


Nilton Di Chiacchio1; Maria Victoria Suarez Restrepo2
Introduction: A topical cosmetic formulation is currently commercially available for the treatment of Brittle Nail Syndrome, a formulation made up of Equisetum arvense, Methyl sulfonyl methane and Hydroxypropyl chitosan. However, the habit of applying nail polish hinders the adherence to treatments that preclude their use. Objective: To propose a scheme that alternates the use of the formulation five times a week, with nail polish. Methods: A clinical, single-blind, crossover controlled intraindividual trial was carried out with 38 female patients. The patients' hands were randomized into two groups (A and B). Results: From weeks 1 to 8, and from Sunday to Thursday, Group A applied the formulation A while Group B did not undergo treatment. In weeks 9 to 16, Group A suspended the application of the formulation, while Group B began treatment. From Thursday to Sunday Groups A and B had their nails painted. A common nail polish was standardized for both groups. A quantitative score was used to evaluate outcomes and observe the percentage of patients who had improvements greater than 50% and 75%. Conclusions: The formulation was more effective in controlling the signs of the syndrome when the nail polish was used in the intervals of the applications. The present study allowed the authors to propose a treatment regimen using the formulation 5 times a week, alternating with the practice of painting the nails.
Keywords: NAIL DISEASES; NAILS; PRODUCTS FOR NAILS AND CUTICLES
Brittle nail syndrome (BNS) is a common complaint. It affects 20% of the general population, and is twice as prevalent in females.1, 2, 3 It is characterized by decreased elasticity and increased fragility of the nails. The most common signs are onychoschizia (lamellar desquamation of the free ungual border), roughness (presence of longitudinal ridges, which can be more or less deep), and onychorexis (longitudinal clefts or fragmentation of the nail plate and/or triangular fragmentation of the free ungual border). 2, 3
Two origins are cited for BNS: idiopathic, or secondary to other skin or systemic diseases.2
In idiopathic BNS, when examined under electron microscopy, it is possible to observe an intrinsic or acquired defect in the intercellular adhesion of keratinocytes, as well as a disorganized structure of proteins, lipids, and keratin fibrils in the nail plate.2-6
The nail's flexibility is determined by its water content (18%) and when this amount is less than 16%, brittleness increases. The lipids present in the nail assist in retaining water. A decrease in the amount of these lipids can promote the manifestation of the syndrome, as occurs after menopause and with exposure to any external agent which leads to water loss. Intercellular junctions between corneocytes seem to be weaker in females. This fragility increases with age, thereby facilitating BNS.7, 8
Secondary BNS is associated with several dermatological or systemic diseases, nutritional deficiencies, drug treatments that affect the ungual matrix or nail plate, and occupational factors.2
The treatment takes into consideration several aspects:2, 3
General measures: avoid trauma, contact with irritants, and dryness. The use of glove is recommended in wet environments or when handling aggravating chemicals. The research and treatment of systemic or dermatological diseases, as well as nutritional deficiencies in cases of onychorexis. The use of emollients containing phospholipids.
In the literature, there are reports of cases of systemic treatment with biotin and topical treatment with tazarotene, however these studies offer a low level of evidence.6, 9
Currently there is a commercially available cosmetic formulation (CF) composed of Equisetum arvense, Methyl sulfonyl methane and Hydroxypropyl chitosan. Equisetum arvense (extracted from a plant) is a source of organic silicon. Nails contain 16 mg of silicon dioxide per 100 g, which seems to contribute to their strength and hardness while maintaining stability among keratin fibrils. 10 Methyl sulfonyl methane is a natural and bioavailable source of sulfur, which seems to improve the quality and growth of the nail plate. 11 Finally, Hydroxypropyl chitosan is a water-soluble film-forming agent and an active principle carrier that promotes the long-lasting adhesion of the nail's surface, with penetration into the ridges, improving the hydration of the nail plate.12, 13
Studies carried out with the daily application of the topical CF for four weeks to treat nail plate alterations of diverse etiologies suggest an improvement of 70-85% in the patients' onychoschizia, as well as in the ungual fragility (90%) and a 20% reduction in the longitudinal ridges.11 The currently recommended regimen is a daily topical application (in the evening) for at least three months, with the complete suspension of cosmetic nail polish use during that period.
