIC ACID; ESTHETICS
Due to the importance of personal appearance, aesthetic corrections of the nose have been of interest since ancient times. In the Middle Ages, Gaspare Tagliacozzi introduced the famous "Italian method" for the reconstruction of nasal traumas and deformities. During the 20th century, various rhinoplasty surgical techniques were created. 1 However, Broeckaert, who is considered the father of modern rhinoplasty - was the first to perform nasal corrections using liquid paraffin as cutaneous filler in the early twentieth century. Doctors favorable to minimally invasive procedures developed techniques and safer materials for correction of nasal defects henceforth. 2
Although being considered the gold standard, the surgical approach of nasal defects is an invasive procedure that often requires the fracture of the nasal bone. Cutaneous fillers arise as an alternative for the correction of small nasal defects and complementation or post-surgical correction.2, 3 Although not definitive, they have gained ground since they are less traumatic and painful, and have minimal complications as compared to the traditional rhinoplasty.4, 5
The search for materials that are safe and long lasting, and have predictable effects is continuous. Hyaluronic acid (HA) based cutaneous fillers are currently the most used due to their ease of application, predictable efficacy, good safety profile and speedy patient recovery.6, 7
In face of the need for further studies on new cutaneous filling substances, the present article aims at profiling patients and demonstrating the effectiveness and safety of a new HA based filler.
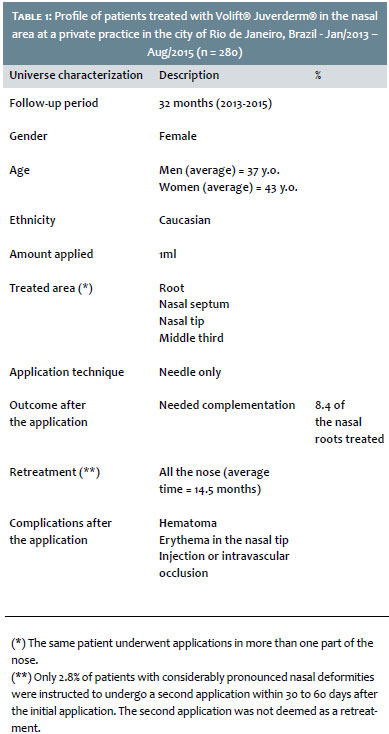
A retrospective and single-center study was carried out with 280 patients who underwent nasal filling with Juvederm Volift® (Allergan Inc., USA) between October 2012 and May 2015 at a private practice located in the city of Rio de Janeiro, Brazil. All study patients were subjected to standardized photographs and followed up with specific data collection forms.
The sociodemographic variables included were gender, age, ethnicity, amount of product applied, treated area, application method, retreatment and complications. The study followed the ethical guidelines established by the Declaration of Helsinki.
The filling substance
Hyaluronic acid is a polysaccharide (glycosaminoglycan composed of alternating and repeating units of D-glucuronic acid and N-acetyl-D-glucosamine) with hydrophilic properties, which causes an increase of the injected tissue. 8-12 The initial filling effect is directly related to the volume of injected filling substance. Nevertheless, studies have shown that there is an indirect effect when the dermis is injected due to the activation of fibroblasts. Hyaluronic acid fillers generally last from 6 to 24 months after injection.13, 14 When an appropriate volume is placed in the correct plane, the filling material can not be perceived visually or by palpation.
The vycross® technology (Allergan Inc., USA), incorporates short to long chains of HA, which generates more efficient crosslinking than that of previously used HA fillers. The inclusion of short HA chains allows attaching HA to the ends of the molecules, resulting in a product with longer durability than that of the fillers that include only long chains of HA. Furthermore, this technology provides higher viscosity to the gel, resulting in an increased lift capacity against the pressure of the skin.
Its elastic modulus (G') is smaller than those the other fillers, providing a more fluid and soft gel that is easier to extrude from the syringe, resulting in a product with better spreadability during injection.
Due to the optimization of crosslinking, products with the vycross® technology may have greater durability in the tissue using at lower HA concentrations in its formula. This lower concentration of HA makes the gel less hydrophilic, which lends more safety and predictability to the results, causing a natural appearance. 15 The filling of the nasal deformities of the studied patients was performed with Juvederm® Volift® Allergan Inc., USA (17.5mg/ml of HA).
After asepsis and antisepsis with alcohol chlorhexidine, the needle was introduced directly into the region to be treated, and the product was deposited anterogradely. In most cases topical anesthesia was not used, and only 2% lidocaine with vasoconstrictor was injected at the entry puncture in cases treated with microcannulae.
