


Marisa Gonzaga da Cunha1; Ana Lucia Gonzaga da Cunha2; Carlos A. Machado3
Keywords: ADIPOCYTES; LYMPHATIC SYSTEM; LIPODYSTROPHY
Despite having become the norm, the term cellulite is mistakenly used to describe a regional hypodermic dystrophy almost exclusive to the female population, which can be associated or not with gynoid-type obesity, and which affects the region of the hips, buttocks, lower limbs and, less frequently, the abdomen and the lateral-posterior face of the arms. It has genetic and constitutional factors that predispose an individual to the condition, factors to which multiple complex and interrelated etiologies are part of the equation. Cellulite, or gynoid lipodystrophy (GLD) in its various degrees is extremely common among females, with onset typical between the ages of 15 and 45 years, corresponding to a woman's reproductive phase. About 95% of women will present some degree of cellulite at some point in life. 1
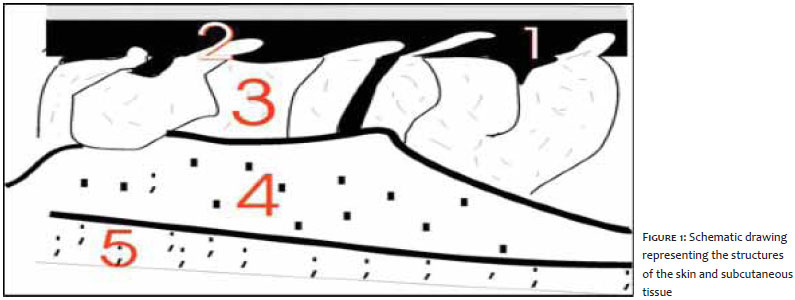
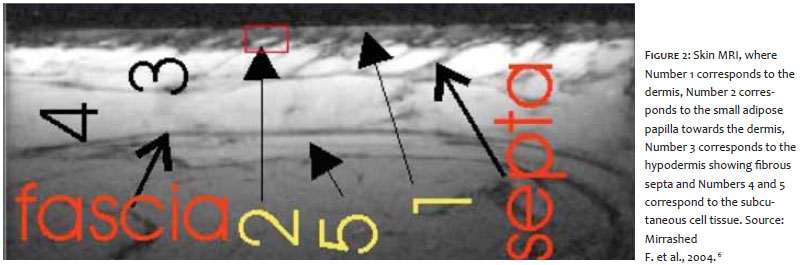
Despite the clear anatomical distinction between the dermis and hypodermis, the two are structurally and functionally integrated through the network of vessels and nerves and the presence of epidermal appendages. 2 The hypodermis or superficial adipose tissue (SAT) is arranged in vertical compartments, distributed perpendicularly to the skin's more superficial layers, with a structure similar to a honeycomb, with uniform distribution throughout the tissue. 3 It is formed by fatty lobules interspersed with well-defined fibrous septa (reticula cutis superficialis) composed of elastic and collagen fibers that are oriented perpendicularly towards the surface, strongly anchored to the dermis, and connecting it with the fascia superficialis. These fatty lobules, located between the dermis and the fascia superficialis serve as a passage to vessels and nerves from the subcutaneous tissue, with compartments that are well-vascularized by capillary vessels 4-7 (Figures 1 and 2).
This distribution in septa pattern plays an important role in preserving cell integrity. 2 The fatty lobules are organized into single or multiple layers depending on the fat content and each individual's SAT thickness. Its thickness increases and decreases according to weight gain during specific situations that determine the formation of GLD. It is important to note that the subcutaneous tissue, or localized fat, is located underneath the skin and that its fatty content is independent of the cells of the hypodermis. 2
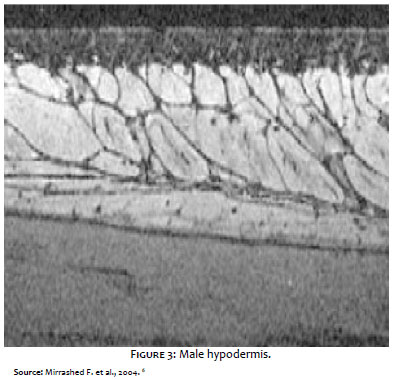
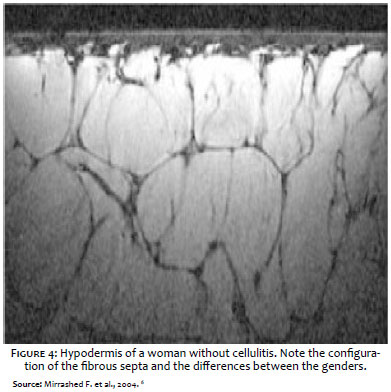
GLD is an exclusively female condition due to the anatomical characteristics of the hypodermis in women, in which the lobes are larger and have parallel septa, while in men the fibrous septa are smaller and arranged in oblique planes, with small fat lobules.6 (Figures 3 and 4).
