


Ada Regina Trindade de Almeida1,2; Ana Flávia Nogueira Saliba1
Hyaluronic acid (HA) based cutaneous filling substances have become the treatment of choice for facial volumization. Hyaluronidase is a soluble protein that promotes the enzymatic degradation of HA. Commercially available preparations differ according to the substance's origin (bovine, ovine or human recombinant). Although cosmetic use has not yet been approved by the FDA, off-label use in dermatology is increasingly common. The purpose of the present article is to review the medical literature and prescribing information (package inserts) over existing commercially available products in order to provide an up-to-date view of the indications, dosage, injection techniques, and adverse effects.
Keywords: HYALURONIC ACID; HYALURONOGLUCOSAMINIDASE; ESTHETICS; OFF-LABEL USE
Hyaluronic acid (HA) is a glycosaminoglycan with high molecular weight that is the main component of the extracellular matrix, influencing its permeability. It is composed of D-glucuronic acid and N-acetyl-D-glucosamine, alternately linked by β bonds. 1-6
With aging, there is a resorption of fat, bones, and a reduction of HA in the skin, resulting in the loss of facial volume and the appearance of wrinkles and rhytids. Currently, HA based filling procedures have became the treatment of choice for increasing facial tissue due to several factors: there are several types available, its effect is immediate, in well-trained hands the result yields a natural appearance, it can be reproduced and, additionally, it can also be reversible when required. 7
Hyaluronidase is a soluble protein responsible for the enzymatic degradation of glycosaminoglycans. 1-6 This enzyme hydrolyses hyaluronic acid, rupturing the β bonds 4 between the residues N-acetyl-D-glucosamine and D-glucuronic acid, generating an increase in the permeability of the skin and connective tissue. 4, 8 This substance is widely found in nature and is involved in several pathophysiological conditions, such as the diffusion of toxins/poisons, fertilization, metastasis, microbial infections, and wound healing. 1-3 Six hyaluronidase-encoding genes were recognized in the human genome (Hyal-1, Hyal 2, Hyal-3, Hyal-4 and PH-20/Spam 1). 9
The serum half-life of hyaluronidase is 2.1 ± 0.2 minutes, being inactivated in the liver and kidneys. 4 Subcutaneous administration of hyaluronidase has immediate action, with a variable duration of between 24 and 48 hours. The reconstruction of the dermal barrier, after having been altered by intradermal injection of hyaluronidase, is fully completed after 48 hours. 3, 8, 10, 11
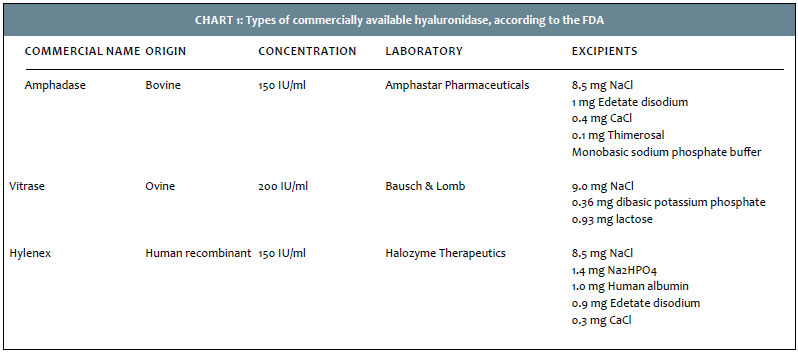
This enzyme has been legally marketed in the U.S. since 1948. 2 Commercial presentations of the injectable form of hyaluronidase are classified according to their origin. Those of bovine testicular origin are: Wydase® (Wyeth Ayerst Pharmaceuticals), Hydase® (PrimaPharmInc - 150 IU/ml), Amphadase® (Amphastar Pharmaceuticals - 150 IU/ml) and Hyalozima® (Apsen - 400 IU / ml).10-13 Wydase® and Hydase® are no longer manufactured due to their high immunogenic power, 2 and Hyalozima®, which was available in Brazil, however was withdrawn from the market in September 2013.
Vitrase® (ISTA Pharmaceuticals - 200 IU/ml) is a purified form, originated from sheep testicles. Hyalase® (Sanofi Aventis - 1.500 IU/ml), available in Australia, is also of ovine origin. 14 Hylenex® (Halozyme Therapeutics - 150 IU / ml) is the human recombinant hyaluronidase produced from hamsters' ovary cells, containing human albumin, and is the most expensive product 3-5, 10, 11, 13 (Chart 1 and Figure 1).
