


Rogerio Nabor Kondo1; Rubens Pontello Junior2
The malar region is the site of skin tumors and sometimes a primary closure is not possible after the excision of the lesion. The A-T flap is a good method for reconstructing an broad and deep defect in which the local surrounding tissue does not allow direct closure. The present study describes the implementation of an A-T flap as an option for the reconstruction of an operative wound secondary to the excision of a basal cell carcinoma.
Keywords: SURGICAL FLAPS; ZYGOMA; CARCINOMA, BASAL CELL
Skin cancers are most often found in the face - an anatomical area of great aesthetic importance to patients. As a consequence, promoting tumor cure while preserving the function and local appearance can be a great challenge for dermatological surgeons, especially when there is need for the preparation of a flap. 1
The present paper describes the application of an A-T flap as an option for resolving a wound secondary to the exeresis of a basal cell carcinoma (BCC) in the malar region.
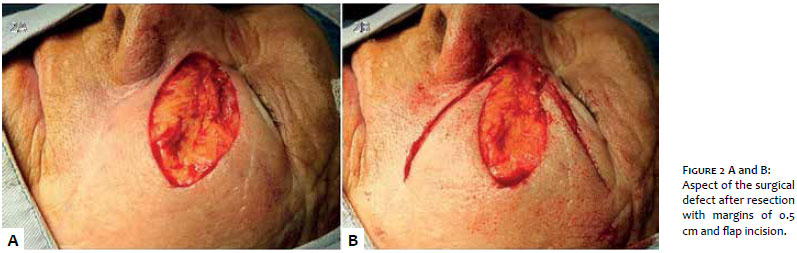
A sixty-seven year old Caucasian female patient presented an infiltrating plaque in the left malar region, with prior biopsy compatible with BCC. Five millimeters margins marking and retail design were carried out (Figure 1). The primary closure of the surgical defect resulting from the excision of the tumor was not possible (Figures 2). The A-T flap was sutured in place with 5.0 mononylon thread (Figure 3). Six months after the patient shows no sign of recurrences of BCC with good aesthetic and functional conditions (Figure 4).
Cutaneous flaps are resources that can be necessary for the closure of skin tumors excisions in the face.1-4 In the malar region, the reconstruction of resulting large wounds can be a real challenge for dermatologic surgeons, given that the local function and aesthetics must be preserved. 2-4
The advancement and rotation flap that uses the nasolabial fold and inferior orbital rim has been described for the closure of cutaneous defects in the malar region. 2, 3 In the present case, the authors have chosen the A-T flap, in which the lesion would correspond to the "A", and the intersection of the lower orbital rim, nasofacial and nasogenian folds corresponds to the horizontal segment of the "T" (Figures 1, 2 and 3). The scar resulting from the horizontal segment of the "T" is naturally "hidden" in the pre-existing grooves (infraorbital, nasofacial and nasogenian rim folds), while the "A" scar (vertical segment of the "T"), is hidden in the bisector of the infraorbital and the nasogenian folds).
In accordance with its main movement towards the area of the defect, the A-T flap is classified as a bilateral advancement flap. 2, 5 It is an excellent method for resolving a wide and deep defect in which the adjacent tissue does not allow direct closure. It has the advantages of being performed with local anesthetic and allowing resolution in a single operative time. Satisfactory results depend on the technique used and of the training to perform it, in addition to the patient's health conditions and postoperative period. 5
In the present case, the primary closure of the resulting lesion would not be possible. A decision was made for a flap rather than a graft, aiming at obtaining the best aesthetic result. The patient did not present dehiscence of sutures, with good integration of the flap and the receiving area, and absence of secondary ectropion. Six months after the procedure it was possible to observe a good aesthetic and functional result, and absence of evidence of tumor recurrence (Figure 4).
Performing an A-T flap can be a good option for the resolution of large defects secondary to the exeresis of cutaneous tumors in the malar region.
1. Hassan MI, Hassan DAE. Reconstruction after removal of basal cell carcinoma. J Am Sci. 2012;8(7):42-9.
2. Baker SR. Advancement flaps. In: Baker SR, editor. Local flaps in facial reconstruction. 2th ed. Philadelphia: Mosby- Elservier; 2007.p.415-74.
3. Galimberti G, Ferrario D, Casabona GR, Molinari L. Utilidade de retalho de avanço e rotação para fechamento de defeitos cutâneos na região malar. Surg Cosmetic Dermatol.2013;5(1):76-9.
4. Camacho-Martinez FM, Rollon A, Salazar C, Rodriguez-Rey EM, Moreno D. Free flaps in Surgical Dermatology. Comparison between fasciocutaneous and myocutaneous free flaps in facial reconstructions. An Bras Dermatol. 2011;86(6):1145-50.
5. Pontello Junior R, Kondo RN, Pontello R. A utilização de retalho A-T para reconstrução de ferida operatória no dorso da mão. Surg Cosmetic Dermatol. 2013;5(3):270-2.
The present study was conducted by the Dermatology Service team, Hospital Universitário Regional do Norte do Paraná da Universidade Estadual de Londrina - Londrina (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}