


Sílvia Arroyo Rstom1; Beatrice Martinez Zugaib Abdalla2; Gisele Gargantini Rezze3; Francisco Macedo Paschoal4
Keywords: KERATOSIS, ACTINIC; MICROSCOPY, CONFOCAL; DERMOSCOPY.
Chronic exposure to ultraviolet radiation (UV) is the primary cause of skin carcinomas, and actinic keratoses (AKs) are considered a precursor lesion of squamous cell carcinoma (SCC). AK is one of the most common dermatological diagnoses and affects an estimated 58 million people in the United States.1,2 In Australia it affects about 40-50% of individuals above 40 years of age due to the large proportion of individuals with phototype I and II skin in the population. 3 It is estimated that the relative risk of an individual carrying AK to develop SCC is 6-10%. 4
Excessive exposure to UV radiation can cause gene mutations in the keratinocytes' deoxyribonucleic acid (DNA). The UV radiation energy absorption by the DNA of the epidermal cells results in the production of cyclobutane-pyrimidine dimers and pyrimidine-pyrimidone photoproducts, the initial event of the immunosuppression, mutation, and carcinogenesis process.5 Topical application of photolyase - an enzyme present in virtually all living beings exposed to light with the exception of placental mammals - showed efficiency, with the removal of 40-45% of dimers from the DNA of human skin irradiated by UV. 6 Photolyase binds to cyclobutane-pyrimidine dimers (CPDs) and the exposure of the photolyase-dimer complex to radiation converts the dimerized pyrimidines to their original structure, fighting the carcinogenesis process. 5-8 When coupled with SPF 100 sunscreen, it enhances conventional photoprotection due to the potential for repairing the damage already established in the cellular DNA.
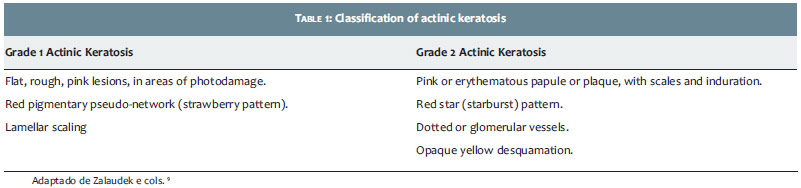
The classification of AK based on clinical and dermoscopic criteria results in Grade I and Grade II AKs (Table 1), with Grade II presenting the highest risk of progression into SCC. 9 In some patients it is possible to observe multiple AK lesions and in these cases, the concept of field cancerization can be used. It is a body area containing subclinical and multifocal pre-neoplastic abnormalities with genetic mutations that may constitute the origin of new primary tumors and local recurrence. 10-12
In recent years, there has been increasing interest in the development of non-invasive diagnostic tests aimed at detecting not only clinically suspected AK lesions, but also detecting and defining sub-clinical lesions, which must also be treated. 10,13 The in vivo confocal microscopy is a resource for viewing cutaneous changes "in vivo" and can also be used to monitor treatment. The main diagnostic criteria of AK in confocal microscopy are: irregular hyperkeratosis, pleomorphism, an epidermal nuclear increase, and architectural derangement. 14-16
The present study was aimed at evaluating the effect of applying a cream containing photolyase in liposomes, associated with SPF 100 sunscreen in patients with actinic damage and AK on the face, using dermoscopy and in vivo confocal microscopy (CM) as the evaluation parameter.
A longitudinal, observational clinical trial was carried out at the Dermatology Department of the Faculdade de Medicina do ABC.
Fourteen patients (8 men and 6 women, aged 45-65 years), with AK Grade I and Grade II, and other cutaneous signs of chronic actinic damage on the face were prospectively studied.
Selected patients who agreed to participate in the study were volunteers from the outpatient dermatology clinic. After a detailed explanation of the study's objectives, and how they were expected to collaborate, in addition to the clarification of doubts, the patients signed a consent term for the research, which aligned with the ethical principles of good clinical practice.
The inclusion criteria were: age 45-85 years, ability to understand the method to be used, agreement to participate in the project, and the presence of AK Grade I or II (associated or not with other cutaneous signs of chronic actinic damage).
The exclusion criteria were: inability to understand the method to be used, pregnancy, lactation, neurological and psychiatric diseases, photosensitizing disease, bearers of collagenoses (such as lupus erythematosus), the use of photosensitizing or immunosuppressants drugs, clinical suspicion of skin cancer, and lesions on the face compatible with active infectious diseases.
