


Juliana Sandin1; Tatiana Gandolfi de Oliveira2; Viviana Chehin Curi3; Ana Carolina Lisboa de Macedo4; Fernanda Dias Pacheco Sakai3; Rossana Catanhede Farias de Vasconcelos5
Keywords: CHEMEXFOLIATION; THERAPEUTICS; SKIN; LACTIC ACID; HYPERPIGMENTATION.
Melasma is a common and usually symmetric pigmentation disorder, characterized by irregular and well-delimited hyperpigmented spots, affecting mainly the face in women, and which causes severe impairment in their quality of life. The natural history of melasma is characterized by a chronic clinical picture, recurrence despite treatment, and varying individual responsiveness to different therapies. 1-5
The term melasma is derived from the Greek melas, which means 'darkened' and refers to its brownish clinical presentation. Despite being recognized since the time of Hippocrates (470-360 B.C.), its actual prevalence is unknown. In 2013, Handel et al. in a population study carried out with civil servants who worked at a university campus in the city of Botucatu (UNESP-São Paulo, Brazil), melasma was diagnosed in 34% of women. The authors of that study believe that 15-35% of adult Brazilian women are bearers of melasma. 6 It is estimated that 5 to 6 million people in the US are affected and that 40% of the Southeast Asian population has melasma (Sundara, 2014). 1,7-9
Although it can occur in both genders and in any skin phototype, melasma is more common in women (9:1), prevailing in Fitzpatrick's phototypes III to V (and intermediate types), and is rare in extreme phototypes. It is believed that this is due to the inability of phototype I patients to induce pigmentation and those with phototype VI to produce pigment with maximum efficiency, thus characterizing stable phenotypes. 6
In Brazil, the majority of cases in women develop between the ages of 20 and 35 years of age, with phototype II and III patients showing melasma earlier than those of higher phototypes - which is explained by the sun-blocking role of melanin in delaying the development of the disease. Genetic predisposition is suggested by reports of family history. In a Brazilian study carried out with 302 patients, family history was present in 56% of them. Patients with a family history of melasma are younger than those without a family history. 1,4,6-8,10-12
Despite numerous studies on the subject, accurate causes of melasma are not fully understood. Most cases are associated with risk factors, such as ultraviolet radiation (UVR) and sex hormones, including combined oral contraceptive (COC) and pregnancy. Other factors include: anticonvulsant medications, photo-toxic medications, ovaries and thyroid diseases, food, intestinal parasites, liver disease, hormone replacement therapy (HRT), cosmetics, photosensitizing drugs, skin inflammatory processes and events causing stress, suggesting that the etiology of melasma is multifactorial and depends on environmental and hormonal factors, in addition to the important role of genetics. 5-7,12,13
Ultraviolet radiation is the most important factor in triggering the disease. The main melanogenesis inducing radiations are ultraviolet A (UVA) and ultraviolet B (UVB), while infrared radiation and visible light have a lower melanogenic potential. Various inflammatory mediators - in addition to inflammatory cells and vessels - are expressed in the skin with melasma in greater amounts than in healthy skin. It is also known that UV rays can lead to the production of multiple cytokines by keratinocytes, which stimulate melanogenesis. 6-11
It is likely that the action of hyperfunctional melanocytes is involved in the physiopathogenesis of melasma, and in the increase in the amount of epidermal melanin, in the number of melanosomes, and in the intensity of dermal elastosis. Melanocytic activity, represented by larger cells with more prominent dendrites, is observed. In these cells, it is possible to verify a larger quantity of melanin being produced and stored in a great number of melanosomes, as well as a greater number of cytoplasmic organelles. Furthermore, electron microscopy demonstrates increased synthesis of tyrosinase in melasma lesions. 1,2,10,11,14
The diagnosis of melasma is mainly clinical. It is a dermatosis characterized by asymptomatic, symmetrical hyper-chromic brownish macules in varied hues that have clear and irregular borders, often occurring in geographical configurations. Its course is chronic, recurring, and is more frequent in photoexposed body sites, especially in the face and neck. 1,6,9,11