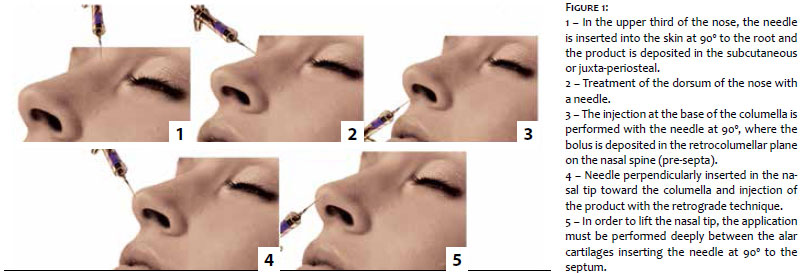
The amount of HA used in each region varied according to the specificities of the case and application plan. Thus, the following quantities are merely mean parameters: in the upper third of the nose, the needle was inserted into the skin at 90º to the nasal root and the product was deposited in the subcutaneous or juxta-periosteal (Figure 1). The amount used ranged from 0.05 to 0.25 ml of HA in one or more punctures.
In the middle third of the nose, fillers were not in general applied for volumizing the area, but only small amounts (0.05 and 0.15ml) were injected aiming at improving the quality of or for "rounding" the skin at the site. In Asian patients or in those with unsightly concavities resulted from surgical procedures in the nose to improve the projection along the nasal dorsum, larger quantities of product were used (0.1ml to 0.4ml).
Injections at the base of the columella were performed with the needle at 90º, depositing from 0.1ml to 0.3ml of HA in a single bolus injection in the retrocolumellar plane, on the nasal spine (preseptal). The application in the cartilaginous septum was performed through the same inferior orifice, however with the needle angled at 45º toward the nasal tip and with a deposition of 0.1ml to 0.2ml in retroinjection, from the upper portion up until the base of the septum.
In some patients, access to the nasal septum was also obtained superiorly with the needle inserted perpendicularly in the nasal tip toward the columella, with retrograde deposition of the product. The elevation of the nasal tip was also obtained with the deposition of HA in this area, between the alar cartilages. The application was deep, with the needle inserted at 90º degrees regarding the septum. The elevation occurred immediately when the filler was deposited (from 0.1ml to 0.3ml) on the structures that form the nasal septum. Superficial applications were not performed in this region due to the risk of necrosis of the nasal tip by vascular obstruction.
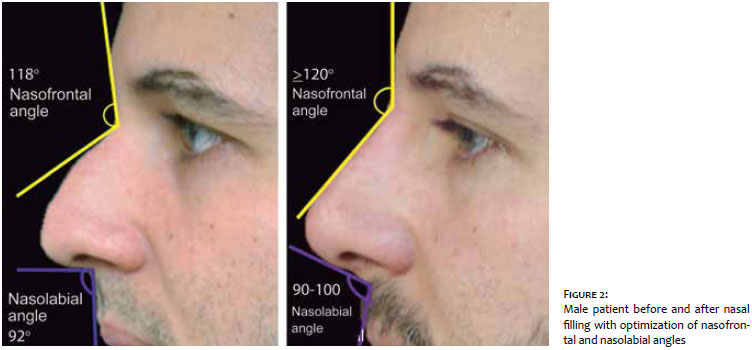
An aesthetic result was deemed satisfactory when the nasolabial angle measurement was gauged at between 90º and 100º for men (Figure 2), and 95º and 110º for women (Figure 3).
When microcannulas were used, a single entry orifice was made in the nasal tip or in the glabellar region, with the deposition of the product being carried out with the retrograde technique. The nasal septum was reached downwardly through the orifice in the nasal tip. Microcannulas with 22G to 25G were used, with lengths varying from 4cm to 7cm. The cannulas were used to improve the projection of the middle third of the nose. In the treatment of the nasal lateral extensions, 27G microcannulas were used in some instances, due to the thinner skin.
Statistical analysis
The data collected with the specially developed forms allowed to carry out the descriptive statistics analysis.
Ten variables were selected for this analysis: i) gender, ii) age, iii) ethnicity, iv) amount of product applied, v) treated area vi) application method (cannulas, needles or both), vii) outcome after the application (aimed at assisting in the decision of whether or not to apply the product to completion), viii) retreatment, ix) complications (presence and type), and x) photographic results in 30 and 60 days after.
Results
One hundred and eighty female (64.3%) and 100 male patients (35.7%) were studied. Their ages ranged from 15 to 88 years (women's mean age = 43 years, men's mean age = 37 years). Of the treated patients, 248 were of Caucasian origin (88.5%), 20 were negroids (7.1%) and 12 were Asian (4.2%). (Table 1)
The application techniques and amounts of filler used in each region of the nose followed those described above, ranging from 0.3ml to 1.0ml of the product in total per application. One milliliter per treatment (session) was used in 90% of cases.