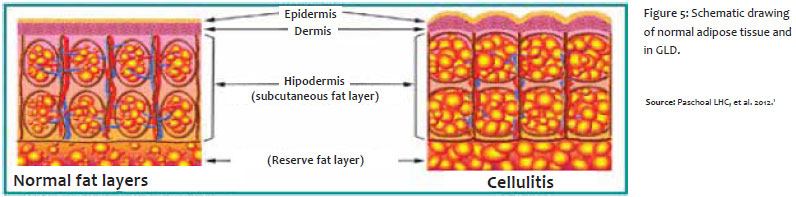
These distinct structures are present in each gender at birth, but due to the hormonal and vascular changes that take place during puberty - when a greater storage of fat and increased interstitial fluid retention occur - the fat lobules increase due to the hypertrophy of adipocytes 1, 7 (Figure 5). Macroscopic anatomical studies of adipose tissue on cadavers has evidenced the arched distribution of women's adipose conjunctive tissue bands within the panniculus, with a protrusion of fat at the dermo-hypodermal interface - which would explain the formation of the skin's dimpled appearance, with an increased volume of adipocytes. This distribution occurs specifically in women due to the presence of vertical fascial bands. Herniations in the dermis are characteristic of the female anatomy, and their presence was confirmed by high-resolution magnetic resonance in the low-density regions of the dermis 6 (Figures 3 and 4).
Pathophysiology
Success in the treatment of GLD is closely linked to the understanding of its physiopathology. 7-9 The present article will review the concepts and the etiologic factors involved in its onset and development.
GLD was defined by Merlin as a "segmental or localized lipodystrophy of the subcutaneous connective tissue with respect to the regional venous-lymphatic stasis. This dermohypodermosis prefigures a hystangiopathy with a fibroblastic response that precedes the alterations of the capillary-venular segment and is maintained by them." 1
Under normal conditions, the arterial system joins the venous system through small capillaries, in a way in which blood is never free in the tissues. In this junction area, vessels cease filtering the colorless substance (interstitial fluid) that surrounds all body cells and which contains necessary nutrients to eliminate waste, which will in turn be drained through the venous system. This mechanism is called the Starling principle. The interstitial fluid is not fully reabsorbed, and the remaining amount is collected and drained to the lymph channels. The first alteration of GLD takes place during this lymphatic drainage, which is carried out inefficiently, generating waste.
The connective tissue is then infiltrated by the interstitial fluid and its waste. This happens in the simple congestive phase, which may be transient or permanent. This interstitial edema, in turn, compresses the capillary vessels, hindering the return of circulation and accentuating the stasis and the permeability of the vascular wall, which increases the exudation. A vicious cycle then ensues, leading some authors to state that "cellulitis has the property of producing more cellulitis".
In a review article, Rossi and Vergnanini described the multifactorial basis for the etiology of GLD. The process would originate with the deterioration of cutaneous vascularization, particularly in response to alterations in the pre-capillary arteriolar sphincter of the affected areas, along with the deposition of hyper polymerized glycosaminoglycans on the wall of dermal capillaries and between the collagen and elastic fibers. The increase in capillary pressure would lead to increased permeability of venular capillaries and the retention of excess fluid in the dermis, among adipocytes and interlobular septa, causing cellular alterations and tissue hypoxia. 10
The increased lipolytic resistance resulting from hypoxia and increased lipogenesis, the latter caused by the action of estrogen, prolactin, and high-carbohydrate diets, would lead to hypertrophy of adipocytes. The widened adipocytes, along with hypertrophy and hyperplasia of periadipocyte reticular fibers, would form micronodules surrounded by protein fragments that subsequently cause the sclerosis of fibrous septa, leading to the appearance of GLD. The overall effect of this process would be a reduction in the blood flow and lymph drainage. 1
Therefore, it is possible to conclude that GLD is a dystrophic process of complex pathophysiology, with multiple interlinked factors that act through different mechanisms in multiple target elements in the dermal connective and adipose hypodermic tissues, on a genetically predisposed ground, where estrogen is a trigger and which, added to several other contributing endogenous factors and exacerbated by general and local exogenous factors, sets off a slow and progressive cascade reaction.
Due to the complex inter-relationship between the etiological factors that act directly or indirectly in the pathophysiology of GLD, and for a better understanding of this condition, it is convenient to separate the structures of the dermo-hypodermic region into "operating units", nevertheless bearing in mind that their actions are simultaneous and obey a central integrator command that is effected by different reflex pathways. GLD's pathophysiology can be explained by the complex and interconnected participation of the four operating units in that tissue. 1
Due to their primary role, fibroblasts - cells responsible for the interstitial matrix unit (IMU) function and which presumably would start the vicious cycle of this condition - should be mentioned. These mesenchymal stem cells, stricken in different harmful ways, primarily alter the turnover of extracellular macromolecules with physico-chemical and structural alterations in glycosaminoglycans and proteoglycans, which constitute the amorphous matrix (fundamental substance, basal membrane, and lining of the cells' surface) and the fibrillar matrix (collagen and elastin). As a result, changes in the biological functions would take place, which would cause secondary changes in the diffusion of nutrients, metabolites, hormones, and neurotransmitters among the tissue cells, the microcirculatory system (microcirculatory unit - MCU) and the sympathetic nerve endings (neurovegetative/autonomic unit - NVU), influencing the functional properties of neuroreceptors, and thus impairing cellular differentiation, the cell/cell and the cell/matrix interactions. In this way, the phenomena occurring in the energetic- adipose unit (EAU), with hypertrophy and resistance to the lipolysis of regional adipocytes, are also explained. Furthermore, there are also variations in the pressures of the various tissue compartments with edematous gelloid infiltration (non-mobile) of the interstitial matrix, fibrotic phenomena of interlobular connective trabeculae and finally the vasculopathic and hemodynamic alterations in the microcirculation.
