


Maurício Pedreira Paixão
The lips are important anatomical units for perfect facial aesthetic balance. A number of methods can be used to improve lip appearance, including chemical and physical peels, botulinum toxin, cosmetic surgery and the use of cutaneous fillers. In the face of the already widespread and yet still growing use of fillers worldwide, the need for precise anatomical knowledge arises as an important tool to prevent complications. The objective of the present study is to shed light on the anatomical peculiarities of this facial topography and review recommendations linked to best practices with cutaneous fillings.
Keywords: ANATOMY; ESTHETICS; HYALURONIC ACID; LIP; LIP PRODUCTS
Lips are anatomical units of extreme aesthetic importance. Their contour and dimensions connote youth, sensuality, and beauty. Like the skin, they are subject to extrinsic and intrinsic factors that are responsible for aging.1, 2
There are several possible approaches for improving the aesthetic quality of the lips, predominantly chemical and physical peelings, which in the latter category includes ablative or non-ablative lasers, mechanical abrasions, botulinum toxin, and different surgical techniques-all examples of treatment modalities.2
This paper will focus on the cutaneous filling technique as a resource to improve the aesthetics of this area. A fundamental prerequisite for its appropriate use is the knowledge of lip anatomy - a determining factor for the correct implementation of this invasive procedure.3
Complications from the use of fillers include ecchymosis, edema, erythema, infections, herpes reactivation, nodules, granulomas and those resulting from vascular damage, which include bleeding, necrosis and embolization - complications that are very relevant to the topic discussed.4
The objective of the present paper is to provide essential information regarding the labial arterial supply, including recommendations to minimize these potential acute complications.
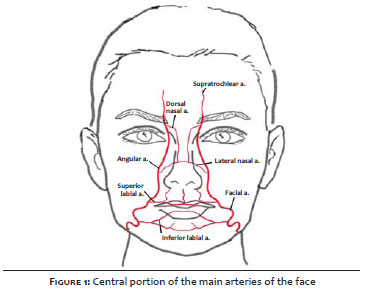
Figure 1 shows the arterial supply of the lips, including its relationship with the major vessels of the central portion of the face. The facial vessels constitute a wide vascular network. Damage caused in a particular artery can be compensated by its contralateral pair and/or anastomoses.3
Upper lip
The arteries responsible for the arterial blood supply of the lips originate in the facial artery (FA). The main artery of the upper lip is the superior labial artery (SLA), and its subalar (SAA) and septal (SA) branches are sometimes additional to this process.5
According to Al-Hoqail et al.,3 Crouzet et al.6 and Ricbourg, 7 based on the dissection of cadavers fixed in formalin, in most cases the SLA originates above the labial commissure and in fewer than 25% of cases its origin coincides with it (Figure 1). Tansatit et al. 5 determined that the distance from the SLA's origin to the labial commissure ranges from 5-9 mm.
Regarding the diameter of the SLA, Park et al. 8 identified a diameter of 1.2 mm at its origin, while Crouzet et al. 6 identified an average diameter of 1.0 mm and Magden et al.9 1.3 mm. Al Hoqail et al. 3 found an average diameter of 1.8 mm and Pinar et al.10, 1.6 mm. Tansatit et al. 5 came to a value of 1.1 + 0.3 mm.
Although the labial artery is commonly bilateral, it varies widely according to the pattern in the dominant side, tortuosity, and path. Interestingly, Al-Hoqail et al. 3 and Magden et al.9 demonstrated the unilateral existence of the SLA in 36% of cases and Tansatit et al.5 in 23% of cases.
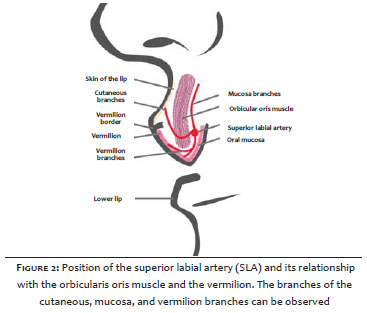
Figure 2 shows that the SLA is located posteriorly to the orbicular oris muscle, emitting perforating branches to reach the skin. Furthermore, branches reaching the vermillion and the oral mucosa are also identified. The SLA is located at an average depth of 4.5 mm in the skin, at 2.6 mm from the mouth, and 5.6 mm from the inferior border of the upper lip. 5 Given the anatomical peculiarities, the arterial supply of the philtrum's portion in the upper lip will be analyzed in the next section.