The treatment was performed in the superior third of the nose (root) in 260 cases (92.9%), in the middle third of the nose in 80 cases (28.6%), in the nasal tip in 230 cases (82.1%), and in the nasal septum in 255 cases (91.1%).
Only needles were used for application in 235 cases (83.9%), only microcannulas were used in 20 cases (7.1%), and a combination of the two methods was used in 25 patients (8.9%).
Between 30 and 60 days after the treatment, 22 patients (8.4% of the 260 patients treated in this region) required complementation in the nasal root, which ranged from 0.1ml to 0.2ml of the product. No complementation was performed in other previously treated regions of the nose.
Eight patients (2.8%) with very pronounced nasal deformities underwent a second application, which took pace after 30 to 60 days of the first application. In these cases, the total dose HA dose was 2.0ml in the two applications.
Since the authors started to use this filling material for the correction of nasal defects in their practice, 48 patients (17.1%) have returned for reapplication of the product. The eight patients who underwent the initial treatment in two stages are not included in this statistic. The minimum time elapsed between the two applications was nine months, and the maximum, 24 months. The average interval relating to all patients who underwent reapplications was 14.5 months. The amount of product used in in retreatments varied from 0.3ml to 1.0ml and, in general, a lesser amount was necessary as compared to the initial application. Only 60% of these patients used 1.0ml in the reapplication.
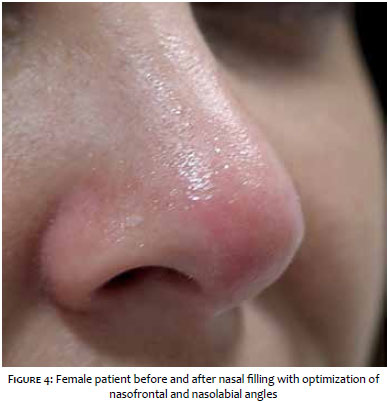
Even using needles for application in almost all cases, only eight patients (2.9%) described visible hematoma. All who underwent the application reported pain to the touch and edema in the application site, in special those treated in the nasal tip and columella. These occurrences, however, receded within 2 to 14 days after the treatment. Twelve patients (4.3%) reported important post-procedure erythema in the nasal tip that in general decreased within up to four weeks - only in one patient (Figure 4) it persisted for longer, having receded after four monthly sessions of intense pulsed light (IPL). There were no complications related to the injection or intravascular occlusion.
All patients had evident improvement in the nasal contour and deformities in the photographic assessment performed immediately after the procedure and in the 30 and 60-day follow-ups after the procedure. There was no report of unaesthetic increase or enlargement of the nasal tip in follow-up visits.
The nasal cutaneous filling procedure is indicated for the correction of the contour and deformities of the nose, constituting an alternative to plastic surgery or a post-surgical complementation. Despite not being definitive, it brings quick and safe good aesthetic results, provided that the applicator physician has mastery of the anatomy of the region to be treated and of application techniques.
Hyaluronic acid based fillers started to be applied in the nasal region eight years ago, with the use of biphasic and monophasic products, different technologies, good aesthetic results and duration ranging from 6 to 12 months. In turn, the product analyzed in the present study started to be used in the nasal region, with the already described application techniques 32 months ago. Unlike the results outcomes obtained with the previously used products, the new product leads to a greater thinning of the nasal tip, which was observed within 3 and 4 weeks after the application.16 This effect was reported by most of the patients treated and also observed by the applicator physician.
Despite the fact that Webster et al. have developed a study on nasal filling with injectable silicone in 347 patients in 1986, 17 it was not possible to found in the literature the description of such a large sample using HA.
