


Analupe Webber1; Lucio Bakos2; Isabel Cristina Palma Kuhl3; Carolina Degen Meotti4; Luiz Fernando Bopp Muller3
Keywords: KERATOSIS, ACTINIC; TREATMENT OUTCOME; THERAPEUTIC.
Actinic keratoses (AK) are dysplastic epidermal lesions induced mainly by chronic exposure to sunlight. Ultraviolet radiation can contribute to the keratinocytes' neoplastic transformation at the molecular level, as well as induce local and systemic immune response suppression, which normally regulates the destruction of malignant cells. Actinic keratoses lesions are considered to be part of a continuum of cellular damage, mutation, and histological processing, which can extend into the dermis as a squamous cell carcinoma, with metastatic potential.1 Therefore, it is recommended that all AK lesions be treated in order to avoid a possible invasive lesion, metastasis and even eventually death.1
There are many available options for the effective treatment of AK. Most have high cure rates - between 75% and 90%.2 The most common treatments are curettage, and cryotherapy.2-4 Topical 5-fluorouracil is the third most commonly used option.2, 3
Imiquimod is an immune response modifier for topical use that is approved for the treatment of AK, superficial basal cell carcinomas, external genital warts, Bowen's disease, lentigo maligna, molluscum contagiosum, verruca vulgaris, and stucco keratosis.5 It regulates the production of cytokines such as interferon-alpha, tumor necrosis factor-alpha, various interleukins of the innate immune response, as well as promoting cellular immune response type 1 T-helper.6, 7 In many studies, the complete and partial improvement of a AK was greater in the imiquimod group than in the placebo's, always with statistically significant differences. The total improvement rate of AKs treated with imiquimod ranged between 45% and 84% for the 16-week treatment scheme and 54% for the 8-week treatment scheme.8, 9
Photodynamic therapy (PDT) involves the use of a photosensitizing agent and the light of a precise wavelength to cause the death of specific cells, therefore allowing the treatment of AK lesions. Two topical photosensitizers can be used: 5-aminolevulinate (ALA) and methyl aminolevulinate (MAL) - ALA's methyl ester. MAL offers advantages over ALA since it has better skin penetration, due to the increased lipophilicity and high specificity for neoplastic cells.10 PDT has been associated with lower morbidity and better cosmetic results when compared with cryotherapy, the most frequently used modality in the treatment of AK.11
The main objectives of the present study were to compare the clinical responses of PDT and imiquimod in the treatment of AK, and assess whether there is a patient preference for either of the treatments.
Study population
The patients selected for the study were to be at least 20-years-old and have from 3 to 10 AK lesions in each hemiface or 6 to 10 AK lesions each.
They were recruited at the Dermatology Ambulatory of the Hospital de Clínicas de Porto Alegre, Rio Grande do Sul, Brazil.
The exclusion criteria were: suspected facial skin cancer, other cutaneous lesions on the face that could affect the clinical evaluation, alcohol or drug dependence, and clinically unstable systemic diseases.
Patients could not be currently using interferon or similar medicaments, other immunomodulating drugs, immunosuppressant drugs, cytotoxic drugs, or any topical treatment for AK lesions in the 3 months prior to the beginning of the study.
The use of moisturizers, retinoids, alpha- or beta-hydroxyacids, and topical corticosteroids in the treated areas was not allowed.
Study design
With the patients having signed a free and informed term of consent approved by the Institution's Research Ethics Committee, the study commenced.
The AK lesions were clinically diagnosed, measured (greatest diameter, in centimeters), mapped, photographed, with each patient being tagged with a number. After inclusion in the study, each received a randomization code, having been drawn for each of the treatment modalities. The patients received PDT with MAL and 5% imiquimod cream on alternate sides of the face (the randomization was used to determine which side of the patient's face should receive each of the treatments). Initially, the randomized side of the face received PDT with MAL, with the topical treatment with imiquimod 5% cream being initiated one month later, on the opposite side.
The same experienced dermatologist who performed the baseline evaluation and the total lesion count at the beginning of the study carried out the final assessment of each patient after the treatment, with the remaining lesions being measured and photographed again.