The FDA (U.S. Food and Drug Administration) only approves the use of hyaluronidase in three situations. 3-5 The first is the use of the enzyme to facilitate the absorption and dispersion of other injected drugs, such as when commonly used in anesthetic retrobulbar block in ophthalmic surgery.
Another indication is as an adjuvant in subcutaneous infusion of fluids, a technique used in the 1940s and 1950s in cases of dehydration. The third indication is as an adjuvant in subcutaneous urography, facilitating the absorption of radiopaque agent. In dermatology, hyaluronidase is used in an off-label manner. It is used in some procedures, such as in hair transplant anesthesia and tumescent liposuction, 15 as well as in the treatment of some conditions, for instance, pretibial myxedema, scleroderma, lymphedema and keloids. 3
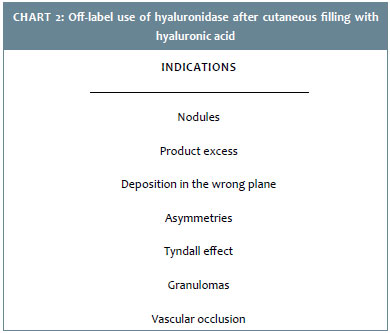
Due to the increasing number of cutaneous filling substances containing hyaluronic acid, this enzyme has gained renewed prominence. 3, 5 Hyaluronidase is commonly used in cases of excess cutaneous filling (overcorrection) and/or when the deposition is carried out on the wrong plane of the skin, resulting in nodules, asymmetries or Tyndall effect. 3, 5, 16
In the literature there are some reports of the use of hyaluronidase as a therapeutic option for rare adverse reactions resulting from cutaneous filling with HA, such as granulomas and vascular occlusions 3, 5, 8, 16-18 (Chart 2).
All these indications will be discussed in the following sections.
Excessive amount of the product
In 2004, Soparkar et al. published the first study on the use of hyaluronidase in the correction of nodules resulting from filling procedures (Restylane®) performed in periocular rhytids. They used 2.5 to 5.0 IU of hyaluronidase in each nodule, five years after the filling procedure, with the complete recession of the lesions after one week. 19
In the same year, Lambros used 75 IU hyaluronidase (Lee Pharmacy, Inc., 50 IU/cc), diluted in 1.5 ml of 0.5% lidocaine with epinephrine in a nodule formed by excess filling substance in the lower eyelid, and obtained 90% improvement in the first 24 hours. 20 Vartanian conducted the first prospective study that consisted of injections of hyaluronic acid gel in both forearms of 12 volunteers. Subsequently, 0.5 ml of 0.9% saline was injected on one side, and 75 IU hyaluronidase were injected on the other side. There was a dramatic decline of palpation scores in the side treated with hyaluronidase, between the fourth and tenth day. 3, 5
Tyndall effect
Hirsch at al. described the case of a 44-year-old woman who underwent cutaneous filling (Juvederm®) in the right nasojugal fold performed by a inexperienced professional, and subsequently developed a large bluish nodule in the region four days later. Seventy-five IU (75 IU) of hyaluronidase (Vitrase®) were injected in the lesion, with the complete regression of the nodule in four days. There was recurrence after a few days, at which time a decision was made for a new treatment with an additional 75 IU. The patient recovered uneventfully during a seven-month follow up. 3, 5, 16 Andre and Levy reported the case of a 25 year-old patient who developed bluish nodules in both lower eyelids one month after undergoing cutaneous filling (Surgiderm®) in the dark circles. One hundred and twelve point five IU (112.5 IU) of the enzyme (Desinfitral, Aesthetic Dermal, UK) were injected in each of the nodes via serial punctures. Within ten minutes a decrease in the volume of the lesions was visible, with a reduction of 50% after one hour and complete disappearance of the nodule after 12 hours of application. 6
Granulomas
In 2005, Brody published a case of a 68-year-old female patient who developed inflammatory nodules in the region of the mentum and labial commissure one week after undergoing cutaneous filling in these areas with hyaluronic acid. 8 She had already received multiple injections of collagen in the glabella and the labial commissure in the previous 19 years. The culture of the aspirated fluid was negative for aerobic and anaerobic bacteria, and the biopsy showed dermal fibrosis with chronic granulomatous inflammation foci. Subsequent treatment with intralesional injection of triamcinolone acetonide (3 mg/ml), oral antibiotics (cephalexin, trimethoprim-sulfamethoxazole) and short courses of systemic corticosteroids resulted in a minimal and unsustained response. Five months later, the patient still had an inflammatory nodule on the right side of the mentum. Fifteen IU (15 IU) of hyaluronidase were injected in the lesion (0.2 ml of solution with 75 IU), with complete regression in 24 hours, without recurrence.
