


Doris Hexsel1; Mariana Soirefmann2; Juliana Schilling de Souza3; Denise Zaffari4; Renata Boscaini David5; Carolina Siega6
Keywords: CELLULITIS; LIPODYSTROPHY, DIET THERAPY.
Cellulite affects nearly all women. Its prevalence is estimated at around 80-90% and although it is not considered a pathological condition, it can cause emotional distress1,2 and is a frequent complaint on the part of patients. It occurs more frequently in the obese population, however it also affects those who are lean. It is rare in men, and in women usually starts after puberty, mainly affecting the thighs, buttocks and abdomen. 3,4 Cellulite can arise with different clinical aspects, such as those referred to as "orange peel", "cottage cheese" or "mattress appearance".
Although cellulite's pathogenesis has not yet been fully elucidated, some scientific evidence links this condition to the peculiar anatomy of women. 5,6 Among the described etiologic factors are changes in the adipose tissue 7 and the configuration of the subcutaneous connective septa.5,6 The literature also quotes hormone and genetic 7 influences, and changes in the microcirculation. 8,9
Alterations in the skin's relief caused by cellulite include elevated and depressed lesions. Subcutaneous fibrous septa that connect the skin to the muscle fascia produce traction on the skin, resulting in depressed lesions. 5 Elevated lesions are caused by the accumulation of fat, which causes tension within the lobe, resulting in the herniation of fat through the dermis.7 Those herniations protrude on the cutaneous surface, producing the different appearances of the elevated lesions (orange peel, cottage cheese and mattress appearance). Nevertheless, no differences in the adipose tissue of elevated areas is observed, compared to the other areas.10 Furthermore, sagging skin is an important aggravating factor of cellulite, especially with increasing age, and is more visible in women over 40-years-old. 4,11
Although there is a positive correlation between cellulite and being overweight,10 its manifestation is also common in women of normal weight and even those that are lean. However, the correlation between specific dietary patterns and the presence or worsening of cellulite is not known. It is believed that treatments aimed at losing weight can have positive effects on the appearance of cellulite, however there is still controversy about what optimal composition of diet could help to reduce the degree of cellulite.12 The present study was aimed at evaluating the effect of a diet low in carbohydrates on reducing the degree of cellulite in women with normal weight, compared to standard diets and those with a high-protein content.
A prospective monocentric study was conducted at the Centro Brasileiro de Estudos em Dermatologia (Brazilian Center for Studies in Dermatology), in the southern city of Porto Alegre, Brazil, after having been approved by the Hospital Moinhos de Vento's Research Ethics Committee. In accordance with the applicable regulations and guidelines of good clinical practice, all patients were fully informed about the study, having signed a term of informed consent before participating in the study.
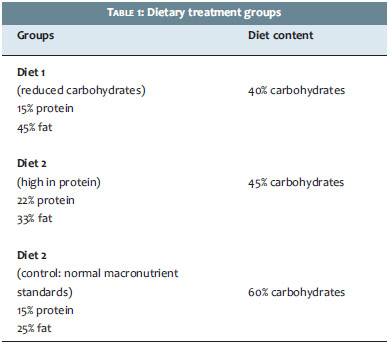
Forty-three female patients aged between 18 and 40 years were included and randomized into one of three treatment groups receiving different dietary macronutrient content, with each diet having the same total caloric value. For the distribution of patients into the groups, a randomization list generated by a statistician external from the study was used. Table 1 summarizes the treatment groups according to the selected diet.
The main inclusion criteria were: body mass index (BMI) between 18.5 and 24.9 kg/m2, use of effective contraception method, absence of signs of inflammatory or infectious process in the body sites studied by the evaluation, and a moderate to severe degree of cellulite in the buttocks according to the Cellulitis Severity Scale (CSS). 13
Six follow-up visits were conducted during the study. At the screening visit, a dermatologist clinically assessed the patients and rated the degree of cellulite according to the CSS.13 A dietitian was responsible for the nutritional assessment, as well as for the dietary guidance.