Each lesion was prepared prior to PDT with light curettage in order to remove hyperkeratotic scales and crusts, usually without bleeding. Topical anesthesia was not necessary. A 1 mm thick layer of 160 mg/g MAL cream (Metvix®; Tafarnaubach Penn Pharmaceutical Services Ltd., Tafarnaubach Industrial Estate, Tredegar Gwent, UK) was applied on each lesion, covering 5 mm of the adjacent skin. Each lesion was then covered with an occlusive dressing and aluminum foil for 3 hours. Next, the dressing was removed and the clean cream with 0.9% saline solution was applied immediately before illumination with red light using the light emitting diode device (Aktilite® CL 128, PhotoCure Inc., Oslo, Norway), with the following parameters: approximate 634 wavelength = 3.0nm, fluence = 37J/cm2, irradiance = 50mW/cm2 at 50 mm distance from the skin's surface, with a maximum variation of ± 10% in the target area over eight minutes. The patient and the medical team used protective goggles during the illumination period.
One month after receiving PDT with MAL, the patients started treatment with imiquimod cream. The medication (Aldara crem®, 3M Health Care Limited - Loughborough - Leicestershire, England) was supplied to the patient in 32 sachets of 250.0 mg. Patients were instructed to apply 5% imiquimod cream in the AK lesions of the contralateral hemiface that had undergone PDT, twice a week for 16 weeks. The patient should apply the cream in the evening and remove it the morning, subsequently applying a 30 SPF sunscreen (provided by the study) on the whole face. In order to increase adherence to the treatment, a poster with the topography of the lesions to be treated was provided. The patients were evaluated monthly.
The final evaluation was carried out by the same evaluator, who acted in a blinded capacity for the treatments performed on each side of the face. The lesions were examined, photographed, classified, and measured.
The patients were assessed for safety and tolerance in Weeks 1 and 4 after the PDT session , and in Weeks 4, 8, 12, and 16 during the treatment with imiquimod. Local and systemic adverse effects that might have occurred were looked for and recorded at each visit. The presence and severity of erythema, edema, vesicles, ulcers, and crusts were recorded on a scale from 1 to 4 (where 1 corresponded to the lack of reaction and 4 the presence of intense reaction). Safety was assessed at each visit by monitoring the occurrence of local and/or systemic side effects.
Patients with persistent AK lesions at the end of the study received alternative treatments (cryotherapy or chemical cauterization).
Statistical analysis
Based on previous studies,12, 13 the minimum sample of 11 patients was calculated to demonstrate the difference of one standard deviation in the individual responses and preferences, and the presence of side-effects when both methods were compared (with 90% power, considering α = 0.05).
The analyses were performed on a intention to treat basis. The data were processed using the software SPSS, version 14. 0.
The Wilcoxon and McNemar tests were used to compare imiquimod and PDT with MAL regarding the partial or complete cure of the lesions and adverse effects. The Bimodal Exact test was used to evaluate the patients' therapeutic preferences.
Twelve patients with a total of 245 lesions were included in the intention to treat analysis. All were women with Fitzpatrick's skin phototypes I or II. The average age was 69 years (ranging from 47 to 80 years). Only one patient had not undergone treatment for AK before entering the study. Cryotherapy was the most frequently used therapeutic modality prior to the study. Only one patient discontinued the use of imiquimod due to discomfort at the application sites during the 2nd month of treatment. Eleven patients completed the study.
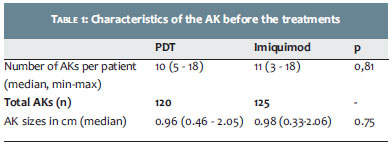
The average baseline number of AKs in the treated areas was 20 (± 8) lesions per patient. AKs in hemifaces treated with PDT and imiquimod had similar baseline characteristics (Table 1).
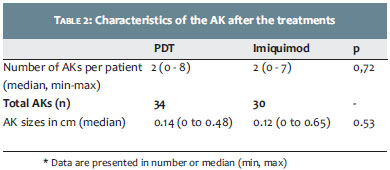
The two treatment methods showed good therapeutic response: 72% of lesions treated with PDT and 76% treated with imiquimod had complete improvement. The average sizes of residual lesions were similar after the two treatments (Table 2).
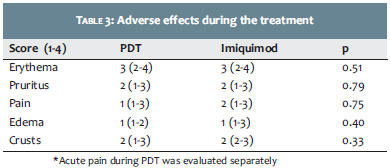
Regarding adverse effects, local cutaneous reactions (erythema, pruritus, pain, edema, vesicles, crusting) and systemic symptoms (headache, fever, malaise, weakness) were observed on the days following PDT and during the months of treatment with imiquimod; there was no statistically significant difference (Table 3). However, in the hemifaces treated with PDT, the local skin reactions were more intense in the 7 days after the sessions. With imiquimod, these signals tended to persist during the 16 weeks of treatment.
