


Frederico Hassin Sanchez1; Eduardo Lerner2
Keywords: MOHS SURGERY; CARCINOMA, BASAL CELL; CARCINOMA, SQUAMOUS CELL; EYELID NEOPLASMS; ORBIT EVISCERATION.
The periocular region is often affected by malignant skin tumors, with basal cell carcinoma (BCC) being the most frequent, followed by squamous cell carcinoma (SCC), and less commonly by sebaceous carcinoma (SC) and Merkel cell carcinoma. Basal cell carcinoma is responsible for 80-90% of all malignant neoplasms of the eyelids.1 It mainly affects the lower eyelid (50-60%), followed by the medial canthal region (25-30%), and to a lesser extent by the upper eyelid and lateral canthal region.1,2 In the literature, the mortality rate is variable, estimated at 1.5 to 11%,3,4 and in general is precipitated by intracranial invasion. Tumors involving the medial canthal region are correlated to an increased risk of intraorbital and intracranial invasion.1, 2
Although less common, SCC has a more aggressive biological behavior due to its metastatic potential. It is estimated that there is a 24% risk of metastasis to regional lymph nodes secondary to palpebral SCC, and an 8% risk of perineural invasion.1, 2, 5
Perineural invasion can result in a worse prognosis, due to an increased risk of orbital invasion, and an increased recurrence rate. Intermittent or continuous pain, and prickling are symptoms that are often associated with perineural invasion.1, 5
Sebaceous carcinoma is often undertreated, due to the fact that it often mimics benign diseases such as blepharoconjunctivitis or chalazion. It can simulate a BCC or a SCC, and has great potential to metastasize and be lethal. 5, 6 It originates in the meibomian glands in the tarsal plate, or in the Zeiss glands, which are related to the eyelashes. It is more frequent in the upper eyelid, but may cause multifocal lesions, with an estimated orbital invasion of around 15-19% of cases. Metastases can occur in 17% of cases, and mortality is estimated at 6%.5, 6
Although rare, Merkel cell carcinoma may arise on the eyelids. It has great lethality, grows rapidly, and primarily affects elderly female patients. Metastases may occur early, having a negative affect on the prognosis for recovery. Other malignant neoplasms in this region are even rarer.1, 5
The surface anatomy of the periocular region classically comprises four anatomical subunits: upper eyelid, lower eyelid, lateral canthal region, and medial canthal region.2
Periocular tumors constitute a challenge to the dermatologic surgeon who, while minimizing the functional impairment of the eyelids,7 should pay attention to the fact that this region is located over the embryonic cleft area, and is therefore less resistant to tumoral spread.1, 8, 9 The risk of orbital invasion is greater with biologically aggressive tumors, such as SC and SCC. Although rare in occurrence, it is estimated that the risk of a periorbital BCC invading the orbits varies from 0.8 to 3.6% of cases.8-10 Among the risk factors are histologic sclerodermiform, micronodular, and infiltrating subtypes, recurrent tumors, development duration in excess of one year, compromise of the medial or lateral canthus, and neural invasion.9-11 The signs and symptoms that are most frequently linked to orbital invasion are adherence of the tumor to the orbital bone, limitation of the ocular motility, diplopia, displacement of the eyeball due to mass effect, palpebral ptosis and, more rarely, proptosis.1,12 The tumor spreads through the periosteum of the orbital cavity, but rarely invades the eyeball.1, 11 Intracranial involvement usually takes place via neural invasion through the superior orbital fissure,13, 14 which is the path of the oculomotor (III cranial nerve) and abducens nerves (VI cranial nerve), and lacrimal and frontal branches of the ophthalmic nerve - which in turn is a branch of the trigeminal nerve (V cranial nerve). A multidisciplinary approach, with the presence of an ophthalmologist, and/or head and neck surgeon is essential in such cases.
Mohs micrographic surgery (MMS) is considered the gold standard treatment for periocular tumors due to the fact that it enables accurate histological control of surgical margins, ensuring a higher cure rate, with lower recurrence rates.10,15,16 An additional advantage of the Mohs' technique is that it allows for a greater economy of the healthy tissue around the tumor, favoring the preservation of important structures and the surgical closure.9-11
Although some periocular tumors are easily handled, most of them are difficult to approach due to their size, location, and aggressive biological behavior. Salashe17 notes that for these tumors, there should ideally be a multidisciplinary team prepared to deal with any tumor size, complex surgical reconstructions, and the management of any possible complications.