The fact that the majority of patients were females can be explained by the interest for aesthetic procedures, which is more frequent among women than among men. Other studies also show a predominance of female patients in the search for that kind of procedures. 17, 18
The predominance of Caucasians among the treated patients can be explained by the greater purchasing power of this population in Brazil. The fact that most of the sample consisted of Caucasians may also explain the lower number of applications in the middle third of the nose, since this population in general already has a projected nasal dorsum. 12
The amount of product used and the parts of the nose that were filled are in line with the literature, despite the fact that the latter have not been conducted with the same product. The reports found in the literature often mention permanent fillers, such as silicone, 17 or semipermanent fillers, such as calcium hydroxyapatite. 19-21
The amount used in the nasal root varied from 0.05 to 0.25 ml of HA in one or more punctures. An angle greater than 120º is desirable, however excessive deposition of product in this area should be avoided, as this could lead to the widening of the nasal root, and the consequent increase in the distance between the eyes.18, 22
Application in the lateral extensions of the nose can be performed to improve asymmetries or widen the middle third of the nose (0.05 to 0.2 ml). 18, 22
The most significant changes caused by the use of fillers in the nose are obtained with the treatment of the lower third of the nose, resulting in the alteration of the position and format of the nasal tip. To lift the nasal tip and consequently increase the nasolabial angle, one or more of the following regions can be treated: the columellar base, nasal septum or nasal tip (between alar cartilages). 18, 22
As the study product has lidocaine in its formulation, despite the fact that no topical or injectable anesthetic was used in the applications with needle (anterograde injection), the pain during the procedure is quite tolerable, being described with lower intensity as compared to that verified when using the same product in the nasolabial fold.
Despite the immediate improvement of the nasal contour and angles with the use of HA, it is worth to note edema will occur immediately after the procedure and remain in place for a few days. The final result is obtained in about four weeks, when the need for supplementation will be assessed. Unlike the results obtained in the treatment of the middle and lower thirds of the nose, 8.4% of the treated patients needed complementation in the upper third. The authors believe that this is due to the greater mobility of the skin in that region, making it more susceptible to local edema immediately after the procedure, with the occurrence of small decrease in volume in the following weeks. Moreover, the product's lower volumerization capacity regarding other fillers with higher elasticity moduli may also have contributed to this increased need for reapplication in that location. 14
In general, the results in the middle and lower thirds of the nose remain after the initial procedure. Eight patients with more pronounced nasal deformities were instructed to undergo the treatment in two sessions, entailing that a two-stage treatment was used, which present a lower risk of complications, such as vascular compressions, for example. Furthermore, as the nose is a structure with low mobility, there is a limit on the amount of filler being applied in each session, a threshold beyond which there will be reflux of the product via the entry orifice. 14
The duration of the results varies among patients and is mainly related to the amount of product used, the severity of the nasal deformity and the treated nasal region. 23, 24 In general, results persist for over a year and in some patients have remained almost unchanged after 18 months of application, which suggests the possibility of an even greater permanence. The authors of the present article did not find similar results for the use of HA in the literature. 25-28
After the assessment of the initial result, 48 patients returned for retreatment 14.5 months (on average) after the first application. It is not possible to state that this would be the average product life in nasal treatments, for patients with longer durations might still have not returned for retreatment, and some other patients might not return for considering that the outcome or duration differed from the expected.
There was a small number of complications linked to the procedure and none of them resulted in permanent problem for patients. Anatomical knowledge and experience in the treatment of this region with fillers can be the main factor related to the low rate of adverse effects found in the present case series.14, 29, 30
The authors of the present article did not find in the literature a study with a significant sample and/or a follow-up period longer than two years, involving the use of the analyzed product in any site of the face. 31
Therefore, the present study is a contribution from the Brazilian dermatology to other countries that may use the product and may serve as the basis for future studies.
Conclusion
The use of HA based fillers in the nose is an increasingly common procedure in the medical practice that leads to good aesthetic results when well indicated. The authors described their experience with the use of a new product in the treatment of this body site, with long lasting and even more natural outcomes, mainly related to the thinning of the nasal tip. In general, nasal fillers are safe and effective and are a consistent alternative to rhinoplasty due to their few adverse events and considerable patient satisfaction. Further research with HA is needed for comparison and reproduction of results.
Acknowledgements
The authors of the present article would like to thank the biostatistician Dr. Luiz Felipe Pinto for his contributing with the data review and statistical analysis.
1. Burke AJ, Cook TA. Open versus Closed rhinoplasty: What have we learned? Curr Opin Otolaryngol Head Neck Surg. 2000;8(4):332-6.
2. Radaelli A. Medical rhinoplasty with hyaluronic acid and botulinum toxin A: A very simple and quite effective technique. J Cosmet Dermatol. 2008;7(3):210-20.
3. Coleman SR, Saboeiro A, Sengelmann R. Comparison of lipoatrophy and aging: volume deficits in the face. Aesthet Plast Surg. 2009 33(1):14-21.
4. Maio M. The Minimal Approach: An innovation in facial cosmetic procedures. Aesth Plast Surg. 2004;28(5):295-300.
5. Tzikas TL. A 52-month summary of results using calcium hydroxylapatite for facial soft tissue augmentation. Dermatol Surg. 2008;34(Suppl 1):S9-S15.