Assessed body circumferences included the waist (midpoint between the iliac crest and the lower costal margin), hip (point of maximum circumference over the buttocks) and arm (midpoint between the acromion and the olecranon), taken with a non-extensible tape measure, in centimeters and millimeters. The cutaneous folds measured were the triceps and sub-scapular folds. The cutoff point was parameterized using the 50th percentile, as described by Frisancho.14 The patients' weight was measured using a scale (Welmy®, Brazil) without clothes and without shoes, while the height was measured using a wall stadiometer. The patients' diet was followed upon by the nutritionist, using the assessment tool of the standard food-questionnaire. The patients recorded their food intake for three days a week over five months - two working days (Tuesdays and Thursdays) and a weekend day (Sunday). This record served as the basis for calculating the percentage of the patients' adherence to the proposed diet, taking into account the percentage of ingested macronutrients versus the percentage proposed in the diet.
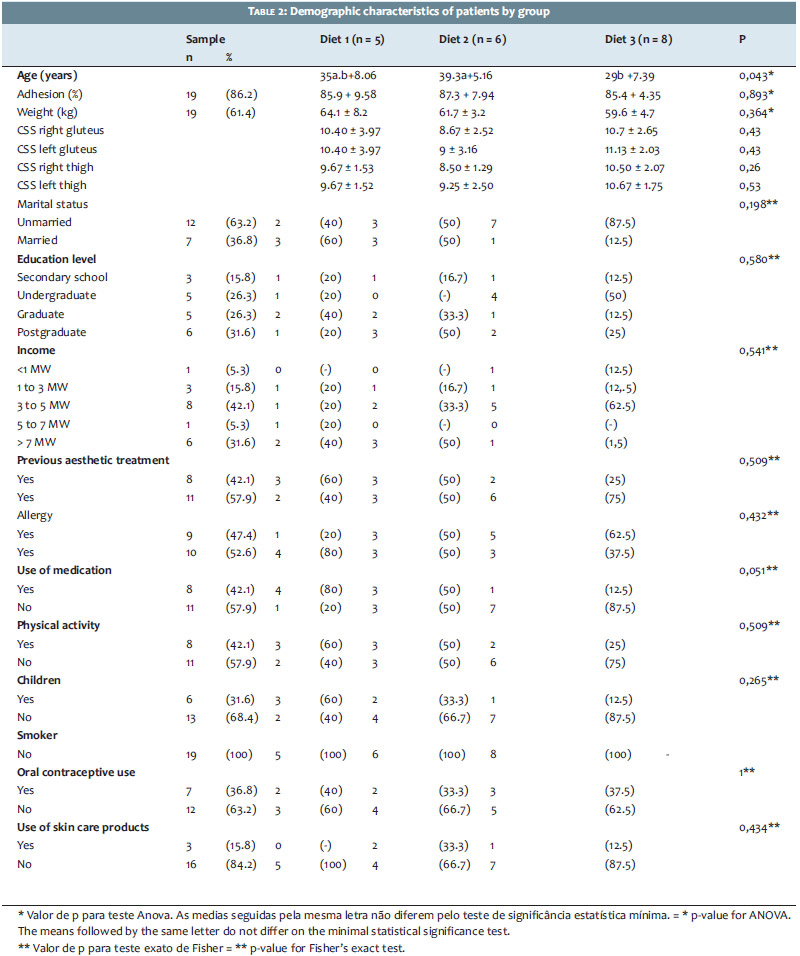
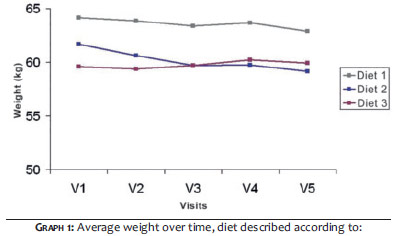
Nineteen of the 43 patients included (44.2%) completed the study: 5 in Group 1, 6 in Group 2, and 8 in Group 3. The demographics are described and stratified by diet in Table 2. The mean values for dietary adherence ranged between 85-89%, with no difference in adherence between groups. The average age of the patients who followed the diet with high-protein content (Diet 2) was higher when compared to that of those who followed the control diet (Diet 3) (p = 0.04). Other demographics were similar between diets, including weight and the degree of cellulite at baseline. Despite not being a significant aspect, the patients who followed the diet with high-protein content (Diet 2) had a lower degree of cellulite in the buttocks at baseline. That diet produced a significant decrease in weight over time (p <0.05), which was not observed with the other two diets (Graph 1).