The present study is aimed at presenting the particularities and challenges of approaching periocular tumors, through analysis of cases where operations were performed at a Mohs micrographic surgery reference center.
A retrospective, observational, cross-sectional study was carried out through a review of medical records, operative records, and a vast photographic archive.
Thirty-four periocular tumors were studied in 33 patients operated on between April 2010 and April 2014, and who were followed up with until September 2014. The patients analyzed had Fitzpatrick skin phototypes II and III. The tumors had the following distribution: 6 in men and 28 in women, 22 were primary tumors, 10 were recurrent, and 2 were incompletely excised.
All patients who underwent surgery had previous biopsies, with paraffin specimens and reports issued by pathologists. Tumors were divided according to histologic type and classified according to the previous biopsy report or the histological analysis performed during surgery (where it was possible to detect remaining tumors in the evaluated margins). In case of an inconsistency between histological subtypes observed in the biopsy reports and those observed in the slides analyzed during surgery, the latter was chosen for the study. This happened in three cases: the previous reports recorded the nodular BCC subtype in two cases and the sclerodermiform BCC subtype in one case; during surgery all three were found to be of the infiltrating BCC type.
In two BCC cases there was no classification of the histological subtype in the report of the incisional biopsy issued by the pathologist. In such cases, the histological slide was requested and analyzed by the Mohs surgeon, with both having been classified as nodular BCC subtype.
The tumors were still classified into primary, recurrent and incompletely excised, and those that had had their surgical safety margin compromised. This was done according to the histological report drafted after the previous conventional surgery and in consideration of those that were referred to Mohs micrographic surgery for a widening of margins.
The anatomical features of this region impose difficulties for dermoscopic visualization, by hampering the delimitation of margins through dermoscopy. Therefore, a choice was made to delimit margins with the naked eye. In all cases an initial surgical margin was marked based on the clinically apparent boundaries of the lesion. A 2 mm margin was used for nodular BCCs, while a 3 mm margin was used for other BCC subtypes, SCCs, and SCs.
Patients with recurrent or aggressive histological subtype tumors, or with tumors located in the medial or lateral canthal region underwent computerized tomography (CT) with contrast and fine cuts in the topography of the orbit. In all, 10 patients with an increased risk of subclinical invasion of the intraorbital structures were operated on with the participation of an ophthalmologist specializing in ocular plastic. One patient with recurrent SC also had the participation of a head and neck surgeon.
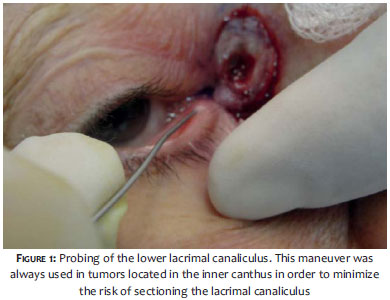
All patients with lesions in the medial canthal region underwent a probing of the upper and/or lower lacrimal canaliculus aimed at minimizing the risk of injury during the tumor resection (Figure 1).
Only two cases were operated on under general anesthesia; the others received tumescent local anesthesia and sedation.
Most tumors operated on were located in the lower eyelid or internal canthus.
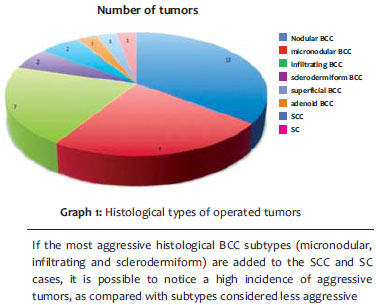
BCC was the most frequent tumor, at 31 cases, with the nodular subtype found in 12 patients, followed by the micronodular (8 cases), infiltrating (7 cases), sclerodermiform (2 cases), superficial (1 case) and one with adenoid differentiation. Other tumors operated on were: SCC (2 cases) and one recurrent SC in the upper eyelid (Graph 1).
None of the patients had an image compatible with the invasion of the orbital cavity under CT.