For most patients, BNS is an aesthetic problem. Some, however, have reported changes in their quality of life. In Brazil, due to the cultural trend of frequent use of nail polish, which is associated with femininity, hygiene, and personal care, it is most likely that patients will find it difficult to adhere to the daily use of the CF or to maintenance schemes that prevent the application of conventional nail polishes.
For this reason, even though following the daily application scheme of the CF for the treatment of BNS is the ideal approach, the present study was aimed at proposing an alternate safe and effective application scheme that would reconcile the habit of use of the CF with that of having the nails painted with nail polish.
A simple blind, crossover clinical trial was carried out with intra-individual control, with a blinded clinical evaluator and histopathologist physician. The study was approved by the Research Ethics Committee of the Hospital do Servidor Público Municipal de São Paulo, in the State of São Paulo, Brazil.
Women bearing idiopathic BNS, between 18 and 65 years old, who signed the free and informed term of consent, were included. Patients were required to have at least two affected nails on each hand. Blood count, ferritin, serum iron, thyroid profile, glucose, and folic acid were requested for all candidates. Patients with any other disease affecting the nails, secondary brittle nail syndrome, hypothyroidism, anemia, polycythemia vera, scleroderma, Darier disease, hypopituitarism, diabetes, neuropathy, peripheral arterial disease, gout, Raynaud's syndrome, sarcoidosis, psoriasis, alterations in the keratinization, cachexia, and iron deficiency were excluded. Patients who were using antimetabolites, gold, penicillamine, antiretrovirals or systemic retinoids were not included. The use of vitamin supplements, amino acids or any topical product for strengthening nails was suspended four weeks before the beginning of the study.
The hands of each patient were randomly assigned to two groups: one to Group A, and the other to Group B, implying that the patient was her own control.
- Group A
From Week 1 to Week 8: the fingernails of patients in Group A received an application of the CF in the evening, from Sunday to Wednesday. On Thursday, regardless of the time of the day, the patient applied the CF on all nails. Once it dried, the patient applied a coat of nail polish, which remained until Sunday evening.
From Week 9 to Week 16: the treatment with CF was suspended and the isolated use of the nail polish was maintained from Thursday to Sunday.
- Group B
From Week 1 to Week 8: no applications were carried out from Sunday to Wednesday. The patient applied nail polish on Thursday, removing it on Sunday.
From Week 9 to Week 16: the fingernails of patients in Group B began receiving the CF, as described for Group A.
The nail polish, as well as nail polish remover, were standardized for all patients and did not contain formaldehyde or acetone.
The objective of Phase 1 of the study (Week 1 to Week 8) was to assess the CF's efficacy. The objective of Phase 2 (Week 9 to Week 16) was to evaluate the maintenance of the results after the CF had been suspended for Group A. Due to an ethical issue, Group B received the CF between Week 9 and Week 16, in order that both hands were equally treated.
Quantitative score for the clinical evaluation of brittle nail
A quantitative score was created based on Van de Kerkhof et al. proposal. 1 This scale was used at each evaluation visit starting on the day of the patient's inclusion in the study.
The score assessed the onychoschizia, the onychorexis, and roughness for each of the nails and the hands in light of the main signs of BNS. Each nail received an individual score for these three parameters. The sum of the scores for the five fingers for each symptom resulted in three scores: onychoschizia (SDL), onychorexis (SO), and roughness (SR). The total score (TS) of the brittle nail for each hand was calculated as the sum of the three ratings for the symptoms (TS = SDL + SO + SR).
a. Onychoschizia
0 = absence of lamellar desquamation
1 = mild: lamellar desquamation that does not affect the entire free border of the nail
2 = moderate: lamellar desquamation affecting the entire free border of the nail plate
3 = severe: total compromise of the free border and up until one third of the nail plat
b. Onychorexis
0 = absence of signs of longitudinal ridges
1 = mild: one longitudinal ridge
2 = moderate: at least one deep longitudinal ridge
3 = severe: multiple superficial and deep longitudinal ridges
c. Roughness of the nail plate
0 = imperceptible elevations and longitudinal ridges
1 = mild: some flattened elevations and longitudinal ridges
2 = moderate: some prominent elevations and longitudinal ridges
3 = severe: more than 70% of the nail plate with protruding elevations and deep grooves
In order to assess the effectiveness of the treatment scheme, the percentage of patients with an improvement of at least 50% and 75% in the total clinical score (TS) for brittle nail and in the individual scores for each symptom (SDL, SO, SR) were analysed. Phase 2's main objective was to evaluate the maintenance of efficacy eight weeks after the completion of the use of the product, i.e. to compare the outcomes between Week 8 and Week 16 in Group A.