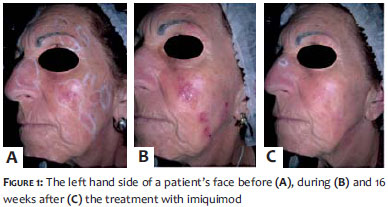
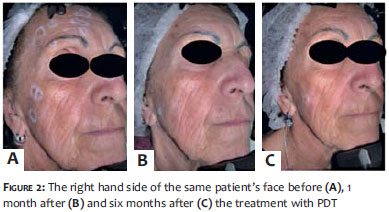
Serious or unexpected adverse reactions were not observed during the study. All patients showed some - mild in general - skin reaction (Figures 1 and 2).
During the PDT procedure, the pain was classified according to a pain scale (0 to 10). The mean value was 7, with a standard deviation of 5-8.
Any irritation reported at the site of injection during the study was deemed to be related to the treatment in progress in that region.
When asked whether they would repeat the treatment, one of the patients answered that she would not repeat the PDT treatment due to the pain, which she considered very intense, and to the inflammatory reaction on the following days.
The assessment of the aesthetic results did not show any hyperpigmentation, hypopigmentation, atrophy, or scarring in the treated areas. Two patients - one treated with imiquimod and the other with PDT - had mild persistent erythema in the hemifaces.
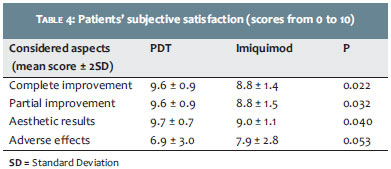
Patient satisfaction was graded with scores from 0 to 10 (total improvement, reduction of lesions, cosmetic results, and adverse effects). The scores of the first three items were significantly higher for PDT (Table 4). Regarding the subjective analysis of adverse effects, there was a trend toward higher scores for imiquimod, nonetheless without statistical significance.
Patients were asked about their preference regarding the two treatments. Of the 12 patients, 10 (83%) preferred PDT, with a statistical significance of (p = 0.03).
The present study was mainly aimed at evaluating the therapeutic response and patients' preference regarding the imiquimod and PDT treatments for AK.
Interestingly, each patient in this study served as her own control, ensuring the accuracy of the comparison. PDT offers a relatively selective and noninvasive therapy, which can be performed at an ambulatory clinic, ensuring adherence to the treatment. This provides benefits regarding patient adherence when compared to topical treatments that require prolonged use at home, especially those whose therapeutic effect are based on the inflammation of the skin.14
The present study offers the intention to treat results including all patients, independently of the cases where patients withdrew during the follow-up.
The therapeutic response rate - the study's main objective - was similar to those reported for other therapeutic modalities, including cryotherapy and 5-fluorouracil cream.8, 15 It is important to highlight that there was a decrease in the size of residual lesions with both treatment methods. Re-treatment with both modalities could further reduce residual lesions or completely cure the condition.
The results also showed that the patients preferred the PDT-based treatment. The study's intra-individual design offered a benefit in the comparison of the efficacy and patient preference between the two treatment options, in the same individual.
Both the PDT and the imiquimod treatments offer advantages over other treatments, especially when there is diffuse actinic damage.16
Due to the high frequency of AK and its potential for development into invasive squamous cell carcinoma, it is important that treatments not only be effective but also straightforward, with tolerable adverse effects and good aesthetic outcomes.17
Although the present study offered important information on the treatment of AK with PDT and imiquimod, it had some limitations, such as the small sample size and the lack of long follow-up periods with patients after the treatment. In addition, the patient sample was composed only of women, not reflecting the typical population of patients bearing AK.18
Although the skin discomfort with PDT occurred only during the week following the treatment, while that caused by imiquimod lasted for 4 months, they were comparable as for their intensity.
Despite the patients' subjective evaluation regarding adverse effects not being statistically significant, it tended to benefit imiquimod - probably due to the acute pain during the PDT session.
In conclusion, the results of the present study showed that both imiquimod and PDT were effective and well tolerated in the treatment of AK. However, patients overwhelmingly preferred PDT, probably due to the rapid improvement of lesions and because of its practicality. In addition, PDT was the first method to be performed, and patients may have had greater motivation to begin the treatment. Furthermore, patient motivation may also have been greater with PDT due to the fact that the application was carried out by physicians, while imiquimod was applied by the patient at home.
The present study was a pilot program. Future studies with greater numbers of patients and longer-term monitoring can confirm the outcomes.