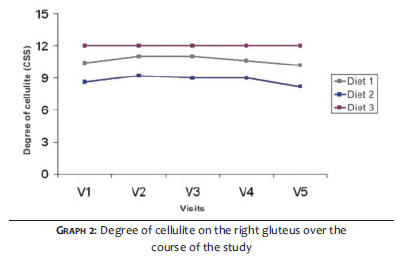
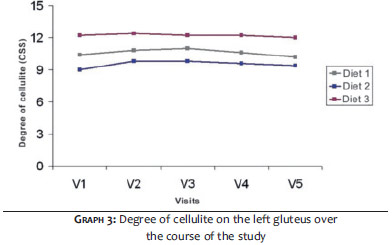
The patients who followed the diet with high-protein content (Diet 2) had lower average scores for the degree of cellulite (CSS) in the right and left buttocks, when compared to those who followed a low-carbohydrate diet (Diet 1) (p = 0.005 and p = 0.051, right and left buttocks, respectively) and the control diet (Diet 3) (p <0.001 and p = 0.007, right and left buttocks respectively). The degree of cellulite in patients who followed Diets 1 and 2 did not differ significantly from each other in the left and right buttocks (p = 0.080 and p = 0.142, respectively). There was no improvement in the degree of cellulite in the right and left buttocks over the course of the study for any of the diet types (Graphs 2 and 3).
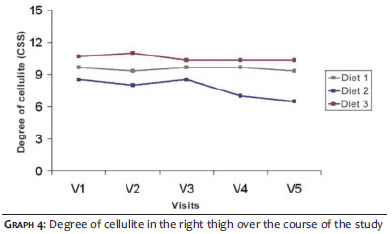
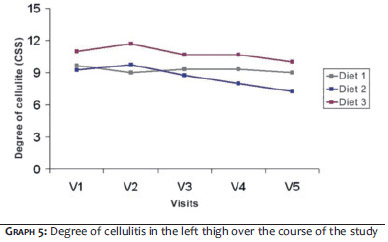
The patients who followed the diet with high-protein content (Diet 2) had a significantly lower degree of cellulite in the right thigh than those who followed a low-carbohydrate diet (Diet 1) in months 4 and 5, and than those who followed the control diet (Diet 3) in months 2, 4, and 5 (Graph 4). The patients who followed the diet low in carbohydrates (Diet 1) had a significantly lower degree of cellulite on the right and left thighs than those who followed the control diet (Diet 3): in month 2 for the right thigh and in months 2 and 5 for the left thigh. The group following the diet with high-protein content (Diet 2) showed an improved degree of cellulite on the right thigh (p = 0.014) and left thigh (p = 0.013) throughout the entire study period (Graphs 4 and 5).
This was the first study to examine the effects of a low-carbohydrate content diet and high-protein content diet on the degree of cellulite.
The patients' adherence rate was low, considering that less than half of those who started the study (44.2%) participated up to the last proposed assessment follow-up visit. This fact demonstrates the difficulty these patients had in following a diet, regardless of the proposed diet, given that there was a high dropout rate in all groups throughout the study. In general, patients' poor adherence in studies evaluating the outcome of diets is a known fact. 15 Adherence rate is influenced by various factors, such as level of education, self-care conditions, concern with one's own quality of life, socioeconomic factors, and psychological conditions. 16,17
The sample obtained was homogeneous regarding almost all demographics except for age, which differs between the diet Groups 2 and 3. Patients who received the diet with a high-protein content were older compared to those who received the control diet. That group's degree of cellulite, however, did not differ significantly from those of the other groups at baseline. Older patients can have a higher degree of cellulite than that of younger patients due to the sagging of skin, which tends to increase with age. 4,10,11
It was possible to observe that patients who followed the high-protein diet showed the greatest reduction in weight when compared with those who followed other diets. In diets high in protein, 25% of the total energy intake is composed of proteins. These diets are considered effective in producing satiety due to increased dietary thermogenesis and a subsequent decrease in food intake, and can aid in weight reduction. 18
Over time, a reduction was seen only in the degree of cellulite in the thigh, for patients who followed the diet with a high-protein content. Comparing the results of groups on each visit, it was possible to observe that these patients (Diet 2) had lower degrees of cellulite, particularly in the buttocks, when compared to patients who followed the other diets. The best effect of Diet 2 on the degree of cellulite can be related to the weight loss observed in this diet.
