


Flávia Estrela Maroja Marinho1; Marcela Duarte Benez Miller2; Fátima Satomi Nishimori1; Pedro Etienne Arreguy Rodrigues Silva1; Maria Shirlei Chaves Loureiro do Carmo3
Keywords: CARCINOMA, BASAL CELL; RECONSTRUCTIVE SURGICAL PROCEDURES; NOSE NEOPLASMS; SURGICAL FLAPS.
The basal cell carcinoma (BCC) is primarily located in areas exposed to sunlight and is the most common type of skin cancer. It can result in significant morbidity if not completely excised.1 On the other hand, nasal skin defects are challenging for surgeons due to reconstruction requirements, and the fact that color irregularity, texture, and skin thickness are all easily visible.2, 3 The integrity of the aesthetic subunits of the nose (tip, dorsum, soft triangle, columella and lateral walls) is critical to maintaining the harmony of facial features4. In the dorsum of the nose, studies show good aesthetic and functional results using the Rieger's flap.4-6
A 71-year-old male patient (a retired electrician), skin type I, with a history of sun exposure and prior excision of multiple BCCs sought care at the dermatologic service. On clinical examination, it was possible to observe a nodule of approximately 2 cm in diameter on the nose, which had been in development for about 2 years (Figure 1).
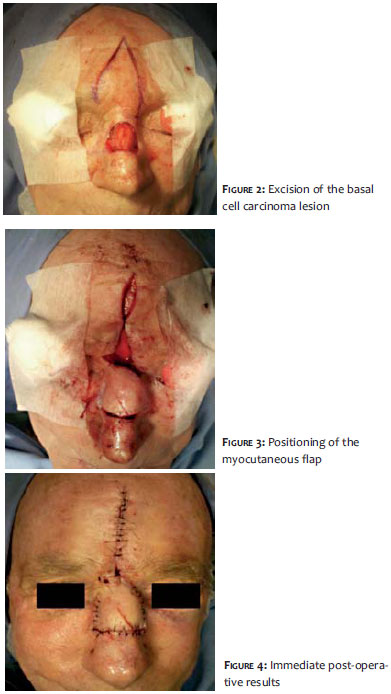
Using dermoscopy it was possible to view arboriform telangiectasias crossing the lesion and an absence of pigment. The histology of an incisional biopsy revealed nodular BCC. A decision was then made for surgical treatment under local anesthesia, excision of the lesion with an initial margin of 4 mm and intraoperative control of margins by a pathologist. After the evaluation of surgical margins that were free of neoplasia, the reconstruction of the nasal dorsum was carried out with the Rieger's flap (Figures 2 to 4). Post-operative care included: placement of drain, pressure dressing, and oral antibiotics therapy with cephalexin. The removal of the drain, the cleansing of the surgical wound and the application of a dressing with sterile micropored adhesive plaster were carried out on the following day.
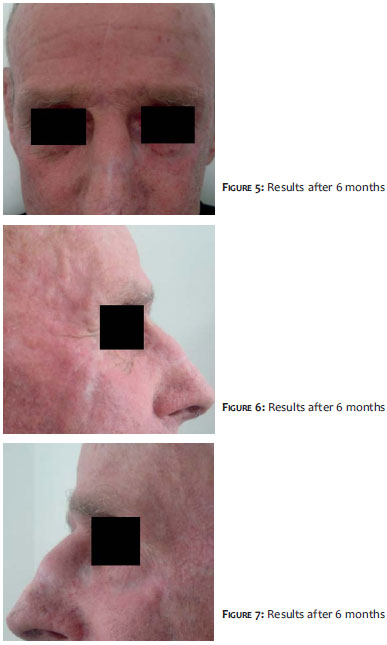
After seven days, the stitches began to be removed alternately. All stitches were removed within 2 weeks. The patient was followed up with for 10 months and, up until the time the present paper was submitted, no clinical or dermoscopic recurrence of the lesion had taken place (Figures 5-7). Furthermore, a good aesthetic outcome was achieved.
Nodular BCC can reach great dimensions and may deepen, causing considerable tissue damage. The nose is the most characteristic feature of the face and any change in its shape, color, or skin becomes obvious. Thus, the surgeon must choose the reconstruction method that provides the best possible aesthetic result.4,6
The Rieger's flap was described by its eponym in 1967, as a good option for reconstruction of defects in the nasal tip of up to 2 cm in diameter.4,5 Since then, it has been described in the literature with slight variations and multiple new nomenclatures, such as glabellar flap, extended glabellar flap and dorsal nasal flap.2,3 It is a rotation/advancement flap used for defects in the middle and lower third of the nose. It resembles a rhomboid flap that takes advantage of the glabellar excess skin, making it especially suitable for elderly patients.5
The skin is incised from the lateral portion of the defect, running through the nasofacial fold to reach the glabellar region. The incision is subsequently drawn down along the contralateral side up to the eyebrow region. The flap should be musculocutaneous. After proper detachment, the flap is rotated/advanced inferiorly, and the glabellar defect sutured primarily.5
The authors chose this flap due to the fact that the patient was elderly and had excess tissue in the donor area. Despite the tumor's extent and location, the use of this flap allowed the excision of the entire lesion with a sufficient safety margin, and made it possible to maintain the harmony of the nasal unit.
1. Rigel DS, Cockerell CJ, Carucci J, Wharton J. Queratose actínica, Carcinoma Basocelular e Carcinoma Espinocelular. In: Bolognia JL, Jorizzo JL, Rapini RP. 2ª. Ed. Dermatologia. Rio de Janeiro: Elsevier, 2011. p. 1641-59.
2. Jackson IT. Reconstrução do Nariz. In: Retalhos Locais na Reconstrução de Cabeça e Pescoço. Rio de Janeiro: DiLivros; 2002.
3. Baker SR. Retalhos Locais em Reconstrução Facial. 2ª. ed. Rio de Janeiro: DiLivros; 2009.
4. Severo Jr LCV, Chambô F, Dibe MJA, Leal PRA. Retalho miocutâneo dorsoglabelar baseado na artéria nasal lateral para reconstrução de defeitos da ponta nasal. Arq Catarinenses de Med. 2007;36(1):124.
5. Valiati AA, Pereira Filho GA, Cunha TF, Minuzzi Filho ACS, E PB. Retalho de Rieger: resultados estéticos e satisfação dos pacientes. Rev Bras Cir Plást. 2011;26(2):250-3.
6. Laitano FF, Teixeira LF, Siqueira EJ, Alvarez GS, Martins PDE, Oliveira MP. Uso de retalho cutâneo para reconstrução nasal após ressecção neoplásica. Rev Bras Cir Plást. 2012;27(2):217-22.
This study was conducted at the Hospital Federal da Lagoa - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}