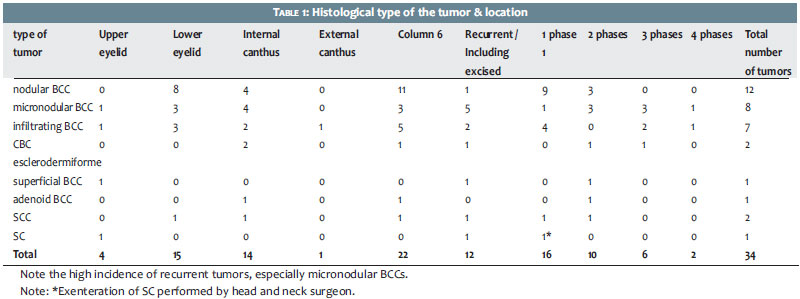
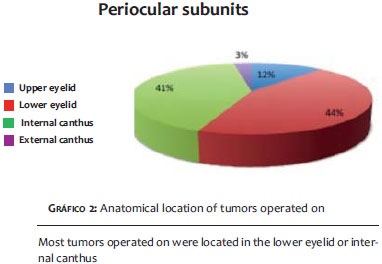
The most affected periocular subunit was the lower eyelid (15 cases), followed by the internal canthus (14 cases), the upper eyelid (4 cases), and external canthus (1 case) (Table 1 and Graph 2).
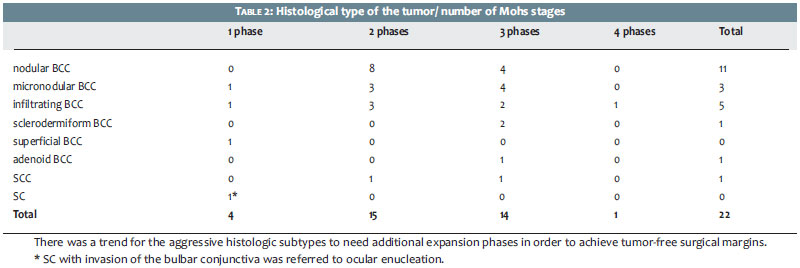
Regarding the number of stages/phases needed to achieve free margins, only 16 were free of neoplasms, given the initial margin of 2-3 mm. In 10 cases, 2 expansion phases were required; 6 cases needed 3 phases; and 2 cases required 4 phases. (Table 2)
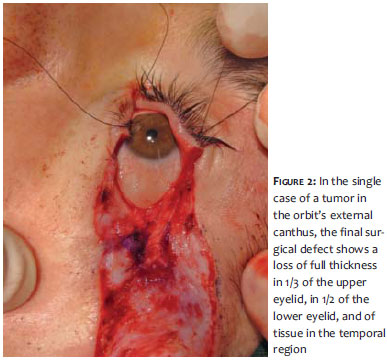
Surgical closure was highly variable according to the size of the surgical defect and location. In lower eyelid tumors, 7 inferior rotation flaps were performed, 1 upper eyelid transposition flap, 1 primary closure, and 6 ear helix chondro-perichondrial grafts.5 The simple skin graft was used in 9 tumors in the internal canthus, skin flaps were used in 3 cases, and primary closures were used in 2 cases. In the upper eyelid, skin flaps were used in 2 cases, a graft was used in 1 case, and the orbital exenteration was used in 1 case of recurrent SC. In the single case of an external canthus lesion, the tumor occupied 1/3 of the upper eyelid and half of the lower eyelid (Figure 2). An ear helix chondro-perichondrial graft was used for the reconstruction of the inferior tarsus and a periosteal flap for the reconstruction of the superior tarsus, followed by the performance of a lateral advancement skin flap for the closure of the upper eyelid.