Vascular occlusion
In 2007, Hirsch at al. described the first case of vascular occlusion by hyaluronic acid successfully treated with hyaluronidase. 17 A 44-year-old female patient underwent multiple injections in the deep dermis of the nasogenian sulcus, with the retrograde technique. The immediate result was excellent, however, six hours after the procedure there was vascular occlusion in the irrigation area of the angular and upper labial arteries, in the right hand side. The patient was treated with 650 mg of aspirin, topical nitroglycerin, local heat, and injection of 30 IU of hyaluronidase in the deep dermis and subcutaneous tissue of the affected area, through multiple punctures. Eight hours after there was not any sign of vascular damage in the region. In 2011, Kim at al. reported the case of four patients with vascular occlusion after cutaneous filling with hyaluronic acid in the nasal region. 18 Only two of them received subcutaneous injection of hyaluronidase on the day after the procedure. The use of such medication, however, did not show any benefit. All developed some degree of skin necrosis and scarring. In light of this result, the authors selected ten mice and injected 0.25 ml of hyaluronic acid (Restylane) in each of their ears. The filler was precisely injected into the posterior auricular artery of both ears of each mouse, with 750 IU hyaluronidase (Hylunidase®; BMIkorea, Jeju, Korea) being injected into only one of them. In five rats, the administration of hyaluronidase was performed four hours after the injection of hyaluronic acid while in the other five, this interval was of 24 hours.
The group treated after four hours showed a significant reduction of necrosis (p<0.05), a fact that did not occur in the group treated after 24 hours.
It was concluded that the early injection of hyaluronidase reduces the filler's vascular complications, however its use has no benefit 24 hours after the performance of the procedure.
In 2014, DeLorenzi developed an in vitro study aimed at evaluating whether the hyaluronidase was able to permeate the wall of the intact human facial artery to hydrolyze the HA filling. 21 Small segments of human facial artery from fresh cadavers were filled with monophasic hyaluronic acid (Juverderm Ultra Plus XC®), acquiring the appearance of "sausages". They were subsequently immersed in 300 IU hyaluronidase (private dispensing chemist) or in saline (control). Four and 24 hours later, the vessels were removed from the preparations, having one of the ends opened. Only the segments immersed in hyaluronidase showed degradation of the filler, after 4 and 24 hours. The conclusion was that the study supported the hypothesis that the enzyme can effectively hydrolyze the AH through the intact arterial wall.
There is no consensus in the literature regarding the recommended dose of hyaluronidase. Generally, the used and suggested amount by the references varies between 5 and 75 IU.
In 2007, Soparkar used 375 IU hyaluronidase for dissolving a hyaluronic acid filling (Restylane®) in the face of a patient. Despite the high dose employed, there was no change in the natural volume of the treated area. In the author's opinion, the recommended dose ranges from 150 to 200IU of hyaluronidase for each 1 ml of hyaluronic acid to be removed. 22 In 2010, a case report described a successful treatment of nodules in the lower eyelids, caused by excess filling substance (Juverderm Ultra®), with only 3 IU of hyaluronidase (Hynidase® - ovine hyaluronidase 1.500 IU/vial, Shreya life sciences Pvt. Ltd., India). 23
Jones at al. performed an in vitro study in order to assess the response to hyaluronidase of fillers with different concentrations of hyaluronic acid (24 mg/ml fluid gel; 20 mg/ml particulate gel, 5.5 mg/ml particulate gel with lidocaine). 24
The study showed that the degradation of hyaluronic acid depends on the concentration of the product used and time of incubation with hyaluronidase. The 24 mg/ml hyaluronic acid gel showed the greater resistance to degradation in vitro, probably due to the higher concentration and greater crosslinking and cohesiveness, according to the authors' findings.