1. Lee PK, Harwell WB, Loven KH, Phillips TJ, Whiting DA, Andres KL, et al. Long-term clinical outcomes following treatment of Actinic Keratosis with imiquimod 5% cream. Dermatol Surg. 2005;31(6):659-64.
2. Chamberlain AJ, Kurwa HA. Photodynamic Therapy. Is it a valuable treatment option for actinic keratoses. Am J Clin Dermatol. 2003;4(3):149-55.
3. Sotirou E, Spalla Z, Maliamani F, Zaparas N, Panagiotidou D, Ioannides D. Intraindividual, right left comparison of topical 5-aminolevulinic acid photodynamic therapy vs. 5% imiquimod cream for actinic keratoses on the upper extremities. J Eur Acad Dermatol Venereol. 2009;23(9):1061-5.
4. Lima HC. Fatos e mitos sobre imunomoduladores. An Bras Dermatol. 2007;82(3):207-21.
5. Stockfleth E, Meyer T, Benninghoff B, Salasche S, Papadopoulos L, Ulrich C, et al. A Randomized, Double-blind, Vehicle-Controlled Study to Assess 5% Imiquimod Cream for the Treatment of Multiple Actinic Keratoses. Arch Dermatol. 2002;138(11):1498-502.
6. Zeichner JA, Stern DWK, Uliasz A, Itenberg S. Placebo-controlled, double-blind, randomized pilot study of imiquimod 5% cream applied once per week for 6 months for the treatment of actinic keratoses. J Am Acad Dermatol. 2009;60(1):59-62.
7. Lehmann P. Methyl aminolaevulinate-photodynamic therapy: a review of clinical trials in the treatment of actinic keratoses and nonmelanoma skin cancer. Br J Dermatol. 2007;156(5):793-801.
8. Alomar A, Bichel J, McRae S. Vehicle-controlled, randomized, double-blind study to assess safety and efficacy of imiquimod 5% cream applied once daily 3 days per week in one or two courses of treatment of actinic keratoses on the head. Br J Dermatol. 2007;157(1):13341.
9. Ferrandiz C. Update on actinic keratosis in clinical trial experience with imiquimod. Br J Dermatol. 2007;157(Suppl 2): 32-33.
10. Wulf HC, Pavel S, Stender I, Wensveen CAB. Topical Photodynamic Therapy for Prevention of New Skin Lesions in Renal Transplant Recipients. Acta Derm Venereol. 2006;86(1):25-8.
11. Freeman M, Vinciullo C, Francis D, Spelman L, Nguyen R, Fergin P, et al. A comparison of photodynamic therapy using topical methyl aminolevulinate (metvix®) with single cycle cryotherapy in patients with actinic keratosis: a prospective, randomized study. J Dermatolog Treat. 2003;14(2):99-106.
12. Bjerring P, Funk J Poed- Petersen J. Randomized double blind study comparing photodynamic therapy (PDT) with Metvix® to PDT with placebo cream in actinic keratosis. Abstracts in the 29th Nordic Congress of Dermatology and Venereology. [cited 2014 Dec 17]. Available from: http://medicaljournals.se/forum/articles/6/Supplement%202/Suppl2.pdf
13. Lebwohl M, Dinehart S, Whiting D, Lee P, Tawfik N, Jorizzo J, et al. Imiquimod 5% cream for the treatment of actinic keratosis: Results from two phase III, randomized, double-blind, parallel group, vehicle-controlled trials. J Am Acad Dermatol. 2004;50(5):714-21.
14. Morton CA. Methyl aminolevulinate (metvix®) photodynamic therapy - pratical pearls. J Dermatolog Treat. 2003;14(Suppl 3):23-6.
15. Wiegell SR, Haedersdal M, Philipsen PA, Eriksen P, Enk CD, Wulf HC. Continuous activation of PpIX by daylight is as effective as and less painful than conventional photodynamic therapy for actinic keratoses; a randomized, controlled, single-blinded study. Br J Dermatol. 2008;158(4):740-6.
16. Vatve M, Ortonne J, Machin MAB, Gupta G. Management of field change in actinic keratosis. Br J Dermatol. 2007;157(Suppl 2):21-4.
17. Stockfleth E, Ferrandiz C, Grob JJ, Leigh I, Pehamberger H, Kerl H. Development of a treatment algorithm for actinic keratoses: a European Consensus. Eur J Dermatol. 2008;18(6): 651-9.
18. Merk HF. Topical diclofenac in the treatment of actinic keratoses. Int J Dermatol. 2007;46(1):12-18.
This study was conducted at the Hospital das Clínicas de Porto Alegre - Porto Alegre (RS), Brazil.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}