Lower levels of glucose, insulin, and glucagon production are attributed to the diet based on a reduced intake of carbohydrates. As a response, the body would produce oxidation of fatty acids with a corresponding result of the burning of fat stocks. 19 According to the literature, both diets low in carbohydrates and diets with reduced lipids promote weight loss. 20 Some studies 21,22 suggest that the storage of fats increases with higher concentrations of fat intake and decreases with diets low in lipid content. However, it is believed that a dietary plan low in carbohydrate content would be more effective in the long run than a diet with reduced lipid content. 20 It is possible that due to the lower thermal effect of fat and the higher energy expenditure required for the conversion of carbohydrates into fatty acids, fat is more easily stored than carbohydrates in adipose tissue.19 Nonetheless, in the present study the diet low in carbohydrate content had no significant effect on the patients' weight or degree of cellulite.
The degree of cellulite was evaluated using the CSS, 13 a scale validated for the objective evaluation of the degree of cellulite. This scale considers the morphological components of cellulite, such as the number of visible depressed lesions, the depth of the depressed lesions, the clinical appearance of elevated lesions, sagging, and the old classification. Each of these five items is assessed with a grade scale ranging from zero to three. The sum of all items results in the final value of the degree of cellulite, which can be classified as mild (1 to 5 points), moderate (6 to 10), or severe (11 to 15 points).
The high dropout rate of patients reduced the sample considerably, affecting the power of the study. A limitation of the present study is that although the nutritional monitoring of patients has been carried out, no validated assessment tool was used to evaluate the patients' adherence to the proposed diets. The initial difference in the average age between the groups could be identified as a possible selection bias, nonetheless all inclusions were randomized.
Despite the limitations, the authors believe they have conducted an original study of a little studied topic: the different types of diet and their effect on the improvement of cellulite, a highly prevalent aesthetic condition among women. This subject deserves further analysis in light of the data from a previous study conducted in the authors' dermatological center, in which patients with nutritional bulimic behavior were found in the sample. 23
Most of the patients studied had difficulty in following the proposed dietary regimen, regardless of the diet type. This was evidenced by the high dropout rate in the present study. The patients undergoing a diet high in protein content showed improvement in the degree of cellulite, probably related to weight loss and the resulting reduction in adipose tissue. Wider and more encompassing studies are necessary to establish the correlation between diet composition and the improvement of cellulite.
Although results are not relevant due to the small final sample, they allow for the suspicion that the reduction of body weight in patients with normal weight, independent of the specific diet type, may improve the degree of cellulite.
1. Brum C. Psychological Impact of Cellulite on the Affected Patients. In: Goldman MP, Hexsel D, editors. Cellulite: Pathophysiology and Treatment, 2nd edition. New York: Taylor & Francis; 2010. p. 5-7.
2. Hexsel D, Hexsel C, Weber M. Social impact of cellulite and its impact on quality of life. In: Goldman MP, Hexsel D, editors. Cellulite: Pathophysiology and Treatment, 2nd edition. New York: Taylor & Francis, 2010. p. 1-4.
3. Khan MH, Victor F, Rao B, Stadick NS. Treatment of cellulite: Part I. Pathophysiology. J Am Acad Dermatol. 2010;62(3):361-70; quiz 371-2.
4. Ortonne JP, Zartarian M, Verschoore M, Queille-Roussel C, Duteil L. Cellulite and skin ageing: is there any interaction. J Eur Acad Dermatol Venereol. 2008;22(7):827-34.
5. Hexsel DM, Abreu M, Rodrigues TC, Soirefmann M, do Prado DZ, Gamboa MM. Side-By-Side Comparison of Areas with and without Cellulite Depressions Using Magnetic Resonance Imaging. Dermatol Surg. 2009;35(10):1471-7.