Philtrum
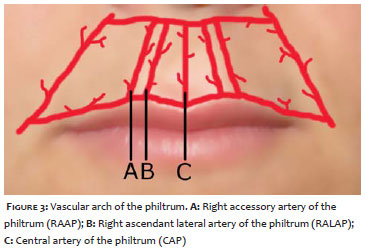
Figure 3 shows the philtrum's arterial supply, carried out by the arch formed by the central artery of the philtrum (CAP), the left and right lateral ascendant arteries of the philtrum (LLAAP and RLAAP, respectively) and the left and right accessory arteries of the philtrum (LAAP and RAAP, respectively).
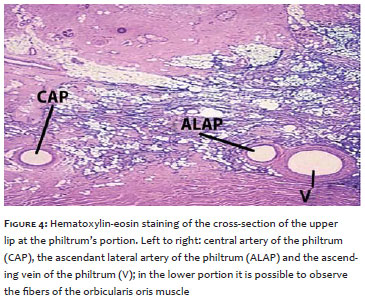
The anatomical study conducted in cadavers by Garcia de Mitchell et al. demonstrated the existence of a fat compartment superficial to the orbicularis oris muscle. In addition, it is important to note that the arteries that make up this arch in the philtrum are located above the orbicularis oris muscle (Figure 4).11
Lower lip
The lower lip is supplied by the FAs, the inferior labial artery (ILA) and the labiomentonian artery (LMA). The LMA may have horizontal branches (called the horizontal labial artery - HLA), and vertical branches (called vertical labial artery -VLA). With a role similar to that played by the SLA, the ILA is primarily responsible for the lower lip's arterial supply. Although there is a dominance of the VLA over the HLA, there is an alternating pattern in the HLA and VLA.3
Many anatomy textbooks and researchers have described the ILA as originating at the level of the labial commissure.3 However, Al-Hoqail et al.3 identified its origin below the labial commissure in 42.9% of cases, at the commissure level in 35.7% of cases, and above the commissure in 21.4% of cases. In addition, its origin in a branch shared with the SLA occurred in 28.6%, while Tansatit et al. 5 identified this pattern in 11.5% of the cases (Kawai's type B).
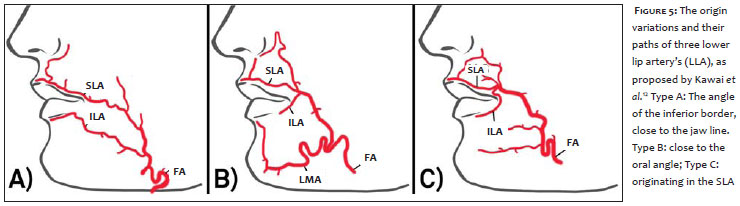
By studying the origin of the ILA, Kawai et al. 12 demonstrated the existence of three patterns: Type A) originally described as the most common (Figure 5). On the other hand, Al-Hoqail et al. 3 demonstrated Type B (42.9%) as the most common type, followed by Type A (35.7%) and Type C (21.4%), respectively. Other origin and path patterns for the ILA were described by Al-Hoqail et al. 3
In turn, Tansatit et al.5 found that the ILA more commonly originates in the FA, forming common branch with the LMA. In 30.8% of cadavers, the FA sends another small transverse branch of the LMA - from one or both sides - before the formation of the main branch. Pinar et al. 10 and Tansatit et al. 5 found a diameter of roughly 1.3 mm for the ILA.
General
Lazzeri et al. 13 provide important general recommendations for the use of cutaneous filling substances:
Prefer using micro cannulas with blunt tips in areas where there is a greater chance of arterial damage, in order to prevent direct injection into the vessel with a conventional needle. Move the blunt tip micro cannula gently in order to avoid tearing and to stimulate temporary vasoconstriction of the vessels. Choose needles/micro cannulas of a smaller caliber, for although greater initial pressure is necessary to inject the product, this choice favors a lower injection speed and reduces the likelihood of vascular occlusion or blockage of the peripheral flow. In order to facilitate the insertion of the cannula, a subcision or pre-tunneling can be performed using an 18G needle. This is safer than carrying out the dissection procedure with the filler substance itself. Aspirate before injecting the product in order to verify that the needle/micro cannula is not inserted in an artery or vein. Avoid the path of a large caliber (>0.5 mm) artery; alternatively use a 25G cannula parallel to that artery in order to minimize the risk of accidental vascular perforation. Inject only small volumes at a time, thereby decreasing the damage, because if a plunger occurs, it will most likely be subclinical. Avoid injection of large volumes in less distensible planes, thereby preventing high pressure locally. To carry out an anesthetic block and/or topical anesthesia promotes arterial vasoconstriction. This is potentially beneficial due to the fact that it minimizes the risk of perforation or cannulization, which occurs more often in vasodilated arteries. Avoid performing the filling procedure associated with other procedures, such as rhytidoplasty and liposuction in the same site, for the risk is higher in tissues that have previously been traumatized.