6. Carruthers J, Cohen SR, Joseph JH, Narins RS, Rubin M. the science and art of dermal fillers for soft-tissue augmentation. J Drugs Dermatol. 2009;8(4):335-50.
7. Humphrey CD, Arkins JP, Dayan SH. Soft tissue fillers in the nose. Aesthet Surg J. 2009;29(6):477-484.
8. Russell WH, Soliemanzadeh P. Nasal tip management utilizing the open approach, rhinology and facial plastic surgery. New York:, Springer-Verlag Berlin Heidelberg; 2009. p. 723-45.
9. Rohrich RJ, Bang H, Muzaffar AR, Adams WP,Robinson JB, importance of the depressor septi nasi muscle in rhinoplasty: anatomic study an clinical application, plastic and reconstructive surgery, 2000:377-387.
10. Randolph B. Capone and Ira D. Papel Capitulo 67 Septorhinoplasty: Management of the Nasal Vault and Septum: Springer-Verlag Berlin Heidelberg 2009 677-687
11. Dingman RO, Natvig P (1977) The deviated nose. Clin Plast Surg 4:145-152
12. Vuyk HD (2000) A review of practical guidelines for correction of the deviated, asymmetric nose. Rhinology 38(2):72-78
13. Radaelli A, Limardo P. "Minimally invasive procedures for nasal aesthetics" J Cutan Aesthet Surg 2012;5(2):115-120.
14. Rokhsar C, Ciocon DH. Nonsurgical rhinoplasty: an evaluation of injectable calcium hydroxylapatite filler for nasal contouring. Dermatol Surg. 2008;34(7):944-46.
15. Meneghini P, Biondi P. Chapter: Nasal analysis; clinical facial analysis. New York: Springer-Verlag Berlin Heidelberg: 2012. p. 73-106.
16. de Lacerda BA, Zancanaro P. Filler rhinoplasty. Der-matol Surg 2007;33(Suppl 2):S207-12.
17. Webster RC, Hamdan US, Gaunt JM, Fuleihan NS, Smith RC. Rhinoplastic revisions with injectable silicone. Arch Otolar- yngol Head Neck Surg.1986;112(3):269-76.
18. Villarejo Kede MP, Sabatovich O. Ácido Hialurônico: Preenchimento de contorno nasal. 3ª ed. Rio de Janeiro: Atheneus, 2015.
19. Kim P, Ahn JT. Structured nonsurgical Asian rhino- plasty. Aesthetic Plast Surg.2012;36(3):698-703.
20. Rivkin A, Soliemanzadeh P. Nonsurgical rhinoplasty with calcium hydroxylapatite (Radiesse!). Cosmet Dermatol. 2009;12:619-24.
21. Becker H. Nasal augmentation with calcium hydrox ylapatite in a carrier-based gel. Plast Reconstr Surg. 2008;121(6):2142-7.
22. Monreal J. Fat grafting to the nose: personal experience with 36 patients. Aesthetic Plast Surg 2011;35(5):916-22.
23. Cassuto D. The use of dermicol-P35 dermal filler for nonsurgical rhinoplasty. Aesthet Surg J. 2009;29(3 Suppl):522-4.
24. Siclovan HR, Jomah JA. Injectable calcium hydrox- ylapatite for correction of nasal bridge deformities. Aesthetic Plast Surg. 2009;33(4):544-8.
25. Han SK, Shin SH, Kang HJ, Kim WK. Augmentation rhinoplasty using injectable tissue-engineered soft tissue. Ann Plast Surg.2006;56(3):251-5.
26. Beer KR. Nasal reconstruction using 20mg/mL cross-linked hyaluronic acid. J Drugs Dermatol. 2006;5(5):465-6.
27. Bray D, Hopkins C, Roberts DN. Injection rhino- plasty: non-surgical nasal augmentation and correc- tion of post-rhinoplasty contour asymmetries with hyaluronic acid: how we do it. Clin Otolaryngol. 2010;35(3):220-37.
28. Dayan SH, Kempiners JJ. Treatment of the lower third of the nose and dynamic nasal tip ptosis with Botox. Plast Reconstr Surg. 2005;115(6):1784-5.
29. Salasche S, Bernstein G, Senkarik M. Surgical anatomy of the skin. New York: Appleton & Lange; 1988. 200-15.
30. Tamura BM. "Anatomia da face aplicada aos preenchedores e à toxina botulínica - Parte II". Surg Cosmet Dermatol. 2010;2(3):205-14.
31. Jasin ME. Nonsurgical Rhinoplasty Using Dermal Fillers. Facial Plast Surg Clin N Am. 2013;21(2):241-252.
The present study was conducted at a private practice in Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}