


Guilherme Muzy1; Elisete Isabel Crocco2; Renata Oliveira Alves3
Keywords: HIDRADENITIS SUPPURATIVA; THERAPEUTIC; LASER THERAPY.
Hidradenitis suppurativa (HS), also known as acne inversa or Verneuil disease, is a chronic inflammatory condition, recurrent and debilitating, with a pathogenesis linked to the chronic obstruction of the follicular portions of the pilosebaceous units. It is estimated that its prevalence ranges from 1-4%. 1,2 Previously identified risk factors are: family history (40% of patients have a relative with this diagnosis); 3 obesity (prevalence is higher than that in the general population); 4 smoking habits (more prevalent in patients with HS, it is believed that nicotine exerts immunological effects, such as neutrophil chemotaxis and obstruction of hair follicles); 5,6 use of drugs (especially in females using oral and injectable contraceptives containing levonorgestrel acetate and medroxyprogesterone). 7
Symptoms typically begin in the period after puberty and up to about 40 years of age, and is more common in women than in men (3.6:1), as described by a French retrospective observational study. 5,8 The clinical picture progresses with deep and inflammatory lesions at body sites that have apocrine glands, most commonly in the anorectal, axillary (Figures 1 and 2), inframammary (Figure 3), inguinal, and perineal regions. 9,10 These lesions begin as inflamed nodules, which can develop into fistulized and interconnected abscesses, with scarring, and pain, which is its main characteristic. 11 It is important to note that the pain picture, the foul odor of the secretions, and the scarring have a significant impact on patients' quality of life. The condition is prevalent in the population, and though therapeutic options are limited, the proper treatment of these patients is necessary due to the increased incidence of depression and sexual dysfunction in patients with HS. 12,13 Thus, due to its chronic nature and impact on patients' quality of life, proper handling of the condition is crucial.
The appropriate management of these patients is necessary due to the various psychological alterations that patients undergo 14 and the chronic nature of HS. Therefore, it is recommended that treatment addresses three fronts: reduction of the progression and extension of existing lesions and the prevention of new lesions; removal of bridges; and the reduction of scar formation.
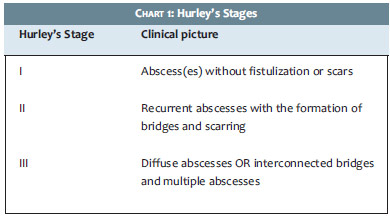
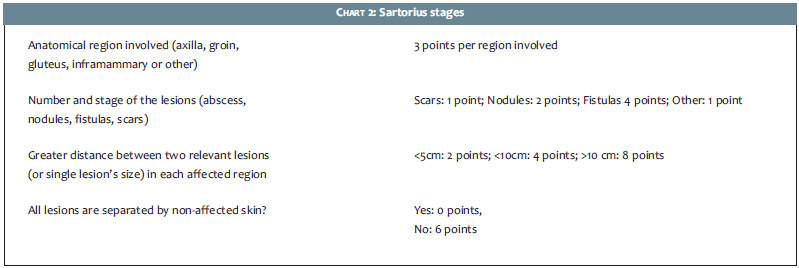
The initial approach for these patients depends on their classification according to the Hurley's staging system (Chart 1) 15, which helps in choosing the treatment modalities that will be used. The Sartorious' staging system is also used (Chart 2) for the monitoring of patients during the treatment.
Patients should be encouraged to stop smoking given the importance of this factor in the pathogenesis of HS. 16 Patients must also be encouraged to adopt a healthy lifestyle, with regular physical exercise and a healthy diet in order to reduce weight. 17
Antibiotics
Due to its broad pathogenesis, there are currently three therapeutic modalities for the management of patients: topical, systemic, and surgical treatments - including lasers in the latter case.
The use of antibiotics is adopted as an initial therapy in cases of early diagnosis of HS, with the combination rifampicinclindamycin being primarily used. The rationale behind this approach focuses on the fact that polymicrobial infections are associated with HS pictures, mainly due to their role of promoting inflammatory activity in the lesions 18 and to the formation of biofilm. 19 In a study carried out by Gener et al., 20 116 patients were treated with 300mg clindamycin and 300mg rifampicin twice daily, with 10 weeks of follow-up. It was possible to observe that there was a reduction in disease activity in the patients after the 10th week, with clinical improvement evidenced by a reduction in the patients' Sartorius staging system. Only 10 patients had adverse reactions to the treatment, with 6 of them choosing to withdraw due to intolerance to gastrointestinal symptoms (diarrhea, nausea, vomiting, and abdominal pain). In a retrospective study involving 34 patients, Zee et al. 21 studied different courses of rifampicin associated with clindamycin, and noted that the treatment's maximum effect takes place after 10 weeks. Of the 13 patients who had complete resolution of the condition, 8 reported recurrence of the clinical picture - these patients bore severe HS (Hurley'sStage III) at the beginning of the treatment.