DeJoseph4 also offers the following suggestions:
The fingers of the hand that is not being used to inject must be employed to stabilize the skin and assist the progression of the cannula. Less massage is necessary when the filling substance is injected deeply into the tissues.
Recommendations specific to the lips
Tansatit et al. 5 bring contributions to the use of filler to the region of the lips:
The injection of lips at a depth greater than 3 mm beneath the vermilion can be deemed safe for the projection of the lips. The vermilion's border is a safe area for creating the "cupid's bow" with 30G microcannulas or 27G needles. An injection that is carried out in deeper planes using 27G microcannula, being inserted longitudinally in the middle of the lip with an aim at increasing its volume, can be deemed safe, for the SLA is not usually located in the more central portion of the lip. Compression of the SLA at about 1 cm above the oral commissure, a point at which it passes near the oral angle, is recommended. Injection in the border of the lower lip is safer. The ILA's path runs close to the alveolar border, outside the lower lip's vermilion. Most labial branches cross into the vermilion perpendicularly, and the marginal arteries that connect with these terminal branches in the vermilion are of a very small caliber. In about only 4% of cases the ILA assumes an aberrant path, running more superiorly and much closer to the vermilion.
For a better understanding of the practical parameters, such as the pressure exerted on the syringe's plunger, the effect of the caliber of the microcannula's/needle's length and the product's viscosity, it is important to briefly discuss the dynamics of fluids.
Through the contributions of outstanding researchers, such as Bernoulli and Darcy-Weisback, a behavioral equation was formulated for an ideal incompressible fluid in linear flow (in the absence of turbulence and/or vortices) in a circular pipe.14 In the present paper, the fluid being analyzed is the cutaneous filling substance.
P = f x (L / D) x (V2 / 2g), where:
P = pressure exerted in the syringe,
f = Darcy-Weisbach's friction factor,
L = pipe's length,
D = pipe's diameter,
V = fluid's speed within the pipe (m/s), and
g = local acceleration due to gravity.
The equation shows that the diameter of the needle/ microcannula and the syringe has a direct effect on the amount of pressure required to promote the filler's flow. It also shows that greater pressure is needed to make the filler flow through a smaller caliber and for longer distances.
In addition, the friction factor is closely related to viscosity. The denser the filler the greater the pressure gradient required in order for it to flow. The use of Darcy-Weisback's equation allows the immediate understanding of important variables applied to the cutaneous filling technique.
The literature describes the considerably intuitive fact that the injected volume directly influences the severity of vascular occlusion.5 Other factors are also determining: The artery's diameter, the degree of vasoconstriction, the applied pressure gradient, the blood flow through the anastomotic network (toward the eyes or the mouth), and the size of the puncture made in the artery's wall (in the absence of direct channeling via the needle) are hemodynamic conditions that influence the degree of vascular occlusion. There are a variety of filling techniques: serial and linear punctures, injections in deposit or in layers, and their variants.15 Since they influence the manner and the amount of injected product, as well as the tissular damage in the filled region, it is reasonable to consider the role of these techniques in the occlusion process.
As a part of the aging process--which is aggravated by the effects of gravity--there is a widening of the cutaneous portion of the upper lip (an increase in distance between the nasal base and mucocutaneous transition line) and a decrease in its thickness. Furthermore, the process includes philtrum deletion, reversal of the vermilion, an obstructed view of the incisor teeth during major facial incursions, and a horizontal flattening of the vermilion. Perioral wrinkles arise concomitantly.2
In 2008, according to data from the American Society of Plastic Surgery, 1.26 million treatments with hyaluronic acid were performed, 123,000 with apatite hydroxide, 58,000 with collagen, and about 32,000 with poly-L lactic acid. It is believed that these statistics are underestimated, as a result of the fact that only dermatologists, plastic surgeons, and otolaryngologists with recognized qualifications were included.16
The widespread use of these techniques, combined with potential complications due to poor practice, justifies the need for prior in-depth knowledge of the anatomy of the area to be treated. Such conduct is expected in order to prevent serious diseases, including acute vascular occlusion.