Finally, the authors suggest that for every 0.1 ml of hyaluronic acid to be treated (in vivo), 5 IU hyaluronidase should be used for the 20 mg/ml gel or 10 IU for the 25 mg/ml gel. In 2014, Rao et al. exposed four types of HA based fillers to various concentrations of hyaluronidase in vitro. 25 The form and consistency of such fillers were analyzed after one and five minutes of exposure. The duration and dose-response were assessed by visual comparison of photographs.
They subjected 0.2 ml of the cutaneous fillers Restylane® (20 mg/ml), Juvéderm® (24 mg/ml), Belotero® (22 mg/ml) and Juvéderm Voluma® (20 mg/ml) to 15 and 30 IU of Hylenex®. Belotero® was the least affected by the exposure, regardless of the hyaluronidase dose and maintaining its shape even after five minutes. Restylane® was the most affected and became moderately liquefied after the exposure to 30 IU of Hylenex® for five minutes. Juvéderm® and Juvérderm Voluma® showed an intermediate result. In summary, after exposure to Hylenex®, Belotero® was the least affected, followed by Juvéderm®, Juvéderm Voluma® and Restylane®.
The reaction of the enzyme to all fillers was dependent on both time and dose. The degree of degradation of the fillers correlated with the degree of crosslinking of the product. Belotero® was the most resistant because of its more cohesive monophasic nature. The study also suggests that doses lower than 15 IU of Hylenex® might not cause noticeable changes in the structure of the tested fillers.
The adverse effects of hyaluronidase are infrequent, and are mainly represented by reactions at the application site. 3-6, 10-12 Soparkar at al. reported temporary pruritus after the injection of the enzyme in only two of the 97 patients treated. 3, 5
Angioedema and urticaria are reported in less than 0.1% of patients.10-12 However, there are still no reports of anaphylactic reactions after intradermal use of hyaluronidase. 3-5, 16
The potential risk of spongiotic encephalopathy is associated with the use of bovine hyaluronidases that are illegally manufactured under non-sterile conditions. 8, 16, 24 Undergoing a preliminary cutaneous test is recommended in the leaflets accompanying medicines, and the use of hyaluronidase is contraindicated in positive tests. 3, 10-13 For the test, three units of hyaluronidase are injected into the intradermal region, typically in the anterior surface of the forearm, and within five minutes an erythematous papule with local heat is observed, characterizing a positive test. The presence of transient erythema or macular vasodilation do not mean positivity. 8, 10, 12, 16
Some authors, however, disagree on the testing requirement, arguing that the occurrence of adverse effects after intradermal use of such medication is extremely rare and that allergic reactions can occur even with a negative skin test. 5
Some medications, such as cortisone, estrogen, adrenocorticotropic hormone, salicylates and antihistamines seem to make the tissues partially resistant to the enzymatic action of hyaluronidase. 3, 8, 10-12, 16
Furosemide, benzodiazepines, and phenytoin appear to be incompatible with hyaluronidase. 10-12.
During pregnancy, this medication is considered category C (animal studies have shown that the drug can have teratogenic effects or be toxic to embryos, nevertheless there are no controlled studies in women). 3, 10-12 Also, it should not be applied in patients allergic to bee stings, for hyaluronidase is one of the components of their venom. 3, 16, 18
Another important contraindication is the presence of an infectious process in the site to be treated. Due to the potential risk for the spread of infection, hyaluronidase should not be used or, if necessary, be associated with systemic antibiotics. 3, 5, 10-13, 16
After adequate asepsis and antisepsis of the site, the marking of area to be treated should be carried out. Hylenex®, Amphadase® and Vitrase® are preparations ready for use. 10-12 Hyalozima® needs to be prepared by dissolving hyaluronidase powder (2,000 UTR) in 5 ml of diluent supplied with the product. The resulting solution has 400 IU/ml. 13 Hyalase® can be diluted in 1 ml of distilled water or added directly to the solution to be used. 14
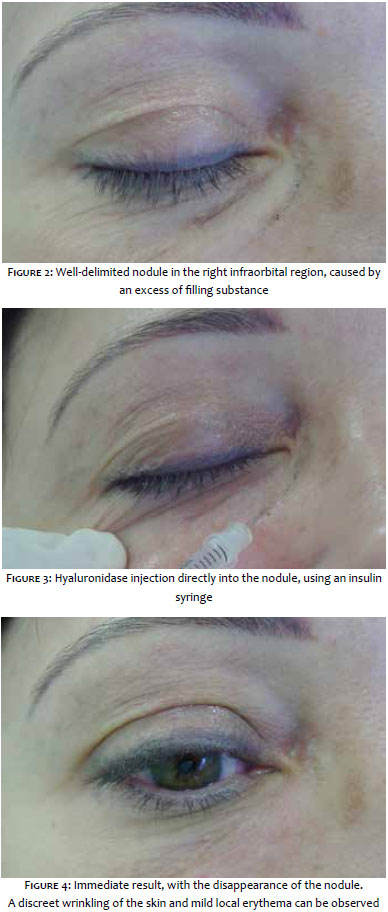
The authors aspirated the solution in insulin syringes of 0.3 ml, resulting in 4 IU for each 0.01ml (smaller scale of the syringe), and then injected 0.01 - 0.03 ml of the solution in each nodule (Figures 2 to 4).