The proliferation and activity of fibroblasts are regulated by the various factors that can cause modifications in the matrix proteoglycans: individual and regional characteristics; age (more cells in the embryonic stage and fewer cells in the senile stage); estrogens (which determine the increased production of hyaluronic and chondroitin sulfuric acids); pregnancy (with increased production of hyaluronic acid and glycosaminoglycans); hypothyroidism (with increased production of hyaluronic and chondroitin sulfuric acids); diabetes (with reduction in the production of glycosaminoglycans and increased heparin); corticosteroids (hydrocortisone inhibits the production of hyaluronic and chondroitin sulfuric acids and heparin, prednisone reduces the production of chondroitin sulfuric acid and increases that of hyaluronic acid); and free radicals (the superoxide depolymerizes the hyaluronic acid).
Regarding histological aspects, GLD has three development stages:
- The initial stage is characterized by alterations in the hypodermis, which differs from the normal adipose tissue by the existence of deformed adipocytes associated with lymphatic stasis, with points of micro-hemorrhages and proliferation of fibroblasts.
- In the second phase, the fibroplasia intensifies, with neocollagenesis and capillary neoformation in addition to mild edema foci in the dermis. This phase corresponds to the appearance of "orange peel". It is called initial edematous fiber sclerodermic panniculopathy.
- The third phase is represented by the intensification of the foregoing phenomena, corresponding to an edematous fiber sclerodermic dermal panniculopathy with collagen hyperplasia and sclerosis of the conjunctive bands of the hypodermis and deep dermis, which clinically correspond to palpable nodules.
It is always important to bear in mind that while the cosmetic concern is relevant, GLD is a cutaneous disorder that can only be controlled and not completely cured, since it is not a true disease, but a predisposition.
GLD Grade I is a secondary characteristic in women, while GLD Grade II can occur at some varying point in a woman's life - during pregnancy or hormonal treatment, for instance. However, although the treatment is only moderate and temporarily effective, 11 persistent cases or more advanced stages should be considered pathological and thus treated and monitored, since they are indicative of peripheral vascular disease.
1. Paschoal LHC, Cunha MG, Ciporkin H. Fisiopatologia e Atualização Terapêutica da Lipodistrofia Ginóide - Celulite. 2 ed. rev e ampl. Rio de Janeiro: Di Livros Ed. Ltda; 2012. p.79-110.
2. Cunha MG, Cunha ALG, Machado CA. Hipoderme e tecido adiposo subcutâneo - duas estruturas diferentes. Surg Cosmet Dermatol. 2014;6(4):355-9.
3. Sbarbati A, Accorsi D, Benati D, Marchetti L, Orsini G, Rigotti G, et al. Subcutaneous adipose tissue classification. Eur J Histochem. 2010;54:226-30.
4. Lancerotto L, Stecco C, Macchi V, Porzionato A, Stecco A, De Caro R. Layers of the abdominal wall: anatomical investigation of subcutaneous tissue and superficial fascia. Surg Radiol Anat. 2011;33(10):835-42.
5. Lookwood TE. Superficial Fascial System (SFS) of the trunk and extremities: a new concept. Plast Reconst Surg. 1991;87(6):1009-18.
6. Mirrashed F, Sharp JC, Krause V, Morgan J, Tomanek B. Pilot study of Dermal and Subcutaneous Fat Structures by MRI in Individuals that differ in Gender, BMI, and Cellulite Grading. Skin Res Technol. 2004;10(3):161-8.
7. Proebstle TM. Cellulite. Hautarzt. 2010;61(10):864-72.
8. Khan MH, Victor F, Rao B, Sadick NS. Treatment of cellulite: Part I. Pathophysiology. J Am Acad Dermatol. 2010;62(3):361-72.
9. de la Casa Almeida M, Suarez Serrano C, Rebollo Roldán J, Jiménez Rejano JJ. Cellulite,s aetiology: a review. J Eur Acad Dermatol Venereol. 2013;27(3):273-8.
10. Rossi AB, Vergnanini AL. Cellulite: a review. J Eur Acad Dermatol Venereol. 2000;14(4):251-62.
11. Wanner M, Avram M. An evidence-based assessment of treatments for cellulite. J Drugs Dermatol. 2008;7(4):341-5.
This study was performed as part of the Dermatology Program at the Faculdade de Medicina do ABC (FMABC) - Santo André (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}