There is no consensus on its clinical classification and, in practice, 3 main patterns of facial melasma are recognized: centrofacial type (affects the perioral, mentonian, and central region of the face); malar type (affects the zygomatic regions), and mandibular type (affects the mandible region).8,11 The MASI (Melasma Area and Severity Index) is the most widely used assessment method in studies involving melasma. Described in 1994 by Kimbrough-Grenn, it is used to clinically quantify the severity of facial melasma. The calculation of the MASI is based on the subjective assessment of 3 factors: area of involvement, pigmentation, and homogeneity of the melasma. 4,6,9,13,15,16
The treatment of melasma is a major clinical challenge whose main objective is the whitening of the lesions and the reduction of the affected area, with the fewest possible adverse effects. 6,10 Melasma has been traditionally treated with a combination of photoprotection, strategies to reduce melanin biosynthesis, and transport and transfer, in addition to therapies that reduce the amount of epidermal melanin, such as peelings. 6,12
The worsening of hyperpigmentation can occur even immediately after an event of low exposure to UVA, since redistribution and oxidation of pre-existing melanin take place. It has been demonstrated that the use of broad-spectrum sunscreen reduces the disease's intensity by up to 50%, while its incidence in pregnancy decreases by 90%. For this reason, the regular use of sunscreen has been affective both in preventing melasma and in increasing the efficacy of other topical agents. 6,12
Several treatment modalities are described that have as their aim to improve the appearance of melasma. However, none of these has emerged as resolutive, and cases of worsening are described mainly during summer. 17 Treatments with laser and intense pulsed light are popular yet still have questionable outcomes, with a great number of adverse effects and a paradoxical increase in pigmentation, especially in high skin phototypes. 5 Among the topical formulations are: hydroquinone, azelaic acid, arbutin ascorbic acid, retinoids, tranexamic acid, and others.5,13,18
Topical depigmenting agents are used with the aim of halting pigment production in melanocytes, and their main target is the tyrosinase. The inhibition of this enzyme reduces the conversion of DOPA into melanin. For over 50 years, hydroquinone has been used as a depigmentation agent through this mechanism.8,18 Hydroquinone can still be combined with tretinoin and with corticosteroids, a treatment known as triple combination that increases its effectiveness and is considered superior to monotherapy. 3,5,12,18
Superficial chemical peels have been used for years to treat melasma, especially refractory cases. 5 They inflict accelerated exfoliation or injury to the skin, induced by caustic agents that cause controlled damage to the basal layer.19 Among the agents used in this type of chemical peel are: alpha-hydroxy acid (AHA) - which is derived from the fermentation of foods - retinoic acid, and others. Both show similar results in melasma treatment. 5,10,19 The benefits of AHAs have been long recognized. There are reports for instance that Cleopatra used whey (lactic acid) as a facial treatment. The more frequently cited AHAs for the treatment of pigmentation disorders are glycolic and lactic acids, which act by inhibiting the activity of the tyrosinase and decreasing the formation of melanin. Although lactic acid has emerged as promising for the treatment of resistant melasma, there are still few studies on the subject. 9,15,16,18
To evaluate the effectiveness of 82% lactic acid peel in treating facial melasma.
A prospective comparative study was conducted at the Dermatology Department of the Faculdade de Medicina da Universidade de Santo Amaro (UNISA), in São Paulo. It was previously approved by the Committee for Research Ethics, and was carried out between September and November 2011. Sixteen women with facial melasma were treated with 3 sessions of 82% lactic acid gel peeling (dispensed by Center Formula® pharmacy - São Paulo, Brazil), applied at 15-day intervals.
The inclusion criteria were: female patients with a clinical diagnosis of moderate to severe facial melasma, who agreed to undergo the proposed treatment. All patients had high phototypes (III to V), had melasma for more than 1 year, and had already tried diverse treatments and clinical procedures. Pregnant and lactating women were excluded from the study.
Two groups of patients were randomly determined: one with patients who were previously using the triple combination (4% hydroquinone, 0.05% tretinoin, and 0.05% dexamethasone) for at least 2 weeks; the other with patients who had not been treating melasma for more than 60 days. A careful clinical evaluation was performed by the medical examiner. The average of the MASI severity index was individually estimated at time points before the treatment, 15 days after each session, and 15 days after the completion of the treatment. (Figures 1 to 4).
