


Lorena Rodrigues Teixeira E. Silva1; Ana Maria Quinteiro Ribeiro2; Luiz Fernando Fróes Fleury Júnior3
Keywords: CARCINOMA, SQUAMOUS CELL; SCALP; WOUND HEALING
Approximately 90% of skin cancers occur on the head and neck as a result of the cumulative damage of ultraviolet radiation. 1 Squamous cell carcinoma (SCC) is the second most common malignant skin tumor, accounting for about 20% of non-melanoma skin tumors. 2 Most lesions occur in sun-exposed areas with severe actinic damage.
This neoplasia can substantially contribute to morbidity and mortality in elderly patients. 2 The risk of local recurrence is 3-16% and less than 5% for metastasis, however that percentage can be higher in high-risk tumors, reaching 15-38%. 1-6
Larger tumors (from 2 cm in diameter, or greater than 2 mm in thickness), more aggressive histological subtypes, perineural invasion, and those located on the lips and ears are considered to be high-risk lesions.
The authors present the surgical approach to SCC on the scalp of patients with advanced tumors who also have a history of chronic exposure to the sun, and that were treated at the Dermatology Department of the Hospital das Clínicas, Universidade Federal de Goiás
Four SCC cases on the scalp, observed over two years, will be described (in patients ranging from 72 to 92 years, 3 men and 1 woman). Photographs were taken before and after tumor resection. The surgeries were performed under local anesthesia with tumescent solution, involving sedation when necessary.
Case 1
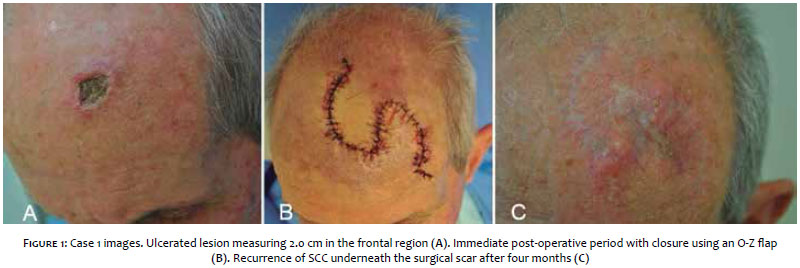
A 78-year-old male patient, with an ulcerated lesion in the frontal region measuring 2 cm in diameter (Figure 1A). An excision with a 0.5 cm margin and O-Z flap closure were performed (Figure 1B). Pathological examination revealed a well-differentiated SCC, with a thickness of 0.5 cm and free margins, which nevertheless were minimal in depth, without perineural invasion. There was recurrence beneath the surgical scar four months after (Figure 1C). Computerized Tomography (CT) scan showed an absence of bone invasion. A new excision was performed including the periosteum, without the closure of the surgical wound. There was healing by secondary intention within three months (Figure 2). There was no recurrence in the 13-month follow-up.
Case 2
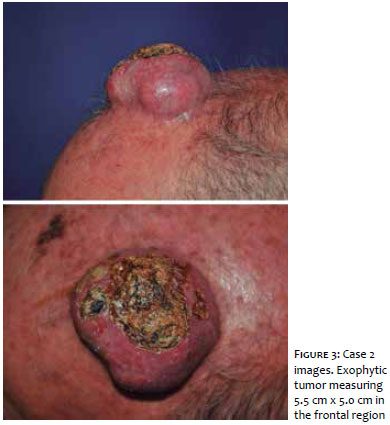
A 72-year-old male patient with a 5.5 cm x 5.0 cm SCC on the forehead (Figure 3). The tomography showed a thickness of 2.0 cm without periosteal invasion. The excision of the lesion was carried out with a 0.5 cm margin. The pathology revealed a moderately differentiated, 2.5 cm thick SCC, with free margins (however minimal in depth), without perineural invasion. A graft was performed on the area with good granulation, after one month (Figure 4). The 28-month follow-up evidenced no recurrence.
Case 3
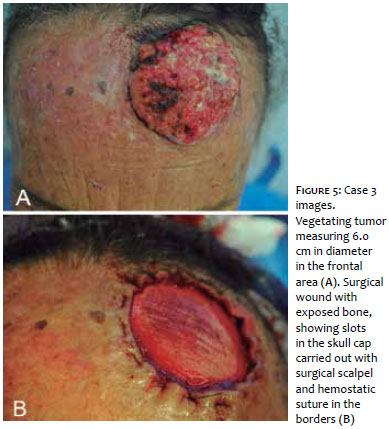
A 77-year-old female patient with a vegetating lesion on the forehead (Figure 5). A skull CT scan ruled out bone invasion. Excision was carried out and a graft over an area with good granulation was performed one month after (Figure 6). Pathological examination showed a moderately differentiated 2.4 cm thick SCC, with free margins without perineural invasion. Recurrence took place at the graft's edge after one year with a new local excision performed. There is no record of recurrence in the 14-month follow-up.
Case 4
A 92-year-old male patient with a left temporal tumor measuring 7.0 cm in diameter (Figure 7). The skull CT scan did not show bone invasion. An excision with a 0.5 cm margin was performed, with the deep margin having been extended due to clinical observation of involvement of the periosteum. There was complete healing by secondary intention in three months. The patient died six months later due to pneumonia.
Four patients with SCC on the scalp were operated on. It was observed that all had a history of chronic exposure to the sun. The male patients also had some degree of androgenetic alopecia. The lesions were large and thick (0.5 cm to 2.4 cm); the preferred option was to perform a wide excision with closure in a second surgical stage. None of the patients had compromise of the skull cap. A primary lesion flap was carried out in one patient, with recurrence beneath the surgical scar in four months. In the re-treatment however, the lesion was even larger, and the preference was given for healing by secondary intention. Due to the local anatomy, all patients showed limited deep margins despite the fact that the excision had reached the periosteum, and two patients had local recurrence in the observed period.