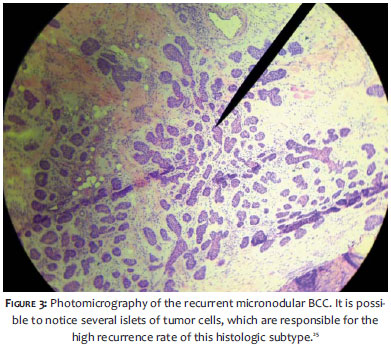
The follow-up time ranged from 5 to 48 months, with 1 to 4 years in 26 patients (76.5%) and shorter than 1 year in 8 patients (23.5%). One female patient had recurrence of an extensive micronodular BCC in the nose and internal canthus (Figure 3). Having previously undergone PDT in 2012, she was advised by a dermatologist physician to seek care at the authors' dermatologic service, when the lesion recurred. She then underwent MMS in January 2013, through surgical reconstruction with a simple skin graft. After 8 months a tumor recurrence was identified at the graft's superior border, and she underwent a new MMS in November 2013. The patient had no signs of recurrence up to the date this paper was submitted (10 months of follow-up).
Regarding complications in the post-operative period, 1 patient had a lower lacrimal canaliculus injury due to tumor infiltration, which progressed to epiphora, and was then referred to the ophthalmologist for evaluation for a possible connective tissue surgery (dacryocystorhinostomy) six months after the CMM. In 5 lower eyelid tumor cases there was a slight scleral show, without relevant functional or aesthetic compromise. One case progressed with chondrite in the donor area of the chondro-perichondrial graft in the ear helix, which was easily resolved with oral corticosteroids.
In line with the international literature, BCC was the most common tumor (91.17% of the patients).12 Considering the fact that the BCC's more aggressive histological subtypes are the sclerodermiform, micronodular and infiltrating1,3, the present study will have come across a large number of aggressive tumors (54.83%) - higher than the average found in the literature.1,8,10 This may be explained by the fact that they were sourced at a reference center for MMS, where most cases have a high complexity level, which also explains the large number of recurrent or incompletely excised tumors, with 12 cases (35.29%) having been operated on during the study's period.
As compared to BCCs, tumors located in the internal canthus have a higher incidence of aggressive subtypes,1,6,16 with 4 micronodular, 2 infiltrating and 2 sclerodermiform tumors (Table 1). That was also the location of the only case of recurrence after MMS. This confirms data from the literature, which point to internal canthus tumors as having greater invasiveness and a poorer prognosis.18,19
As for the location of the lesions, the data from the present study is aligned to the literature,1,2 with a predominance in the lower eyelid (44.11%), followed by the internal canthus (41.17%), the upper eyelid (11.76%) and the external canthus (2.94%) (Graph 2).
Large surgical margins imply larger surgical defects, requiring complex reconstructions. Most authors recommend using the smallest possible safety margin, sufficient only to completely remove the tumor without generating excessively large defects, thereby minimizing the functional and cosmetic deficits. Hsuan et al.20 demonstrated that 2 mm margins were insufficient for the complete removal of nodular BCC from the eyelid in about 18% of cases. Chadha et al.21 recommend 2 mm margins in clearly delimited BCCs, having found incompletely excised surgical margins in approximately 13% of cases and a recurrence rate of 3.3%. Other studies recommend 3-5 mm surgical margins for tumors in the area.8, 11, 22
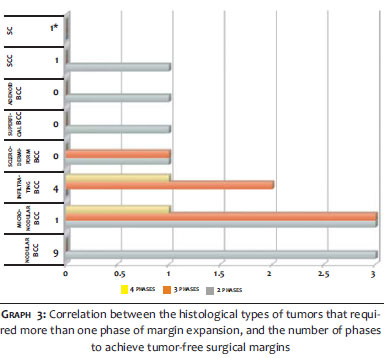
Although the surgical margins recommended for the treatment of BCC with conventional surgery are variable and depend on the histological type and the affected area,23 in general, most authors consider surgical margins between 2-5mm reasonable for the eyelids.11, 19-21 With MMS, the authors used an initial margin of 2-3mm, which was not enough to excise the tumor in most studied cases, since 52.94% of tumors needed more than 1 phase of surgical expansion (Graph 3). This finding demonstrates the importance of the histological control of margins through MMS.