After the selection of AK lesions per patient, the documentation was performed through clinical photography, optical dermoscopy with polarized light dermoscope (Derm Lite FOTO System, USA) and in vivo CM (Viva Scope 1500, Mavig Viva Scope Systems, Munich, Germany).
The area evaluated through CM was 8 mm2, where half of the analyzed area presented the AK partially or fully, and the other half, the perilesional region.
The patients were instructed to perform daily application of the cream containing photolyase in liposomes and SPF 100 sunscreen (Eryfotona®-AK-NMSC, ISDIN Produtos Farmacêuticos LTDA, São Paulo, Brazil) and follow the recommendations in an explanatory leaflet. Patients were followed up with every 30 days at dermatologic consultations. After 120 days, new clinical photographic, dermoscopic and in vivo CM documentation was carried out.
The images obtained before and 120 days after the beginning of the treatment were compared and the evaluation of the response to the treatment in the AKs was carried out based on the dermoscopic polarized light images and the in vivo CM.
Seventeen AK lesions (14 Grade I and 3 Grade II) were documented with clinical and dermoscopic photographs before and after 120 days' use of the cream containing photolyase in liposomes and SPF 100 sunscreen, with 8 of these lesions studied through in vivo CM.
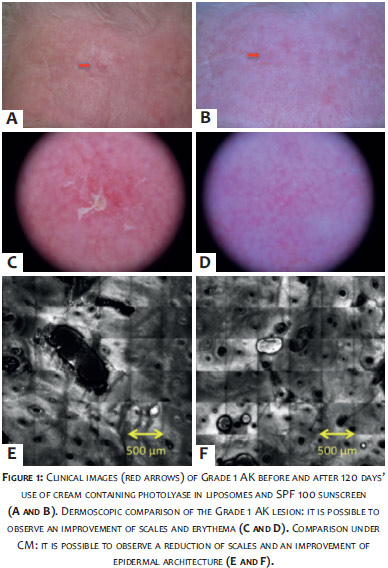
From the 14 Grade I AK, 9 had clinical and dermoscopic improvement, with reduction of erythema and desquamation (Figure 1), 3 remained unchanged, and 1 lesion developed into Grade II AK.
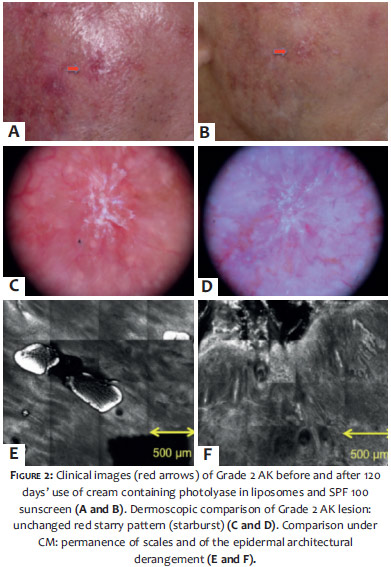
All 3 of the Grade II AK did not improve clinically or dermoscopically after 120 days using the cream. (Figure 2)
In the CM examination of 8 lesions, 5 were Grade I AK and 3 Grade II AK. All patients with Grade I AK had a reduction in desquamation and improvement in the epidermal architectural pattern in the examinations. The 3 patients with Grade II AK did not present changes under the CM after 120 days' use of the medication. (Figures 1 and 2)
Risk factors that contribute to the development of non-melanoma skin cancers are well known and mainly include race, age, gender, chronic exposure to chemical and physical mutagenic agents. (UV radiation), in addition to genetic factors. Excessive exposure to UV radiation, especially type B ultraviolet (UVB), is associated with an increased risk for developing skin cancers, including basal cell carcinoma and SCC, as it can cause gene mutations in the DNA of the keratinocytes. Failure to repair these genetic alterations can lead to uncontrolled cell growth and cancer formation. Furthermore, the UV radiation has a significant effect on the cutaneous immune system, inducing a state of local immunosuppression that prevents the rejection of tumors in formation.
