


Renan Minotto1; Liliam Dalla Corte2; Ana Letícia Boff3; Mariana Vale Scribel da Silva2; Marina Resener de Morais4
Keywords: NAILS; KERATOACANTHOMA; FINGER FALANGES.
Keratoacanthoma, when located in the nail unit, is an unusual and destructive form of this neoplasm, which can develop in the nail bed or in the proximal nail fold. In contrast to other keratoacanthomas, spontaneous regression is rare. The presence of this tumor type in the nail apparatus region is problematic, due to the location, the therapeutic choice, and the possibility of recurrence after local excision.1 In this topography, the tumor may present variations when compared to other locations, being classically represented by a nodular, painful endoexophytic lesion with a crateriform area filled with keratin. Histological confirmation of the case is necessary. Therapy should be based on clinical, radiological, and histological correlation.2
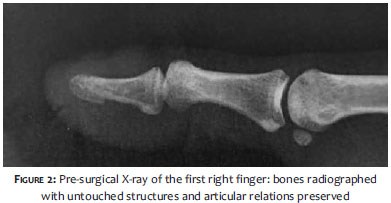
A 60-year-old Caucasian male patient reported the onset of changes in the right index finger two years earlier, which had been subsequently treated as onychomycosis without success. The lesion continued to grow. On clinical examination, he presented nail dystrophy with plate destruction and exposure of the nail bed's lesion (Figure 1), areas with waxy texture to the touch, and surrounded by hardened keratinized tissue and edema of the finger. The initial diagnostic impressions included squamous cell carcinoma, keratoacanthoma, and amelanotic melanoma. The X-ray of the affected area showed swelling of the soft tissues, but nevertheless did not reveal osteoarticular abnormalities, suggesting the presence of a (probably) non-compressive superficial lesion (Figure 2). Direct and cultural mycological tests came out negative. A decision was then made to do a wedge biopsy for the removal of a representative specimen of the lesion. The histological examination confirmed the keratoacanthoma diagnosis (Figure 3). In the face of this result, the authors indicated the surgical excision with complete avulsion of the nail plate and removal of the tumor - which encompassed the bed and proximal nail fold, up until the plane close to the bone - and healing by secondary intention. The histological examination of the specimen has confirmed the presence of a keratoacanthoma with free margins, leading to a recommendation of the total removal of the tumor. In the post-excisional follow-up of the lesion, there was no evidence of recurrence in the late postoperative period.
The keratoacanthoma involving the nail and periungual tissue is a keratinocyte neoplasm that is rarely found at these body sites. It has a destructive development and sometimes affects the underlying bone structures through tumor compression. It is a rare and aggressive variant of the classic keratoacanthoma, and tends to appear on the first three fingers - particularly on the index finger - however it can also occur on the toes. The tumor usually occurs in middle aged Caucasian men. It can be solitary, multiple, eruptive or familiar.1, 2, 3 The clinical picture differs from that of the traditional keratoacanthoma, for in the subungual form there is usually pain, early and fast growth, and underlying bone compression. On clinical examination it presents as a verrucous or hyperkeratotic nodule in the nail bed, along the distal edge of the nail, often in association with partial onycholysis. In the proximal portion of the subungual tissue, the tumor can arise as a lesion similar to paronychia. In contrast to keratoacanthoma that occurs at other body sites, spontaneous regression is rare. The differential diagnosis of a painful and nodular lesion in the distal phalanx includes: dermoid cyst, common wart, subungual exostosis, amelanotic melanoma, squamous cell carcinoma, and subungual keratoacanthoma.1, 2 Due to its fast growth, the digital keratocanthoma often causes erosion or bone compression. The radiological finding is a cup-shaped defect in the terminal phalanx. The bone damage usually resolves after tumor excision.1, 2 Subungual keratoacanthomas tend to have less inflammation and increased invasion in deeper planes, and can be present in cases of pigmentary incontinence such as with Bloch-Sulzberger syndrome.3, 4
The histopathology is similar to that of the keratoacanthoma that occurs in other areas, typically revealing parakeratosis and epidermal hyperkeratosis with the center filled with keratin.1 On the other hand, the digital keratoacanthoma's typical characteristics include: vertical orientation, presence of many dyskeratotic cells, scarce eosinophils and neutrophils in the epithelium, and reduced fibrosis in its base. It is important to differentiate the keratoacanthoma from the squamous cell carcinoma in order to allow for a better therapeutic choice and assessment of prognosis. Both can clinically present pain, inflammation, or destruction of the distal phalanx.1, 2, 4, 5 Radiologically, the subungual keratoacanthoma is almost indistinguishable from the subungual squamous cell carcinoma. Nonetheless, keratoacanthoma causes a lesion in the distal phalanx that has well-defined borders and grows but does not penetrate the bone. Furthermore, the keratoacanthoma usually occurs in patient's in their 50's, whereas the squamous cell carcinoma usually occurs in patient's in their 70's and is slower growing.1-3, 5 Curettage and local excision are indicated by many authors as the initial treatment of choice for digital keratoacanthoma. 6 Recurrences, however, are common and are probably related to the tumor's tendency for deeper planes of invasion and close connection to underlying bone structures. Due to its ability to correctly define tumor margins, Mohs surgery can help in reducing recurrences and thus avoid involvement of the fingertip. Amputations have been reported in cases of multiple recurrences, extensive bone destruction, or where the differentiation from squamous cell carcinoma is difficult. Other treatments with non-surgical procedures have been used in specific cases with varying results.1, 2 The present case exhibited aspects – such as the lack of an initial diagnosis, the fact that it was treated as onychomycosis, and that there was a necessity to carry out a biopsy (as in cases of tumor lesions in the nail apparatus) – that drew the authors' attention.
1. Cecchi R, Troiano M, Buralli L, Innocenti, S. Recurrent distal digital keratoacanthoma of the periungual region treated with Mohs micrographic surgery. Australas J Dermatol. 2012;53(1):e5-7.
2. González-Rodríguez AJ, Gutiérrez-Paredes EM, Montesinos-Villaescusa E, Burgués Gasión O, Jordá-Cuevas E. Queratoacantoma digital distal: importancia del diagnóstico diferencial con el carcinoma escamoso subungueal. Actas Dermosifiliogr. 2012;103(6):549-51.
3. Underhill T. Subungual keratoacanthoma: the importance of accurate diagnosis. J Hand Surg Eur Vol. 2010;35(7):599-600.
4. Connolly M, Narayan S, Oxley J, Berker DAR. Immunohistochemical staining for the differentiation of subungual keratoacanthoma from subungual squamous cell carcinoma. Clin Exp Dermatol. 2008;33(5):625-8.
5. André J, Richard B. Subungueal keratoacanthoma. Ann Dermatolol Venereol. 2012;139(1):68-72.
6. Pellegrini VD Jr, Tompkins A. Management of subungueal keratoacanthoma. J Hand Surg Am. 1986;11(5):718-24.
This study was performed at the Hospital Santa Casa de Misericórdia de Porto Alegre - Porto Alegre (RS), Brazil.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}