The calculation of the MASI is based on the subjective evaluation of 3 factors: the area of involvement, pigmentation, and homogeneity. Four areas of the face are evaluated in its calculation: frontal (FT), right malar (RM), left malar (LM), and mentonian (MT), respectively corresponding to 30%, 30%, 30%, and 10% of the total area of the face. Each area receives scores from zero to 6, according to its extension. The severity of melasma is measured by 2 factors: pigmentation (P) and homogeneity (H), in a scale ranging from 0 to 4. The mathematical formula is: MASI = 0.3 x (P x FT + H x FT) x AFT + 0.3 x (P x RM + H x RM) x ARM + 0.3 x (P x LM + H x LM) x ALM + 0.1 x (P x MT + H x MT) x AMT. Its output value ranges from 0 to 48. 4,13,15,16
The 82% lactic acid peeling was applied to all patients. A gauze dampened with the product was used for the application only in areas affected by melasma. A local mild erythema was expected 5 minutes after the application. In the absence of this outcome a new layer was applied and 5 additional minutes added on. The product remained on the patient's skin for a maximum of 10 minutes, and was then removed with saline solution.
The patients were instructed to apply 0.05% desonide cream at night during the first week after the procedure in order to avoid post-inflammatory hyperpigmentation. Those who were using the triple combination would resume it after this period. The adverse effects found were reported by the authors.
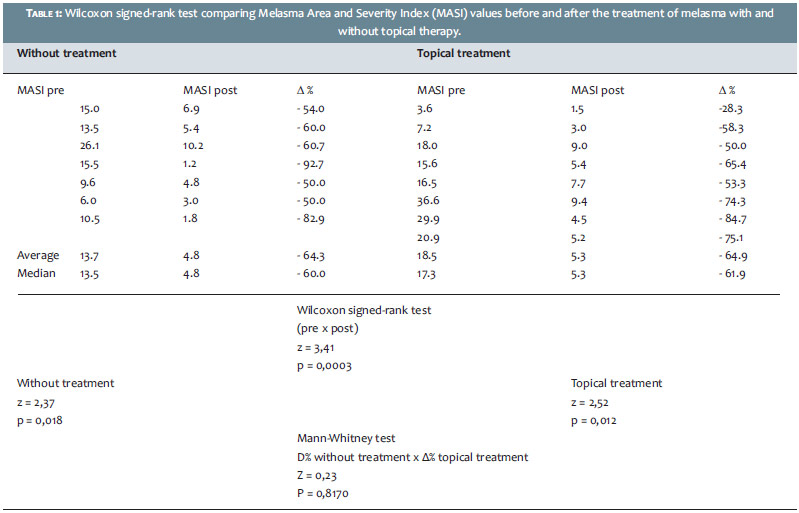
The Wilcoxon signed-rank test 20 was used in the analysis of the results in order to compare MASI values observed before and after the application of the product, for each group. The percentage differences were computed according to the following formula:
Δ% = [(post-value - pre-value) / pre-value] x 100.
The Mann-Whitney test 20 was applied to compare values of Δ% without the treatment and Δ% with topical treatment. Significance levels were established at 0.05 (or 5%).
Sixteen patients were selected for the study, 1 patient did not return for the last evaluation after the third application, and was excluded from the study. The patients' ages ranged from 31 to 62 years (mean = 41 years).
Eight patients were previously using the triple combination, the remaining 7 were not using any topical medication. Most patients required 2 peel applications at each session in order to achieve the expected response (erythema). None of the patients complained of discomfort at the moment of application.
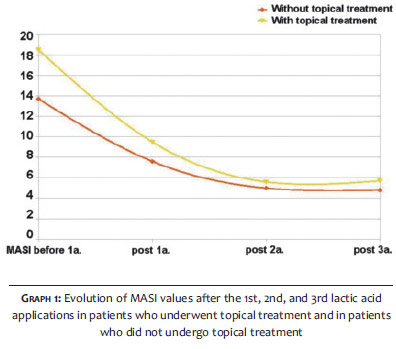
All patients saw their MASI values decrease (Table 1). In the group where patients were not using any topical agent for melasma, the average MASI was 13.7 before and 4.8 after the treatment. For the group that was using the triple combination, the initial average MASI was 18.5, falling to 5.7 after the completion of the treatment (Graph 1).