Isotretinoin
Isotretinoin is a vitamin A derivative that is widely used for the treatment of acne vulgaris. Due to its inhibitory effects on sebum production, stimulation of keratinocytes differentiation, promotion of normalization of the cellular desquamation, 22 and excellent results in the treatment of this condition, some studies were carried out in order to determine the benefits of using this drug for HS.
In a retrospective study including 68 patients, Boers and Van Gemert 23 used isotretinoin as monotherapy, in 0.5 mg*day/kg doses during the first month, increasing to 1.0 mg*day/kg for at least 4 months. During the study's follow-up period (minimum of 4 and maximum of 6 months), the authors verified complete remission in 16 patients (23.5%), with 11 of those having maintained that response during an average follow-up period of 57 months.
Nevertheless, a retrospective study by Soria et al. 24 in which 88 patients used isotretinoin for treating HS showed that the treatment was ineffective. The patients used a variable daily dose of 23.0 mg/day to 65.0 mg/day for an average period of 7.8 months, and only 14 patients (16.1%) reported an improvement of symptoms, while 67 (77.0%) reported no change in symptoms, and 6 (6.9%) patients described worsening.
Dapsone
Dapsone is a competitive antagonist of para-aminobenzoic acid (Paba), which is used by bacteria in the synthesis of folic acid. Furthermore, it has anti-inflammatory properties that are not related to its antibacterial effect, and is thus used for the treatment of infectious and inflammatory dermatoses. Characteristically, conditions that respond well to this drug exhibit exuberant polymorphonuclear infiltrate in the affected tissue, with the neutrophils' products one of its main therapeutic targets. Due to the appearance of neutrophils in the later stages of HS lesions, its use was then investigated in this condition. 25
In a retrospective study by Yazdanyar et al. 26 24 patients with HS in different stages were treated with a daily monotherapy of 50mg to 200mg of dapsone (the majority took 100mg daily, for an average of 4.3 months). After the treatment, 6 patients showed significant clinical improvement, and 3 showed little improvement, with none of these having been initially classified as HS Hurley's Stage III. Sixteen patients did not improve after the treatment.
TNF-αinhibitors
In a double-blind, randomized placebo-controlled study published by Grant et al., 27 it was demonstrated that infliximab yields good results for the treatment of HS. For 8 weeks, 15 patients received 5 mg/kg doses of infliximab, following the application program at weeks 0, 2, 6 (a program already used for other inflammatory conditions, such as Crohn's disease and rheumatoid arthritis).28 The researchers found a significant reduction in the severity of HS in the study's patients, with reductions of up to 50% in the staging systems when compared to the beginning of treatment.
A systematic review by Alhusayen et al. 29 carried out in 2012, showed that this drug has enough evidence to be used in the treatment of HS. Nonetheless, due to its high cost and potential adverse effects, its use is recommended in patients with Hurley's Stages II or III, who have failed to achieve a significant improvement with the use of antibiotics and who have had a major impact on their quality of life. However, there is still a lack of large randomized studies to define the effectiveness of this approach in HS.
There are other drugs belonging in this class that are being studied, including adalimunab and etanercept. In the case of etanercept, a double-blind randomized placebo-controlled study was conducted by Adams et al., 30 where 20 patients were randomized to receive 50mg of etanercept or a placebo subcutaneously twice a week for 12 weeks. After that period, all patients received a new therapy course for 12 weeks. At the end of weeks 12 and 24, no significant improvement was seen in the patients. The adalimunab was evaluated in a phase 2 open study, in which 10 patients received 160mg adalimunab at week 0, followed by 80mg at week 1, with a weekly maintenance dose of 40mg for 12 weeks. Although the substance has been well tolerated and there have not been reports of serious adverse events, it was not possible to demonstrate a clinical improvement of patients. 31
Finasteride
Finasteride is an antiandrogen drug that exerts its effects through competitive inhibition of 5 alpha-reductase type II, which is responsible for converting testosterone to dihydrotestosterone (DHT) - its active metabolic enzyme. 32 Due to the fact that it mainly inhibits 5 alpha-reductase type II, which is present only in hair follicles, it is believed that this drug acts by decreasing the inflammatory response at that location.
In a 2005 study, Joseph et al. 33 followed up on the use of finasteride in 7 patients who had not shown any improvement after treatment with antibiotics. The patients were followed up with for a period varying from 8 to 24 months, using 5mg of the drug, with 6 of them having important clinical improvement, and 3 achieving complete remission.
A study published in JAMA by Randhawa et al., 34 investigated the use of this drug in 3 children, obtaining interesting results in terms of treatment, with 3 showing significant improvement. Nevertheless, due to the fact that the drug has a high risk of causing feminization in male fetuses, it should be used with caution in women of childbearing age, as is the case with isotretinoin.
Surgical therapy and lasers
Surgical therapies and laser-based techniques are employed in situations where treating lesions with other modalities has failed. Initially, surgical excision was carried out, however this method proved ineffective for large lesions due to the limited feasibility of the procedure. As a result, laser-based treatments have emerged as an interesting option due to the possibility of their use in extensive lesions and the conservation of healthy tissue around the lesions, eliminating the necessity of using surgical grafts or flaps.