Mutations that occur in the gene that encodes p53 protein - an important tumor suppressor gene - are directly related to the development of skin cancer, with UV radiation being its primary cause. High levels of p53 (evidenced by immunohistochemistry) due to mutations and increased gene expression can be considered as biological markers of actinic damage and field cancerization. 10
Photolyase is an enzyme belonging into the family of flavo-proteins and consists of 400 to 600 amino acids. It has an essentially globular structure. This enzyme is present in prokaryotic and certain eukaryotic organisms, including fish and marsupials, however it is absent in humans and placental mammals. These enzymes are produced by recombinant gene technology and/or extraction from bacteria and algae, and are then encapsulated in multilamellar liposomes. Photosomes® are liposomes containing biologically active photolyase, prepared from Anacystisnidulans (unicellular algae) cultures. The liposomal component comprises egg lipids, phosphatidylcholine, oleic acid, and cholesterol. 5,17
The two main types of DNA damage are the formation of cyclobutane-pyrimidine dimers (CPDs) and pyrimidinepyrimidone photoproducts (6-4PPs). These photoproducts interfere with the replication and cellular transcription processes, reducing the synthesis of RNA, decreasing the cell cycle's speed, and can result in apoptosis. The formation of dimers is of crucial importance in the carcinogenesis process: they promote mutations in tumor suppressor genes and contribute to cutaneous immunosuppression (allowing the disorganized growth of the transformed cells). 5-8
Humans have a repair system (nucleotide excision repair - NER), which functions as a defensive process to prevent adverse events caused by UV radiation, protecting the genome and removing lesions from the DNA. In addition to the NER, some biological systems, except for those of placental mammals, use photolyase to effectively remove the cyclobutane-pyrimidine dimers. Photolyase binds to cyclobutane-pyrimidine dimers (CPDs), creating a photolyase-dimer complex, whose exposure to radiation (300-500nm) converts the dimerized pyrimidines into their original structure (monomeric form). The process known as photoreactivation therefore involves two critical steps: the binding of the enzyme with the dimers (CPDs) - which is independent of light, and the catalysis process, which starts using a photon of blue light as the substrate, resulting in the repair of the CPDs. 5 Topical application of photolyase has proven very efficient, with the removal of 40-45% of the cyclobutane-pyrimidine dimers present in the UVB irradiated human skin, immediately after photoreactivation. Furthermore, it restored the expression of adhesion molecules (ICAM 1), which play a key role in maintaining the immune response of the skin following UVB radiation.
Another added benefit is that by reverting the CPDs, photolyase prevents the saturation of the natural repair systems and enhances the NER mechanism. 6
The application of exogenous photolyase differs from the conventional photoprotection in its ability to repair an already established damage to the cellular DNA. It represents an innovative strategy that promotes conventional photoprotection and DNA repair in the same product. Patients in the current study had a significant improvement in the of AK Grade 1 lesions and in the photodamage after 120 days' use of the medication. The drug was proven to have worked directly in the field cancerization, which is currently the subject of many studies as it is a site that must be treated in order to prevent the formation of new AKs and non-melanoma skin cancer.
Actinic keratosis is currently considered an incipient in situ SCC that develops into a process that involves several steps, where UV radiation leads to the formation of field cancerization and AK, culminating with the onset of SCC.1,18-20 Squamous Cell Carcinoma and AK are often contiguous lesions. In a study evaluating over 1,000 SCCs located in areas exposed to the sun, nearly 100% of the lesions had histological alterations consistent with AKs on their periphery. 21,22 Thus, in addition to being a precursor lesion of non-melanoma skin cancer, AK is also considered a marker of risk for the development of this group of neoplasias. Due to this fact, it is increasingly important to develop new technologies and products that also treat precancerous lesions and increase the awareness of the population regarding the use of sunscreen. The product in question has the advantage of associating an SPF 100 sunscreen to a drug that can inhibit some factors of carcinogenesis.
New non-invasive technologies that have aided in the diagnosis of these skin lesions are: dermoscopy examination and, more recently, the in vivo CM examination. These examinations are important not only to detect clinically suspicious lesions of AKs or SCCs, but also to detect and define subclinical field cancerization lesions and for following upon the proposed treatment.
Regarding the dermoscopy examination, there are few studies on the characteristics of this test in AK lesions. The more frequently described characteristic in the initial AK lesion is the red pigmentary pseudo-network pattern ("strawberry vascular pattern"). 23 As the lesion progresses into intraepithelial carcinoma, it develops a pattern called "red starburst", besides presenting diffuse yellow opaque scales. As the lesion gradually transforms into SCC, it increases neovascularization, developing grouped dotted or glomerular vessels, and finally linear and irregular vessels. In addition, the scales gradually become thicker and the presence of ulceration is common. 9 In the present study it was possible to analyze these patterns. The patients with a presence of a red pigmentary pseudo-network pattern and the presence of lamellar scaling showed an improvement in the dermoscopy examination after 120 days' use of medication. The patients with Grade 2 AK, with a "red starburst" pattern did not show such significant improvement in dermoscopy after taking the drug for only 120 days.