By comparing the MASI indices both pre- and post-application of acid lactic (82%), the Wilcoxon signed-rank test showed a significant reduction (p = 0.0003), with an initial MASI average of 17.3 as compared to a final MASI average of 5.3, with a 64% reduction (Table 1).
All patients showed the expected transient erythema immediately after applying the peel. Two had reversible complications after the first session - one of them with mild local desquamation and the other with exulceration - both in the malar region. All were treated with 0.05% desonide cream and had complete regression of these effects. From these patients, 1 belonged in the group that had been topically treated, with that treatment having been suspended for 30 days. All had improvement of lesions without formation of local post-inflammatory hyperpigmentation, and returned for other peeling sessions as planned. Regardless, 100% of patients were satisfied with the treatment that was performed.
Melasma is a common pigmentation disorder that affects a large portion of the population. According to a survey carried out by the Brazilian Society of Dermatology (SBD) in 2006, melasma corresponded to 8.4% of complaints in dermatology practices. 6 Due to the fact that it is an unaesthetic dermatosis located primarily on the face, it has a significant negative impact on affected individuals. Patients also report low self-esteem, withdrawal from social life, and have lower productivity levels. Although several treatments have been described for melasma, its therapeutic options remain a major challenge. 1,2,4,6,21
Superficial chemical peels are relatively simple procedures that have been reported in the literature since 1962, having been consolidated by the dermatologic practice.19 Chemical peels are indicated for the treatment of various dermatological conditions, and the most studied in the treatment of melasma are Jessner's solution and glycolic acid. 3,10 Side effects are possible after the use of peelings, with post-inflammatory hyperpigmentation being among them. It is suggested that prior preparation of the skin with topical products such as retinoic acid could reduce this complication. 3 This was not confirmed by the present study, as none of the patients had permanent side effects-nor by those who were not using any topical medication, with all patients having maintained the proposed treatment.
AHAs have been used effectively in the treatment of various dermatological conditions - among them glycolic acid, which is the main peeling agent used in the treatment of melasma.9 The dominance of US literature on the subject may explain the great number of publications on glycolic acid, which seems to be the preferred agent for superficial peeling in that country. 19 Although lactic acid is safe and cost effective, there are few indexed studies on its use in peels for the treatment of melasma. 15,16 The majority of authors report the necessity of 2 to 5 peeling sessions to achieve some result. 9,15,16 Although those authors use higher concentrations of lactic acid (85% to 92%), the present study's patients underwent only 3 applications of 82% lactic acid peeling, with all achieving an improvement of melasma.
The population evaluated in the present study reflects the melasma patients' epidemiology (i.e. high phototype women).1,6,7 In the studies describing the use of lactic acid, the patients had an initial MASI of 14.0 to 20.0, with a reduction of 57-80% after the application of lactic acid peel. 9,15,16 These data are aligned with the present study's findings, where the initial average MASI was 17.0, with a reduction of 64% after treatment. The present study's data show that the improvement was more significant after the first peeling application, with the melasma continuing to regress later on, albeit to a lesser extent. None of the studies quoting lactic acid suggested such a response.
It is known that the triple combination is the first line treatment for melasma. 13,17,18 Although highly effective, there was no difference between the treated group and those who did not receive the formula, showing that the results of the present study were due to the application of lactic acid peeling.
Regular use of sunscreen is effective both in the prevention of melasma and in the improvement of other topical therapies. 6,18 In the present study, all patients adhered to the regular use of sunscreens, and the great improvement of MASI can be due not only to the application of lactic acid peels, but also to this fact.
In line with what is reported in the literature, no permanent complications were described during the treatment with lactic acid peeling, demonstrating that it is an effective and safe resource. Notwithstanding, there is still a necessity for further controlled studies.
Pigmentary disorders (including melasma) are generally resistant to several types of treatment, causing frustration for both the patient and the physician. 1,13,21 Although there are few studies on lactic acid peel for treating this disorder, the present analysis has shown that it can be an important tool for improving resistant melasma, especially in patients with high skin phototypes.
1. Miot LDB, Silva MG, Marques MEA. Estudo comparativo morfofuncional de melanócitos em lesões de melasma. An Bras Dermatol. 2007;82(6):529-64.