In the enrollment visit, the most affected nail (object-nail) of each hand was selected, and a cross-sectional sample of the free border was collected with the assistance of a nail plier. The same procedure was carried out in Week 8 and Week 16 with the same nail that was selected in the enrollment visit for each hand.
The samples were analyzed by conventional microscopy.
The nail samples were cut with a razor along the longer axis in order for the cut surfaces to be rectified, and were subsequently included as fresh tissue in paraffin blocks. Samples with 4µm were carried out and stained with hematoxylin-eosin. Histology was not used as a parameter to evaluate the effectiveness of the treatment, but to observe the main findings of the syndrome in the patients.
In Phase 1 of the study, the treatments were compared using ANOVA models (sources of variation: Group, week, patient, and interaction week versus patient). The residues' normality and homocedasticity were assessed using the Shapiro-Wilk test and a graph plot of predicted and residual values, respectively. Wilcoxon signed-rank nonparametric tests were performed for each week in the case of violations of the model's assumptions. Then, the proportion of patients with improvement in the score of at least 50% and 75% as compared to Week zero, was calculated for each week of the study. The comparison was performed using the McNemar test.
In Phase 2, in order to assess the continuing efficacy of the treatment, the results of Week 0, Week 8, and Week 16 were compared by ANOVA models or the Friedman test, in the case of violations of the normality of the model's residues. In a second step, the percentage of patients with improvement of at least 50% and 75% was compared between Weeks 8 and Week 16, using the McNemar test. Phase 2's analyses were carried out only for Group A.
Exploratory data analysis via frequencies, percentages, mean values and standard deviations were performed in order to evaluate the histological data, with graphs having been built for better visualization of the results.
The confidence level used in the analysis was 95%, and the software employed was the XLSTAT 2013.
The study included 38 female patients, whose hands were randomly distributed into Group A and Group B (38 hands each per group). Three patients did not complete the study, having denied the occurrence of adverse events when asked about their motives for leaving the follow up course. The mean age of the patients was 49 years (min = 33 years old, max = 63 years old). The results were analyzed according to the improvement achieved in each of the individual parameters (onychoschizia, onychorexis, and roughness) and the brittle nail total score.
Onychoschizia
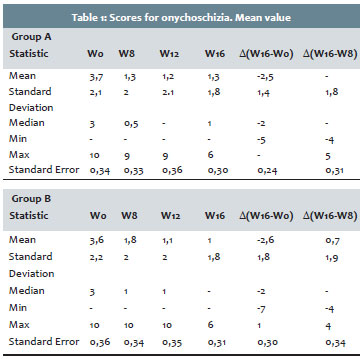
During Phase 1 of the study (Week 0 to Week 8), Group A had a mean value for onychoschizia that was significantly lower than that of the Group B (ANOVA, p = 0.004) (Table 1). The interaction between week and Group was not significant (p = 0.191), therefore, it was not necessary to compare the groups separately in each week.
During this phase, the proportion of patients with an improvement of at least 50% did not significantly differ between Groups A and B (McNemar's test, p-value W2 = 0.219, p-value W4 = 0.581 and p-value W8 = 0.180).
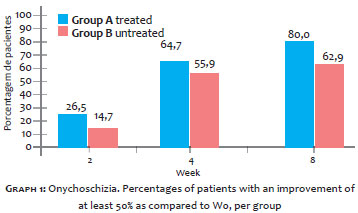
Although this difference was not statistically significant, it was possible to notice that the improvement for Group A was greater in all weeks evaluated. At Week 8, 80% (n = 28) of Group A's hands had clinical improvement greater than 50% for desquamation, as compared to 62.9% (n = 22) in Group B (Graph 1).