The anatomical focus of this lip's topography has other implications, even for surgical planning, transcending its purpose related to the best use of fillers. For example, the recognition of the possibility of anatomical variation of the SLA, with unilateral origin, has a predictive value for the survival of single-pedicled axial flaps, such as the Estlander, McGregor, and Abbe among others, widely used in the treatment of lip carcinomas.3
The wide variety of anatomical presentations revealed by the various studies carried out with cadavers have shown that the vessels of the labial region have numerous individual configurations. Alterations in the diameter, path, dominance, and symmetry were found in a series of analyses of cadavers.3, 5, 6, 9, 10 It is important to recognize the relevance of the data contained in the basic sources of anatomy for the advancement of learning. Nevertheless, given its impact on daily practice, it becomes impossible to disregard these relevant anatomical variations.
Avoiding intersections with the path of the lip's vessels is of great importance.5 Regarding the ILA, the recognition of the types proposed by Kawai et al. 12 allows for the best choice for the site of the needle's/microcannula's insertion, as well as the identification of its possible path (Figure 5). Although with less apparent variations, such reasoning also applies to the SLA in the upper lip.
Another anatomical peculiarity mentioned is in regards to the region of the philtrum. The understanding of the philtrum's anatomy is valuable, since this area is subject to many cosmetic procedures, such as cutaneous filling. It is possible to observe that this region's arteries are superficial to the orbicularis oris muscle, in a symmetrically opposite location regarding the SLA (Figure 4).11 This superficial layout explains the common occurrence of bleeding verified when performing a filling of the philtrum's pillars.
In fact, it is believed that alterations resulting from angiogenesis in the philtrum have participation as a causal or predisposing factor of congenital lip defects, including the cleft lip.11
Regarding complications, the formation of a centralized database containing essential information, such as topography, product type, injected volume per region, complications observed, and duration and reversibility of complications would be of great statistical value. Medical specialty societies could promote such an initiative, encouraging the dissemination of statistical results obtained from their analysis, which would guide professionals to act based on the best evidence of these complications.
The damage or vascular occlusion caused by fillers is rare, however it can be poorly reported or not recognized, which interferes with an accurate reporting of its prevalence. 4 This reinforces the recommended creation of the database. Diagnosis and early management are challenging. The vascular injection occurs when the filling substance causes the vessel's occlusion. Another possible form of vascular occlusion results from the increased external pressure exerted by the volume of the filling substance, paralyzing the blood flow. Such occlusion can be arterial or venous, with the first being described as being associated with sudden and intense pain, leaving the skin pale or purplish in color. Another possibility is induced and persistent vasospasm.4, 17
It is worth noting that the diameter of the main arteries in the lips is large enough to allow the implementation of microsurgical anastomoses.3 Their dimensions can be greater than that of the diameter of the needles/microcannulas, making intra-arterial injections physically feasible. Regarding the microcannulas, it is interesting to note that, if on the one hand a 25G cannula allows for the injection of a greater quantity of the substance in bolus, on the other hand its larger caliber implies a lesser risk of causing a perforation in the arterial wall when compared to a thinner cannula, such as 30G.5
The embolization of the retinal artery causes blindness.13, 17 In a review of cases of blindness, fat was the most commonly used type of filling substance, and in fact, occurred when the filling procedure was carried out in the lower third of the face. A case of temporary loss of visual acuity was described with the use of corticosteroid in the scalp for the treatment of alopecia areata, and other cases of blindness linked to the use of intranasal injections and in angiomas. That study did not conclude that blindness resulted from the use of artificial fillers used only in the lip region - however it should be noted that, despite this conclusion, it does not mean that it cannot happen. Finally, the authors warn about the threat of such a situation and the high probability of permanent sequel, even when all necessary measures are taken.13, 17
Although they did not provide a mathematical exemplification, Lazzeri et al.13 found that a shorter distance from the retinal artery's origin implied a greater risk of blindness. This correlation can be easily verified by the Darcy-Weisbach's equation, which shows that less pressure is needed when the vessel's length is shorter, unfortunately making the occurrence of this condition easier. It is also important to note that the degree of exerted pressure can be intense to the point of promoting the retrograde flow of the filler up to the internal carotid, a point at which cerebral embolization would take place. This represents a situation with even more serious consequences, and whose symptoms will depend on the involved area of cerebral ischemia.17, 18
Finally, despite the great diversity of filling techniques, there is no consensus on which would be the best one.19 It is also worth noting that there is no consensus among experts regarding this matter or as to the type of product to be injected into a specific region. 20 In consideration of this, well-conducted, prospective studies would be valuable for elucidating these issues.