6. Nurnberger F, Muller G. So-called cellulite: an invented disease. J Dermatol Surg Oncol. 1978;4(3):221-9.
7. Mirrashed F, Sharp JC, Krause V, Morgan J, Tomanek B. Pilot study of dermal and subcutaneous fat structures by MRI in individuals who differ in gender, BMI, and cellulite grading. Skin Res Technol. 2004;10(3):161-8.
8. Draelos ZD. The disease of cellulite. J Cosmet Dermatol. 2005;4(4):221-2.
9. Terranova F, Berardesca E, Maibach H. Cellulite: nature and aetiopatho-genesis. Int J Cosmet Sci. 2006;28(3):157-67.
10. Hexsel D, Siega C, Schilling-Souza J, Porto MD, Rodrigues TC. A comparative study of the anatomy of adipose tissue in areas with and without raised lesions of cellulite using magnetic resonance imaging. Dermatol Surg. 2013;39(12):1877-86.
11. Hexsel D, Dal'Forno T, Mazzuco R. Definition, clinical aspects, classifications, and diagnostic technique. In: Goldman MP, Hexsel D, eds. Cellulite: Pathophysiology and Treatment, 2nd edition. New York: Taylor & Francis; 2010. p. 13-23.
12. Smalls LK, Hicks M, Passeretti D, Gersin K, Kitzmiller WJ, Bakhsh A, et al. Effect of Weight Loss on Cellulite: Gynoid Lypodystrophy. Plast Reconstr Surg. 2006;118(2):510-6.
13. Hexsel DM, Dal'Forno T, Hexsel CL. A validated photonumeric cellulite severity scale. J Eur Acad Dermatol Venereol. 2009;23(5):523-8.
14. Frisancho AR. Anthropometric standard for the assessment of growth and nutritional status. Ann Arbor: The University of Michigan Press; 1990. p. 48-53.
15. Samaha FF, Iqbal N, Seshadri P, Chicano KL, Daily DA, McGrory J, et al. A low-carbohydrate as compared with a low-fat diet in severe obesity. N Engl J Med. 2009;360(9):859-73.
16. Chimenti BM, Bruno MLM, Nakasato M, Isosaki M. Estudo sobre adesão: fatores intervenientes na dieta hipocalórica de coronariopatas internados em um hospital público de São Paulo. Rev Bras Nutr Clin. 2006;21(3):204-10.
17. Kurita GP, Pimenta CAM. Adesão ao tratamento da dor crônica: estudo de variáveis demográficas, terapêuticas e psicossociais. Arq Neuro-Psiquiatr. 2003;61(2):416-25.
18. Halton TL, Hu FB. The Effects of High Protein Diets on Thermogenesis, Satiety and Weight Loss: A Critical Review. J Am Coll Nutr. 2004;23(5):373-385.
19. Polacow VO, Lancha J, Antonio H. Dietas hiperglicídicas: efeitos da substituição isoenergética de gordura por carboidratos sobre o metabolismo de lipídios, adiposidade corporal e sua associação com atividade física e com o risco de doença cardiovascular. Arq Bras Endocrinol Metab. 2007;51(3):389-400.
20. Last MD, Stephen A, Wilson MD. Low-Carbohydrate Diets. Am Fam Physician. 2006;73(11):1942-8.
21. Shai I, Schwarzfuchs D, Henkin Y, Shahar DR, Witkow S, Greenberg I, et al. Weight Loss with a Low-Carbohydrate, Mediterranean, or Low-Fat Diet. N Engl J Med. 2008;359(3):229-241.
22. Sacks FM, Bray GA, Carey VJ, Smith SR, Ryan DH, Anton SD, et al. Comparison of Weight-Loss Diets with Different Compositions of Fat, Protein, and Carbohydrates. N Engl J Med. 2009;360(9):859-73.
23. Hexsel DM, Siega C, Schilling-Souza J, Stapenhorst A, Rodrigues TC, Brum C. Avaliação dos aspectos psicológicos, psiquiátricos e comportamentais de pacientes com celulite: estudo-piloto. Surg Cosmet Dermatol. 2012;4(2):131-6.
The present study was carried out at the Centro Brasileiro de Estudos em Dermatologia, Porto Alegre (RS), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}