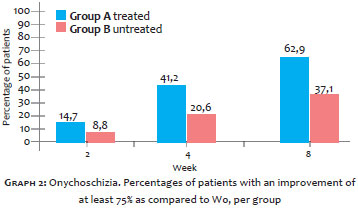
The proportion of patients with improvement of at least 75% was significantly higher in Group A (n = 22, 62.9%) when compared to Group B (n = 13, 37.1%) at Week 8, with a peak at Week 4 (McNemar's test, p-value S2 = 0.625, p-value S4 = 0.092, p-value S8 = 0.035) (Graph 2).
Significant differences were found between Week 0, Week 8, and Week 16 for Group A (ANOVA: p-value <0.001). During Phase 2 of the study (Week 9 to Week 16), Group A did not show a significantly different mean value for desquamation at Week 16 as compared to Week 8, while Week 8 and Week 16 had lower mean values than those of Week 0 (Table 1). These results evidenced the maintenance of the treatment's efficacy throughout the 16 weeks of the study.
The proportion of patients with improvement of at least 50% did not differ significantly between Week 8 and Week 16 (McNemar test, p = 0.688).
Onychorexis
There were no significant differences between Groups A and B at Weeks 2, 4, and 8 (Wilcoxon signed-rank; pW2 > 0.999, PW4 = 0.197, pW8 = 0.729).
As this symptom was virtually absent in the sample throughout the study, the percentage of patients with improvement of at least 50% or 75% as compared to Week zero was not calculated. Nevertheless, the percentage of patients with onychorexis did not increase during the study. The Phase 2 analyses were performed only for Group A. No significant differences were found between Week 0, Week 8 and Week 16 (Friedman; p-value = 0.607).
Roughness
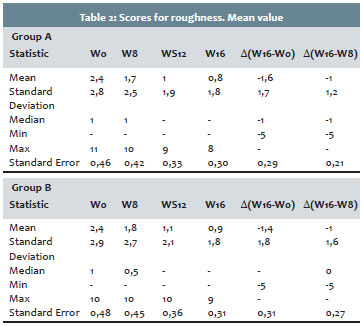
There were no significant differences between Groups A and B at Weeks 2, 4, and 8 (Wilcoxon signed-rank; p-value W2 > 0.999, p-value W4 = 0.856, p-value S8 = 0.309).
Fifteen hands (39.5%) had a score equal to zero from Week zero for Group A, and 16 hands (42.1%) for Group B, meaning that it was not possible to assess the improvement over time in such cases. For the remaining hands that had some degree of roughness, only 19 could be evaluated both to Group A and Group B, for Week 2 and Week 4; and only 18 for Week 8. The proportion of patients with an improvement of at least 50% did not differ significantly between groups (McNemar test, p-value W2 = 1.000, p-value W4 = 1.000 and p-value W2 = 1.000).
The proportion of patients with an improvement of at least 75% also did not differ significantly between groups (Mc-Nemar test, p-value W2 = 1.000, p-value W4 = 1.000 and p-value W2 = 1.000).
Significant differences were found between Week 0, Week 8, and Week16 for Group A (ANOVA; p-value> 0.001). A significant improvement in the score's mean value for roughness in Group A at Week 16 was found as compared to Week 0 and Week 8 (Table 2).
The proportion of patients with improvement of at least 50% did not differ significantly between Week 8 and Week 16 (z test for two proportions; p-value = 1.000). The total number of patients with evaluations for both groups in these weeks was 15.
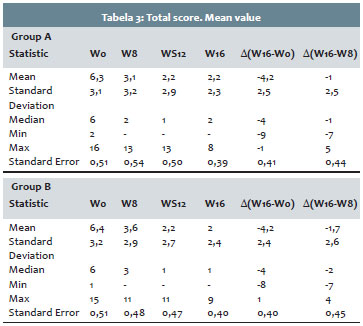
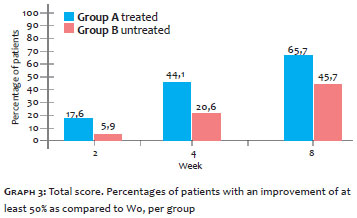
Total score
In the total score, Group A presented a mean value that was significantly lower than that of Group B over the eight weeks (ANOVA, p = 0.008) (Table 3). The proportion of patients with an improvement of at least 50% was significantly higher in Group A than in Group B at Week 4 (McNemar test, p-value W2 = 0.125; p-value W4 = 0.039 and p-value W8 = 0.167) (Graph 3). It is important to note that in Week 8 roughly 66% (23) of the patients showed a clinical improvement greater than 50% in the total score for Group A and 45.7% (16) for Group B.