The in vivo CM emerged as a potential resource for studying epidermal cutaneous alterations, due to the fact that it allows the in vivo non-invasive visualization of the superficial layers of the skin, through images produced by different light reflection indices of the cutaneous structures, with a microscopic resolution similar to that of conventional histology. 14,24,25 In this manner, CM can also be used for the diagnosis of AK with a sensitivity and specificity of 98%. 13 It can currently be considered a non-invasive method for the diagnosis and monitoring of AK and field cancerization. 13
The CM findings of AK lesions include irregular hyperkeratosis with parakeratosis, architectural derangement, and enlargement of the nuclei of epidermal cells with pleomorphism. The architectural derangement pattern does not involve the total thickness of the epidermis in AK cases. The AK images can also have thick refractory bands in the dermis, corresponding to solar elastosis. 14, 15, 26-28
The major limitation of CM is the limited depth that the wavelength of the device reaches in the skin, preventing the precise visualization of the dermoepidermal junction in hyperkeratotic lesions. Ulrich et al. 26 reported an estimated sensitivity of 97.7% of the examination after having studied 44 cases of AK through CM. Therefore, CM can be a useful diagnostic tool in the management and follow-up of patients with low skin phototypes and a history of intense exposure to the sun, allowing the early diagnosis of AK. 26 Its use was also described in the monitoring of the therapeutic response after photodynamic therapy, demonstrating progressive normalization of the epidermal architecture in the cases treated successfully, paving the way for its use in monitoring and evaluation of the therapeutic response of other treatment modalities for AK. 29 In the present study, the CM examination was proven to be an important complementary diagnostic test for monitoring AK lesions and perilesional areas of field cancerization.
The topical application of the cream containing photolyase in liposomes and SPF 100 sunscreen is an innovative strategy. It provides photoprotection and repair of DNA through a single product, leading to the improvement of Grade I AK and of field cancerization, from the clinical, dermoscopic, and CM perspectives.
1. Ceilley RI, Jorizzo JL. Current issues in the management of actinic keratosis. J Am Acad Dermatol. 2013;68(1 suppl 1):28-38.
2. Berman B1, Bienstock L, Kuritzky L, Mayeaux EJ Jr, Tyring SK; Primary Care Education Consortium, et al. Actinic keratosis: sequelae and treatments. Recommendations from a consensus panel. J Fam Pract. 2006;55(suppl):1-8.
3. Nora AB, Panarotto D, Lovatto L, Boniatti L, Manozzo M. Frequency of counseling for skin cancer prevention by the vari- ous specialties in Caxias do Sul. An Bras Dermatol. 2004;79(1):45-52.
4. Salasche SJ. Epidemiology of actinic keratoses and squamous cell carcinoma. J Am Acad Dermatol. 2000;42(1Pt2):4-7.
5. Sancar A. Structure and fuction of photolyase and in vivo enzymology: 50th anniversary. J Biol Chem. 2008;283(47):32153-7.
6. Stege H, Roza L, VinkAA, Grewe M, Ruzicka T, Grether-Beck S, et al. Enzyme plus light therapy to repair DNA damage in ultraviolet-B-irradiated human skin. Proc Natl Acad Sci USA. 2000;97(4):1790-5.
7. Jans J, Shul W, Sert Y-G, Rijken Y, Rebel H, Eker PM, et al. Powerful skin cancer protection by a CPD photolyasetransgene. Current Biology. 2005;15(2):105-15.
8. Stege H. Effect of xenogenic repair enzymes on photoimmunology and photocarcinogenesis. J Photochem Photobiol B. 2001;65(2-3):105-8.
9. Zalaudek I, Giacomel J, Schmid K, Bondino S, Rosendahl C, Cavicchini S, et al. Dermatoscopy of facial actinic keratosis, intraepidermal carcinoma, and invasive squamous cell carcinoma: A progression model. J Am Acad Dermatol. 2012;66(4):589-97.
10. Braakhuis BJ, Tabor MP, Kummer JA, Leemans CR, Brakenhoff RH. A genetic explanation of Slaughter's concept of field cancerization: evidence and clinical implications. Cancer Res. 2003;63(8):1727-30
11. Torezan LA, Festa-Neto C. Cutaneous field cancerization: clinical, histopathological and therapeutic aspects. An Bras Dermatol. 2013;88(5):775-86.