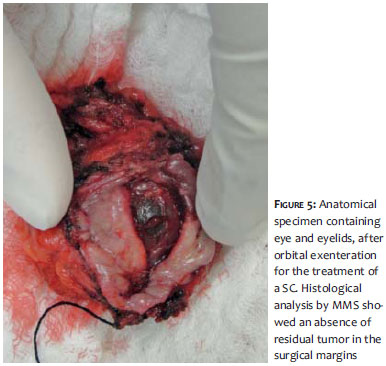
Although some authors question the use of MMS for the treatment of SC,24 the strict histological control achieved by the Mohs technique was important in the management of a case of recurrent SC in the upper eyelid in which a bulbar conjunctival invasion was identified during the procedure. In this case a choice was made for an orbital exenteration during the same surgical event, with the involvement of a head and neck surgeon (Figures 4 and 5). After the exenteration, a new perioperative histological analysis of the margins was performed, in which the tumor was not observed, making it unnecessary to perform a new surgical approach to extend the exenteration. The patient's follow-up was carried out by the Head and Neck Surgery and Radiotherapy Departments, with no recurrence having been found as of the submission date of the present paper.
The multidisciplinary team effort, which included the contribution of an ophthalmologist and a head and neck surgeon, was critical to the success of the most complex cases, allowing a better approach to deep soft tissues in the orbit and assisting in complex surgical reconstruction and post-operative management.
Notwithstanding the short follow-up time, which ranged from 1 to 4 years in 76.5% of patients - and shorter than 1 year in 23.5% - there was a low recurrence rate, with only one case (2.94%) to date.
Regarding the type of surgical reconstruction, several techniques were used according to the surgical defect's location and size. Five patients developed slight scleral show, with minimal aesthetic impact, and an absence of any recorded cases of ectropion, entropion, or infection.
The complex anatomy and the peculiar biological behavior of tumors affecting the periorbital region require a specific knowledge on the part of the dermatologic surgeon and the support of a multidisciplinary team.
Most tumors operated on had aggressive histologic subtypes, with roughly 1/3 being recurrent or incompletely excised, evidencing the high degree of difficulty of treating these tumors.
Regarding BCCs, tumors located in the internal canthus showed more aggressive biological behavior, coinciding with the literature data.1,16,19 This was also the location for the only case of recurrence after MMS - one micronodular BCC, which had a large subclinical size - a fact aligned with the literature that deems this subtype as highly recurrent.25
Although surgical margins of 2-3 mm have been performed in all tumors by numerous authors,18,20,21,22 and considered reasonable for the treatment of primary BCC, most cases in the present study required successive expansion phases in order for neoplasia-free margins to be achieved (Table 2). This datum demonstrates the importance of strict histological control of surgical margins achieved by MMS.
Of the 20 tumors with subtypes considered aggressive, 13 (65%) required more than one expansion phase. Of the 14 less aggressive tumors, only 5 (35.7%) demanded more than 1 expansion phase, demonstrating the relationship between aggressive histological types and subclinical invasion.
Despite the limited size of the sample and the short follow-up time, MMS yielded a high cure rate and a low recurrence rate to date.
The multidisciplinary approach to periocular tumors provided an excellent oncologic management, with maximum functional and aesthetic preservation.
1. Kourt G, Martin P. Eyelid and Periocular Skin Tumors. In: Zeynel A. Karcioglu, editors. Orbital Tumors: Diagnosis and Treatment. New York: Springer; 2005. p. 233-44.
2. Spinelli H M, Jelks GW. Periocular Reconstruction: A systematic approach. Plast. Reconstr. Surg. 1993;91(6):1017-24.
3. Wang JK, Liao SL, Jou JR, Lai PC, Kao SC, Hou PK, et.al. Malignant eyelid tumours in Taiwan. Eye (Lond). 2003;17(2):216-20.
4. Margo CE, Waltz K. Basal cell carcinoma of the eyelid and periocular skin. Surv Ophthalmol. 1993;38(2):169-92.
5. Faustina M, Diba R, Ahmadi MA, Esmaeli B. Patterns of regional and distant metastasis in patients with eyelid and periocular squamous cell carcinoma. Ophthalmology. 2004;111(10):1930-2.
6. Robert P, Taylor MC, James A, Lehman MC. Sebaceous Adenocarcinoma of the Meibomian Gland Presentation of a Case and Review of the Literature. Arch Ophthalmol. 1969;82(1):66-8.