Four SCC cases on the scalp were reported. They had tumors of large diameters and thicknesses in common. The choice of surgical method was a challenge for the medical team. The majority of SCC cases reported in the literature occur in the head and neck, and 8.3% to 25.2% of these affect the scalp. 3, 4 In a recent study carried out in Australia, 10% of patients with nodal metastasis had primary lesions in the scalp. 7 The main sites of metastases are the cervical lymph nodes and the parotid. 5, 6
Primary characteristics of SCC have been studied and can serve as predictors for neoplasias with worse prognoses. The American Joint Committee on Cancer (AJCC) has established criteria for the staging of high-risk primary tumors as follows: diameter > 2.0 cm, thickness > 2 mm or Clark level > IV, perineural invasion, located on the ear and lip, and poorly differentiated or undifferentiated. 5, 7 Recurrent tumors are biologically more aggressive. Thus, the therapeutic choice should take into account the prognostic factors. According to these criteria, the four patients described had high-risk SCCs.
Four-millimeter margins are recommended for "low risk" SCCs while 6.0 mm margins are recommended for "high risk" SCCs in order to achieve 95% free margins histologically. 1, 7 Mohs micrographic surgery is considered a first-line treatment for larger tumors. 2, 7 With scalp lesions, it is difficult to reach the deep margin due to the fact that it is restricted to the anatomical thickness. This region has the greatest rate of incomplete excision. 1, 4 After surgery, the patient should be followed up with regularly, at intervals of four to six months. 7
Ninety percent of recurrences and metastases occur in the first five years. 2 There are not enough studies existing to form consensus on the performance of adjuvant radiotherapy, sentinel lymph node biopsy, and prophylactic lymphadenectomy. 7
Due to the fact that Mohs surgery was unavailable where the study was conducted, a decision was made to not correct the defect during the first surgical episode, and to wait for the pathology results containing the evaluation of margins.
The scalp is an anatomical region of thick, inelastic tissue. Commonly used for the correction of full thickness defects in this region, flaps can be disadvantageous in extensive defects due to the inelasticity of the regional skin. 8 In the four cases studied, due to the fact that they were high-risk tumors, conducting flaps would hamper re-treatment if there were positive margins or recurrence arising from distortion of the surgical site. Flaps were also not chosen due to the advanced age of the patients, since this would increase the time needed for their surgery.
In the case of two patients, the complete healing occurred by second intention within three months, while in the other two patients autologous skin grafts were performed after complete granulation. In patients requiring excision of the periosteum, the curettage of the outer layer of the skull was performed. The objective was to reach the diploic space, which is highly vascularized, achieving the granulation that enables the regeneration of the epithelium or the implementation of a skin graft. 8 The aesthetic and functional results were satisfactory, mainly due to the fact that the patients were bald. Choosing not to perform flaps has facilitated the follow-up of local recurrence, as in Case 3.
Treatment of SCC on the scalp with wide excision and without closure flaps during the first operative event is an option for high-risk tumors. This technique allows the evaluation of local recurrences without anatomic distortion of the bed, since long-term follow up is recommended. It also allows short surgeries and less post-operative morbidity, which can be decisive in the case of elderly patients. On the downside, caring for the surgical wound is laborious and it can take several weeks to achieve complete healing. The scar area will be left without hairs and with thinner skin, becoming more fragile and therefore more susceptible to injuries.
1. Jenkins G, Smith AB, Kanatas AN, Houghton DR, Telfer MR. Anatomical restrictions in the surgical excision of scalp squamous cell carcinomas: does this affect local recurrence and regional nodal metastases? Int J Oral Maxillofac Surg. 2014;43(2):142-6.
2. Alam M, Ratner D. Cutaneous Squamous Cell Carcinoma. N Engl J Med. 2011;344(13):975-83.
3. Clayman GL, Lee JJ, Holsinger FC, Zhou X, Duvic M, El-Naggar AK, et al. Mortality risk from squamous cell skin cancer. J Clin Oncol. 2005;23(4):759-65.
4. Baker NJ, Webb AA, Macpherson D. Surgical management of cutaneous squamous cell carcinoma of the head and neck. Br J Oral Maxillofac Surg. 2001;39(2):87-90.
5. Ch'ng S, Clark JR, Brunner M, Palme CE, Morgan GJ, Veness MJ. Relevance of the primary lesion in the prognosis of metastatic cutaneous squamous cell carcinoma. Head Neck. 2013;35(2):190-4.
6. Vauterin TJ, Veness MJ, Morgan GJ, Poulsen MG, O'Brien CJ. Patterns of lymph node spread of cutaneous squamous cell carcinoma of the head and neck. Head Neck. 2006;28(9):785-91.
7. Nuño-González A, Vicente-Martín FJ, Pinedo-Moraleda F, López-Estebaranza JL. High-Risk Cutaneous Squamous Cell Carcinoma. Actas Dermosifiliogr. 2012;103(7):567-78.
8. Hoffmann JF. Reconstrução do escalpo. In: Baker SR. Retalhos Locais em Reconstrução Facial. 2ª ed. Rio de Janeiro: Di Livros; 2009. p. 641-67.
This study was performed at the Department of Dermatology, Hospital das Clínicas, Universidade Federal de Goiás (UFG) - Goiânia (GO), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}