2. Miot LDB, Miot HA, Silva MG, Marques ME. Fisiopatologia do Melasma. An Bras Dermatol. 2009;84(6):623-35.
3. Azzam OA, Leheta TM, Nagui NA, Shaarawy E, Hay RMA, Hilal RF. Different therapeutic modalities for treatment of melasma. J Cosmet Dermatol. 2009;8(4):275-81.
4. Pandya AG, Hynan LS, Bhore R, Riley FC, Guevara IL, Grimes P, et al. Reliability assessment and validation of the Melasma Area and Severity Index (MASI) and a new modified MASI scoring method. J Am Acad Dermatol. 2011;64(1):78-83.
5. Rivas S, Pandya AG. Treatment of melasma with topical agents, peels and lasers: an evidence-based review. Am J Clin Dermatol. 2013;14(5):359-76.
6. Handel AC, Miot LDB, Miot HA. Melasma: uma revisão clínica e epidemiológica. An Bras Dermatol. 2014;89(5):772-83.
7. KrupaShankar DSR, Somani VK, Kohli M, Sharad J, Ganjoo A, Kandhari S, et al. A cross-sectional, multicentric clinico-epidemiological study of melasma in India. Dermatol Ther. 2014.4(1):71-81.
8. Costa A, Moisés TA, Cordero T, Alves CRT, Marmirori. Associação de emblica, licorice e belides como alternativa a hidroquinona no tratamento clínico do melasma. An Bras Dermatol. 2010;85(5):613-20.
9. Magalhães GM, Borges MFM, Oliveira PJV, Neves DR. Peeling de ácido lático no tratamento do melasma: avaliação clínica e impacto na qualidade de vida. Surg Cosmet Dermatol. 2010;2(3):173-9.
10. Steiner D, Feola C, Bialeski N, Silva FAM. Tratamento do melasma: revisão sistemática. Surg Cosmet Dermatol. 2009;1(2):87-94.
11. Sheth VM, Pandya AG. Melasma: A comprehesive update. Part I. J Am Acad Dermatol. 2011;65(4):689-97.
12. Hexsel D, Lacerda DA, Cavalcante AS, Filho CASM, Kalil CLPV, Ayres EL. Epidemiology of melasma in Brazilian patients: a multicenter study. Int J Dermatol. 2014;53(4):440-4.
13. Arefiev KLB, Hantash BM. Advances in the treatment of melasma: a review of the recent literature. Dermatol Surg. 2012;38(7 pt 1):971-984.
14. Kang WH, Yoon KH, Lee ES, Kim J, Yim H, Sohn S, Im S. Melasma: histopathological characteristics in 56 korean patients. Br J Dermatol. 2002;146(2):228-37.
15. Sharquie KE, Al-Tikreety MM, Al-Mashhadani SA. Lactic acid as a new therapeutic peeling agent in melasma. Dermatol Surg. 2005;31(2):149-54.
16. Sharquie KE, Al-Tikreety MM, Al-Mashhadani SA. Lactic acid chemical peels as a new therapeutic modality in melasma in comparasion to Jessner's solution chemical peels. Dermatol Surg. 2006;32(12):1429-36.
17. Hexsel D, Soirefmann M, Dumêt Fernandes J, Siega C. Objective assessment of erythema and pigmentation of melasma lesions and surrounding areas in lomg-term management regimens with triple combination. J Drugs Dermatol. 2014;13(4):444-8.
18. Sheth VM, Pandya AG. Melasma: A comprehesive update. Part II. J Am Acad Dermatol. 2011;65(4):699-714.
19. Bagatin E, Hassun K, Talarico S. Revisão sistêmica sobre peelings químicos. Surg Cosmet Dermatol. 2009;1(1):37-46.
20. Siegel S., Castellan Jr N. J. Estatística não paramétrica para ciência do comportamento. Porto Alegre: Artmed; 2006.
21. Salem A, Gamil H, Ramadan A, Harras N, Amer A. Melasma: Treatment evaluation. J Cosmet Laser Ther. 2009;11(3):146-50.
The present study was carried out at the Dermatology Department of the Universidade de Medicina de Santo Amaro - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}