When the solution is older and kept under refrigeration, it is possible to notice that there is more resistance in the injection, "locking" the syringe. This takes place due to the slight increase in the viscosity of the solution. It can, however, be observed that the product remains effective, since there is immediate dissolution of the hyaluronic acid accumulation after local injection.
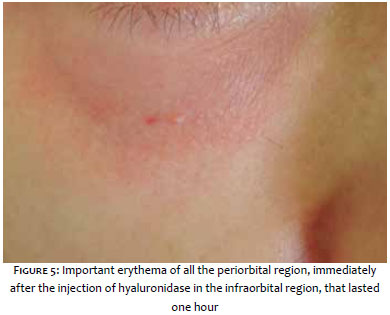
Edema and erythema (Figure 5), and discreet wrinkling of local skin immediately after the procedure (Figure 4), are the most frequent side effects, lasting 30-50 minutes and subsequently disappearing completely.
Hyaluronidase should always be easily accessible to dermatologists who perform cutaneous filling with hyaluronic acid and should be available at the practice for emergencies.
The patient to be treated should be informed about the off-label use of hyaluronidase.
There is no evidence that adding lidocaine or epinephrine is beneficial. 5
It is recommended that hyaluronidase solutions be used within 12 hours after the preparation, for they rapidly lose the viscosity, reducing activity at room temperature. 3 In the authors' experience, if kept in the refrigerator they can be used within 30 days, without losing effectiveness.
The needle's gauge should be adequate for the size and location of the lesion. A 30G needle can be used in superficial nodules. In deeper ones, 26 or 27G needles can be used. 5
Hyaluronidase should be injected, where possible, into the HA deposit. When this deposit is very superficial, the injection should be applied just below the site. 5
Hyaluronidase should not be used in areas treated with botulinum toxin in the previous 48 hours, due to the risk of diffusion. 5
The hyaluronidase enzyme is able to hydrolyze HA, increasing the permeability of the skin and connective tissue. Although not approved by the FDA, the use of this enzyme in dermatology has achieved prominence due to the increased number of cutaneous fillings containing HA. Studies have shown the efficacy of hyaluronidase in the treatment of nodules arising due to an excess of filling material, asymmetries, Tyndall effect, and even in cases of granuloma formation and vascular occlusion. There are several commercial presentations that are differentiated primarily by the origin of the product (bovine, ovine or human recombinant), and are related to low levels of adverse effects.
Currently, hyaluronidase is essential for every dermatologist who performs dermal fillings with HA. The personal experience of each professional will be important in determining how to use the enzyme, since there is no consensus in the literature regarding the dose used and the application technique.
1. Wohlrab J, Finke R, Franke WG, Wohlrab A. Clinical trial for safety evaluation of hyaluronidase as diffusion enhancing adjuvant for infiltration analgesia of skin with lidocaine. Dermatol Surg. 2012;38(1):91-6.
2. Bordon KCF. Caracterização funcional e estrutural da hialuronidase isolada da peçonha de serpente Crotalus durissus terrificus [Tese de Doutorado]. Ribeirão Preto: Faculdade de Ciências Farmacêuticas de Ribeirão Preto-Universidade de São Paulo; 2012.