The proportion of patients with an improvement of at least 75% was a majority in Group A as compared to Group B only at Week 8 (McNemar test, p-value W2 = 1.000; p-value W2 = 0.219 and p-value W8 = 0.77). Significant differences were found between Week 0, Week 8, and Week 16 for Group A (ANOVA; p-value > 0.001). The mean value for the total score in Group A was significantly lower at Week 16 when compared to Week 8 and Week 0. These results evidenced an even greater efficacy of the treatment over the 16 weeks of the study. The factor that contributed to the continued improvement from Week 8 was the improvement in roughness for both groups between Week 0 and Week 16.
The proportion of patients with an improvement of at least 50% did not differ significantly between Weeks 8 and Week 16 (McNemar test, p-value = 0.227). The total number of patients with evaluations for both groups in these weeks was 26.
Histological analyses
Histological evaluations were performed for the hand's object-nail (most affected) in both groups. The most examined nail was that of the first finger, followed by the fourth and second finger, respectively. The third and the fifth nails presented low percentages for both groups. All 38 participants were assessed for the subject-nail.
It was possible to observe that 81% and 90% of the object-nails in Group A and Group B, respectively, showed fragmentation of the nail plate. This finding varied very little in Week 8 and Week 16 for both groups.
Adverse Events
No adverse events were reported related to the product under investigation during the clinical study.
In the present study it was possible to observe that the most frequent symptom was the onychoschizia, found in all patients, followed by roughness, present in 60% of the sample. The presence of onychorexis was rare in this sample of patients, which is why the results were not conclusive in evaluating the product's effectiveness with this particular symptom. However, none of the patients with this event worsened during the study, while the prevalence of onychorexis in the sample remained stable. The most affected nail was that of the first finger, followed be the nails of the fourth and second fingers.
At present, the evaluation of BNS is clinical. Microscopic alterations described in the literature were observed by electron microscopy. However, this method is expensive and impractical. For this reason the authors decided to observe and describe the findings of conventional microscopy in the studied sample. Before the beginning of the treatment, nail fragmentation was observed in all samples through hematoxylin-eosin staining. The authors initially considered that this could clinically correspond to onychoschizia. However, despite the clinical improvement of onychoschizia, histological nail fragmentation did not change. One hypothesis is that this fragmentation could be caused by a technical device in the cutting of the blocks.
During the first eight weeks, there was significant improvement in onychoschizia and ungual roughness for both groups, for which the proportion of patients with improvement higher than 50% was similar. It is worth noting that before starting the study all patients used nail polish consistently and without interruption, but that during the study protocol nail polish was only applied from Thursday to Sunday. Thus, due to the fact that contact of the nail plate with aggravating agents such as acetone, formaldehyde and nail polish decreased, this had led to an improvement in the group that did not initially receive the CF. However, the reduction in the mean onychoschizia score and the proportion of patients with an improvement of at least 75% were significantly higher for the group treated with the CF in Phase 1 of the study.
In the second phase - in which there was an inversion of the groups - the good results obtained for onychoschizia in the first eight weeks for Group A were maintained through Week 16, despite the suspension of the CF application. As for roughness in Phase 2, Group A continued to improve. This improvement was more evident with the growth of the nail. These results indicated that the CF was more effective in treating onychoschizia and nail roughness than at only reducing the contact with aggressive agents with the nails, and its benefits were sustained after being discontinued. Regarding the total score for brittle nails, it was possible to observe from Week 4 that the proportion of patients with an improvement of at least 50% was statistically significantly higher for Group A, showing thus the CF's rapid onset of action. At Week 8 the proportion of patients with improvement of at least 75% was statistically superior to that of the group using CF when compared to the group that did not use the product. Between Week 8 and Week 16, the improvement in the total score for Group A continued even after the cessation of treatment. These results confirmed the CF's efficacy for the idiopathic BNS' symptoms, even when the frequency of application decreased to five days per week. The maintenance of benefits after cessation of use could be linked to the prolonged action of the product, as well as to the control exerted over aggressive agents (not using nail polish for some time, nail polish without formaldehyde, and nail polish remover without acetone).