7. Sanchez FH, Eduardo L. Reconstrução palpebral com enxerto condro-pericondral de hélice de orelha. Experiência de um centro de referência em cirurgia micrográfica de Mohs. Surg Cosmet Dermatol. 2013;5(4):324-9.
8. Amjadi M, Coventry B, Greenwood J. Surgical Treatments of Non-Melnaoma Skin Cancers: A Review. The Internet J Plast Surg. 2010;7(2). [Cited 2014 Aug 10]. Available from:: https://ispub.com/IJPS/7/2/9861 .
9. Muller FM, Dawe RS, Moseley H, Fleming CJ. Randomized comparison of Mohs micrographic surgery and surgical excision for small nodular basal cell carcinoma: tissue-sparing outcome. Dermatol Surg, 2009;35(9):1349-54.
10. Tüzün Y, Kutlubay Z,Engin B, Serdaroğlu S. Basal Cell Carcinoma. In: Xi Y, editor. Skin Cancer Overview. Croatia: InTech; 2011. [Cited 2014 Aug 10]. Available from: http://www.intechopen.com/books/skin-cancer-overview/basal-cell-carcinoma .
11. Telfer NR, Colver GB, Morton CA. Guidelines for the management of basal cell carcinoma. Br J Dermatol. 2008;159(1):35-48.
12. D Naidu D, R Salas, K Lee, W Payne. Cutaneous Non-Melanoma Malignancies with Retrobulbar Extension. The Internet J Plast Surg. 200;4(2). [Cited 2014 Aug 10]. Available from: https://ispub.com/IJPS/4/2/5185 .
13. Wood LD, Ammirati CT. An overview of mohs micrographic surgery for the treatment of basal cell carcinoma. Dermatol Clin. 2011;29(2):153-60.
14. Cumberland L, Dana A, Liegeois, N. Mohs micrographic surgery for the management of nonmelanoma skin cancers. Facial Plast Surg Clin North Am. 2009;17(3):325-35.
15. Ratner D, Lowe L, Johnson TM, Fader, DJ. Perineural spread of basal cell carcinomas treated with Mohs micrographic surgery. Cancer. 2000;88(7):1605-13.
16. Litwin AS1, Rytina E, Ha T, René C, Woodruff SA. Management of periocular basal cell carcinoma by Mohs micrographic surgery. J Dermatolog Treat. 2013;24(3):232-4.
17. Salasche SJ, Shore JW, Olbricht SM. Periocular tumors. Dermatol Clin. 1992;10(4):669-85.
18. Ishi LA, Pereira LC, Schellini SA, Marques MEA, CR. Padovani. Carcinoma basocelular da pálpebra - fatores relacionados com a recidiva tumoral. An bras Dermatol.2004;79(4):423-30.
19. Jankovic I, Visnjic M, Binic I, Kovacevic P, Jankovic D, Jankovic A. Does incomplete excision of basal cell carcinoma of the eyelid mean tumor recurrence? An. Bras Dermatol. 2010;85(6):872-7.
20. Hsuan JD, Harrad RA, Potts MJ, Collins C. Small margin excision of periocular basal cell carcinoma: 5 year results. Br J Ophthalmol. 2004; 88(3):358-60.
21. Chadha V, Wright M. Small margin excision of periocular basal cell carcinomas. Br J Ophthalmol. 2009; 93(6):803-6.
22. Margo CE, Waltz K. Basal cell carcinoma of the eyelid and periocular skin. Surv Ophthalmol. 1993;38(2):169-92.
23. Takenouchi T, Nomoto S, Ito M. Factors influencing the linear depth of invasion of primary basal cell carcinoma. Dermatol Surg. 2001;27(4):393-6.
24. While B1, Salvi S, Currie Z, Mudhar HS, Tan JH. Excision and delayed reconstruction with paraffin section histopathological analysis for periocular sebaceous carcinoma. Ophthal Plast Reconstr Surg. 2014; 30(2):105-9.
25. Hendrix JD Jr, Parlette HL. Micronodular basal cell carcinoma. A deceptive histologic subtype with frequent clinically undetected tumour extension. Arch Dermatol 1996;132(3):295-8.
This study was conducted at the Centro de Cirurgia Micrográfica do Rio de Janeiro da Policlínica Ronaldo Gazolla - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}