3. Lee A, Grummer SE, Kriegel D, Marmur E. Hyaluronidase. Dermatol Surg. 2010;36(7):1071-77.
4. Dunn AL, Heavner JE, Racz G, Day M. Hyaluronidase: A review of approved formulations, indications and off-label use in chronic pain management. Expert Opin Biol Ther. 2010;10(1):127-31.
5. Rzany B, Becker-Wegerich P, Bachmann F, Erdmann R, Wollina U. Hyaluronidase in the correction of hyaluronic acid-based fillers: a review and recommendation for use. J Cosmet Dermatol. 2009;8(4):317-23.
6. Pierre A, Levy PM. Hyaluronidase offers an efficacious treatment for inaesthetic hyaluronic acid overcorrection. J Cosmet Dermatol. 2007;6(3):159-62.
7. Cassuto D, Sundaram H. A problem-oriented approach to nodular complications from hyaluronic acid and calcium hydroxylapatite fillers: Classification and recommendations for treatment. Plastic and Reconstructive Surgery. 2013;132(4 suppl 2):48S-58S.
8. Brody HJ. Use of hyaluronidase in the treatment of granulomatous hyaluronic acid reactions or unwanted hyaluronic acid misplacement. Dermatol Surg. 2005;31(8 Pt 1):893-7.
9. Stern R, Jedrzejas MJ. The hyaluronidases: Their genomics, structures, and mechanisms of action. Chem Rev. 2006;106(3):818-39.
10. Hylenex® [package insert]. Halozyme Therapeutics, Inc: San Diego, California, USA, 2012.
11. Vitrase® [package insert]. Bausch & Lomb, Inc: Tampa, Florida, USA, 2012.
12. Amphadase® [package insert]. Amphastar Pharmaceuticals, Inc: Rancho Cucamonga, California, USA, 2013.
13. Hyalozima® [package insert]. Apsen, Inc: São Paulo, São Paulo, Brasil, 2012.
14. Hyalase® [package insert]. Sanofi-Aventis, Inc: Macquarie Park, Nova Gales do Sul, Austrália, 2010.
15. Costa IMC, Gadelha AR. Cirurgia Dermatológica em Consultório. 2ª ed. São Paulo: Atheneu; 2009.
16. Hirsch RJ, Brody HJ, Carruthers JD. Hyaluronidase in the office: a necessity for every dermasurgeon that injects hyaluronic acid. J Cosmet Laser Ther. 2007;9(3):182-5.
17. Hirsch RJ, Cohen JL, Carruthers JD. Successful management of an unusual presentation of impending necrosis following a hyaluronic acid injection embolus and a proposed algorithm for management with hyaluronidase. Dermatol Surg. 2007;33(3):357-60.
18. Kim DW, Yoon ES, Ji YH, Park SH, Lee BI, Dhong ES. Vascular complications of hyaluronic acid fillers and the role of hyaluronidase in management. J Plast Reconstr Aesthet Surg. 2011;64(12):1590-5.
19. Soparkar CN, Patrinely JR, Tschen J. Erasing restylane. Ophthal Plast Reconstr Surg. 2004;20(4):317-8.
20. Lambros V. The use of hyaluronidase to reverse the effects of HA filler. Plast Reconstr Surg. 2004;114(1):277.
21. DeLorenzi C. Transarterial degradation of hyaluronic acid filler by hyaluronidase. Dermatol Surg. 2014;40(8):832-41.
22. Soparkar CN, Patrinely JR, Skibell BC, Tower RN. Hyaluronidase and restylane. Arch Facial Plast Surg. 2007;9(4):299-300.
23. Menon H, Thomas M, D'silva J. Low dose of Hyaluronidase to treat over correction by HA filler - a case report. J Plast Reconstr Aesthet Surg. 2010;63(4):e416-7.
24. Jones D, Tezel A, Borrell M. In vitro resistance to degradation of hyaluronic acid dermal fillers by ovine testicular hyaluronidase. Dermatol Surg. 2010;36(Suppl 1):804-809.
25. Rao V, Chi S, Woodward J. Reversing facial fillers: Interactions between hyaluronidase and commercially available hyaluronic-acid based fillers. J Drugs Dermatol. 2014;13(9):1053-6.
The present study was conducted at Hospital do Servidor Público Municipal de São Paulo - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}