Despite the fact that the ideal treatment for BNS with CF is a daily application for three months, the authors believe that the scheme proposed in this study may be an alternative posology for patients who do not want to stop using conventional cosmetic nail polishes. The maintenance of the benefits after the suspension of the CF observed in the present study suggests that the guidelines for the treatment should go along with those of pulse therapy, alternating treatment intervals of at least two months with a pause in treatment. Nevertheless, further studies are necessary in order to confirm what would be the ideal treatment period.
Figures 1 and 2 show the development of two patients during Phase 1 of the study.
In the group of patients involved in this study, the most common symptoms of BNS were onychoschizia and the ungualroughness. Changes in the nail care habits, the temporary suspension of the habit of applying nail polish, and the use of fewer aggravating products, without acetone and formaldehyde, led to the improvement of these symptoms. The alternative scheme of five CF applications per week was more effective for the control of BNS symptoms than just reducing the aggravating factors. It was not possible to evaluate the product's affect on onychorexis in the study's sample, due to the fact that that symptom was virtually absent.
The present study, therefore, allows for the proposal of an alternative scheme of CF use (five times a week) to reconcile the management of BNS with the habit of applying nail polishes.
1. Van de Kerkhof Peter, Pasch M, Scher RK, Kerscher M, Gieler U, Haneke E, et al. Brittle nail syndrome: a pathogenesis-based approach with a proposed grading system. J Am Acad Dermatol. 2005;53(4):644-51.
2. Iorizzo M, Pazzaglia M, Piraccini BM, Tullo S, Tosti A. Brittle nails. J Cosmet Dermatol. 2004;3(3):138-44.
3. Costa IMC, Souza- Carmo Nogueira L, Santiago Garcia P. Sindrome das unhas frágeis. An Bras Dermatol. 2007;82(3):263-7.
4. Garson JC, Baltenneck F, Leroy F, Riekel C, Müller M. Histological structure of human nail as studied by synchrotron x-ray microdiffraction. Cell Mol Biol. 2000;46(6):1025-34.
5. Shelley WB, Shelley ED. Onychoschizia: scanning electron microscopy. J Am Acad Dermatol. 1990;23(4):1127-32.
6. Colombo VE, Gerber F, Floersheim GL. Treatment of brittle fingernails and onychoschizia with biotin: scanning electron microscopy. J Am Acad Dermatol. 1990;23(6 Pt 1):1127-32.
7. Helmadach M, Thielitz A, Ropke EM, Gollnick H. Age and sex variation in lipid composition of human fingernail plates. Skin Pharmacol Appl Skin Physiol. 2000;13(2):111-9.
8. Brosche T, Dressler S, Platt D. Age- associated changes in integral cholesterol and cholesterol sulfate concentrations in human scalp hair and finger nail clippings. Aging (Milano). 2001;13(2):131-8.
9. Sherber N, Hoch A, Coppola RN, Carter EL, Chang HL, Barsanti FR, et al. Efficacy and safety study of tazarotene cream0,1% for the treatment of brittle nail syndrome. Cutis. 2011;87(2):96-103.
10. Haneke E. Onychocosmeceuticals. J Cosmet Dermatol. 2006;5(1):95-100.
11. Parcell S. Sulfur in human nutrition and applications in medicine. Altern Med Rev. 2002;7(1):22-44.
12. Sparavigna A, Setaro M, Genet M, Frisenda L. Equisetum arvense in a new transungual technology improves nail structure and appearance. J Plast Dermatol. 2006;2(1):31-8.
13. Monti D, Saccomani P, Chetoni P, Burgalassi S, Saettone MF, Mailland F. In vitro transungual permeation of ciclopirox from a hydroxypropyl chitosan-based, water-soluble nail lacquer. Drug Develop Indus Pharma. 2005;31(1):11-17.
This study was carried out at the Hospital Municipal do Servidor Público Municipal de São Paulo (HSPM) - São Paulo, Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}