1. Philipp-Dormston WG, Hilton S, Nathan M. A prospective, open-label, multicenter, observational, postmarket study of the use of a 15 mg/mL hyaluronic acid dermal filler in the lips. J Cosmet Dermatol. 2014;13(2):125-34.
2. Paixão MP, Montedonio J, Queiroz Filho W, Pouza CET, Almeida AEF. Lifting de lábio superior associado à dermabrasão mecânica. Surg Cosmet Dermatol. 2011;3(3):249-53.
3. Al-Hoqail RA, Meguid EM. Anatomic dissection of the arterial supply of the lips: an anatomical and analytical approach. J Craniofac Surg. 2008;19:785-94.
4. DeJoseph LM. Cannulas for facial filler placement. Facial Plast Surg Clin North Am. 2012;20(2):215-20, vi-vii.
5. Tansatit T, Apinuntrum P, Phetudom T. A typical pattern of the labial arteries with implication for lip augmentation with injectable fillers. Aesthetic Plast Surg. 2014;38(6):1083-9.
6. Crouzet C, Fournier H, Papon X, Hentati N, Cronier P, Mercier P. Anatomy of the arterial vascularization of the lips. Surg Radiol Anat. 1998;20(4):273-8.
7. Ricbourg B. Blood supply of the lips. Ann Chir Plast Esthet. 2002;47(5):346-56.
8. Park C, Lineaweaver WC, Buncke HJ. New perioral arterial flaps: anatomic study in clinical application. Plast Reconstr Surg. 1994;94(2):268-76.
9. Magden O O, Edizer M, Atabey A, Tayfur V, Ergür I. Cadaveric study of the arterial anatomy of the upper lip. Plast Reconstr Surg. 2004;114(2):355-9.
10. Pinar YA, Bilge O, Govsa F. Anatomic study of the blood supply of perioral region. Clin Anat. 2005;18(5):330-9.
11. Garcia de Mitchell CA, Pessa JE, Schaverien MV, Rohrich RJ. The philtrum: anatomical observations from a new perspective. Plast Reconstr Surg. 2008;122(6):1756-60.
12. Kawai K, Imanishi N, Nakajima H, Aiso S, Kakibuchi M, Hosokawa K. Arterial anatomy of the lower lip. Scand J Plast Reconstr Surg Hand Surg. 2004;38(3):135-9.
13. Lazzeri D, Agostini T, Figus M, Nardi M, Pantaloni M, Lazzeri S. Blindness following cosmetic injections of the face. Plast Reconstr Surg. 2012;129(4):995-1012.
14. Sanks RL. Flow in Conduits. In: Jones GM, Bosserman BE, Sanks RL, Tchobanoglous G, editors. Pumping Station Design. Burlington, USA: Elsevier; 2008. p. 3.5-6.
15. Bartus CL, Sattler G, Hanke CW. The tower technique: a novel technique for the injection of hyaluronic acid fillers. J Drugs Dermatol. 2011;10:1277-80.
16. Montedonio J, Queiroz Filho W, Pousa, CE, Paixão MP, Almeida AEF. Fundamentos da ritidoplastia. Surg Cosmet Dermatol. 2010;2(4):305-14.
17. Weinberg MJ, Solish N. Complications of hyaluronic acid fillers. Facial Plast Surg. 2009;25(5):324-8.
18. Danesh-Meyer HV, Savino PJ, Sergott RC. Case reports and small case series: Ocular and cerebral ischemia following facial injection of autologous fat. Arch Ophthalmol. 2001;119(5):777-8.
19. Thomas MK, Dsilva JA, Borole AJ, Naik SM, Sarkar SG. Anatomic and mechanical considerations in restoring volume of the face with use of hyaluronic acid fillers with a novel layered technique. Indian J Plast Surg. 2014;47(1):43-9.
20. Lee SK, Kim HS. Recent trend in the choice of fillers and injection techniques in Asia: a questionnaire study based on expert opinion. J Drugs Dermatol. 2014;13(1):24-31.
This study was carried out at a private practice in São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}