12. Szeimies RM, Torezan L, Niwa A, Valente N, Unger P, Kohl E, et al. Clinical, histopathological and immunohistochemical assessment of human skin field cancerization before and after photodynamic therapy. Br J Dermatol. 2012;167(1):150-9.
13. Ulrich M, Maltusch A, Rowert-Huber J, Gonzalez S, Sterry W, Stockfleth E, et al. Actinic keratoses: non-invasive diagnosis for field cancerization. Br J Dermatol. 2007;156(Suppl):13-7.
14. Ulrich M, Stockfleth E, Roewert-Huber J, Astner S. Noninvasive diagnostic tools for nonmelanoma skin cancer. Br J Dermatol. 2007;157(Suppl):56-8.
15. Horn M, Gerger A, Ahlgrimm-Siess V, Weger W, Koller S, Kerl H, et al. Discrimination of Actinic Keratoses from Normal Skin with Reflectance Mode Confocal Microscopy. Dermatol Surg. 2008;34(5):620-5.
16. Braga JCT, Scope A, Klaz I, Mecca P, González S, Rabinovitz H, et al. The significance of reflectance confocal microscopy in the assessment of solitary pink skin lesions. J Am Acad Dermatol. 2009;61(2):230-41.
17. Hofer A, Legat FJ, Gruber-Wackernagel A, Quehenberger F, Wolf P. Topical liposomal DNA repair enzymes in polymorphic light eruption. Photochem Photobiol Sci. 2011;10(7):1118-28.
18. Kaufmann, R. The Concept of Field cancerization. e-Supplement Abstracts of the 6th Congress of the European Association of Dermatologic Oncology. 2010 Jun.
19. Berman B, Cohen DE, Amini S. What is the role of field-directed therapy in the treatment of actinic keratosis? Part 1: overview and investigational topical agents. Cutis. 2012;89(5):241-50.
20. Glogau RG. The risk of progression to invasive disease. J Am Acad Dermatol. 2000;42(1pt 2):23-4.
21. Guenthner ST, Hurwitz RM, Buckel LJ, Gray HR. Cutaneous squamous cell carcinomas consistently show histologic evidence of in situ changes: A clinicopathologic correlation. J Am Acad Dermatol. 1999;41(3 pt 1):443-8.
22. Yanofsky VR, Mercer SE, Phelps RG. Histopathological variants of cutaneous squamous cell carcinoma: a review. J Skin Cancer. 2011;2011:210813.
23. Zalaudek I, Giacomel J, Argenziano G, Hofmann-Wellenhof R, Micantonio T, Di Stefani A, et al. Dermatoscopy of facial non-pigmented actinic keratosis. Br J Dermatol. 2006;155(5):951-6.
24. Rigel DS, Gold LFS. The importance of early diagnosis and treatment of actinic keratosis. J Am Acad Dermatol. 2013;68(1):S20-7
25. Gerger A, Koller S, Weger W, Richtig E, Kerl H, Samonigg H, et al. Sensitivity and specificity of confocal laser-scanning microscopy for in vivo diagnosis of malignant skin tumors. Cancer. 2006;107(1):193-200.
26. Ulrich M, Maltusch A, Rius-Diaz F, Rowert-Huber J, Gonzalez S, Sterry W, et al. Clinical applicability of in vivo reflectance confocal microscopy for the diagnosis of actinic keratoses. Dermatol Surg. 2008;34(5):610-9.
27. Wurm EMT, Curchin CES, Lambie D, Longo C, Pellacani G, Soyer HP. Confocal features of equivocal facial lesions on severely sun-damaged skin: Four case studies with dermatoscopic confocal and histopathologic correlation. J Am Acad Dermatol. 2012;66(3):463-73.
28. Rishpon A, Kim N, Scope A, Porges L, Oliviero MC, Braun RP, et al. Reflectance confocal microscopy criteria for squamous cell carcinomas and actinic keratoses. Arch Dermatol. 2009;145(7):766-72.
29. Giacomo THBD, Santiago AVDA, Braga JCT, Blumetti TCMP, Ferreira JASLB, Canosa JM, et al. Perspectivas no uso da microscopia confocal in vivo na prática do cirurgião dermatológico. Surg Cosmet Dermatol. 2011;3(4):338-44.
The present study was carried out at the Faculdade de Medicina do ABC (FMABC) - Santo André (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}