The use of carbon dioxide laser has been addressed by Lapins et al. 35 in a series of 24 patients with Hurley's stage II who had already undergone HS treatments without success. This technique induces the vaporization of the lesions, as it is able to reach the deep layers of the subcutaneous adipose tissue and muscle fascia, making it useful for treating infected lesions due to the bactericidal effects of heat. Of the 24 patients, only 2 had recurrences in the treated sites, and 4 showed new lesions (5-10cm away from the treated sites).
In a similar study, Hazen and Hazen 36 used the CO2 laser technique in 61 patients with a total of 185 areas treated. Recurrence was observed in only 2 areas in the same patient during a follow-up period that ranged from 1 to 19 years.
Based on the role of hair follicles in the pathophysiology of HS, their selective ablation has emerged as an interesting option for controlling the disease. Among available treatments, 1,064nm Nd:YAG laser was evaluated by Tierney et al. 37 in a randomized controlled prospective study with 22 patients. Three monthly therapy sessions were carried out within half of each patient's body, and the results were compared with the other half, which had received topical treatment with antibiotics only. The results obtained showed significant improvement in all treated patients, with variations in the improvement in the Sartorius score (Chart 2), depending on the areas treated (73.4% for the inguinal region, 62.0% for the axilla, 53.1% for the inframammary region, resulting in an overall improvement of 65.3%).
Metformin
Metformin is an oral hypoglycemic drug that acts by reducing hepatic gluconeogenesis and insulin resistance. 38 It also presents antiplatelet and anti-inflammatory properties. 39 Given the association between polycystic ovary syndrome, HS and insulin resistance, there have been attempts to evaluate the drug's action in the treatment of this disease.
An open clinical trial was carried out with 25 patients, all bearers of HS (in all stages), who were initially treated with 500mg of metformin daily, with an increase in the dose to 1,000mg after one week and to 1,500mg after another week. After reaching the maximum dose of 1,500mg/day, patients used the medication continuously for 22 additional weeks and were evaluated at weeks 12 and 24 of the treatment. The degree of severity was reassessed at each consultation, and was initially calculated with the Sartorius system. The impact of the treatment was also assessed through the questionnaire Dermatology Life Quality Index.
Of the 25 patients, 18 (72%) had an average reduction of 12 points in the Sartorius system, with 7 of them having decreased by more than 50%. The 7 remaining patients (28%) had no response to the treatment. Regarding the quality of life questionnaire, 19 patients had improvement with a decrease in incidence rates of depression and absenteeism. However, further and more controlled clinical trials, with a greater number of patients, should be carried out in order to confirm the efficacy of metformin in HS, with its use being recommend in patients who have already tried other treatment modalities and do not wish to undergo surgical procedures.
Because it is a difficult to control disease, treatment for HS should be individualized. Initially, the patient must be closely examined in order to be rated according to the Hurley's staging system, and to have risk factors and associated conditions determined. It is important to bear in mind that this is a dynamic condition and treatments used in more advanced forms of HS can be recommended in the early stages, according to the dermatologist's evaluation.
Initially, Hurley's Stage I could be addressed with topical clindamycin, with the possibility of monthly 1,064nm Nd:YAG laser treatments being evaluated. 37
Hurley's Stage II could be initially treated with 300mg clindamycin in combination with 300mg rifampicin twice daily for 10 weeks, 20,21 with 1,064nm Nd:YAG laser being performed for 3 or 4 months, with monthly sessions. 37 At this stage, in the event that the patient presents intolerance or refractory, it could be valuable to institute treatment using biologic agents, with infliximab being the first choice due to its encouraging results.29 Finasteride, which is seldom used for HS, has only case reports, 33,34 however it seems to be an effective therapy - with or without association to the chosen antibiotic therapy - like metformin.
Hurley's Stage III can initially be addressed with the already mentioned therapies. However, excisional surgeries or CO2 based excision must be considered.
Many dilemmas and difficulties are involved in the treatment of HS, since it is a chronic disease with a significant impact on the quality of life of patients who have a poor response to the more usual therapies. Most of the more effective treatments, such as the use of lasers or biological products, are difficult for much of the population to access. It is important for dermatologists to master the surgical and clinical options of the different treatment modalities in order to be able to change the course for individual bearers of HS.
1. Alikhan A, Lynch PJ, Eisen DB. Hidradenitis suppurativa: a comprehensive review. J Am Acad Dermatol. 2009;60(4):539-61.
2. Jemec GB. Clinical practice. Hidradenitis suppurativa. N Engl J Med. 2012;366(2):158-64.
3. von der Werth JM, Williams HC. The natural history of hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2000;14(5):389-92.
4. Revuz JE, Canoui-Poitrine F, Wolkenstein P, Viallette C, Gabison G, Pouget F, et al. Prevalence and factors associated with hidradenitis suppurativa: results from two case-control studies. J Am Acad Dermatol. 2008;59(4):596-601.
5. Vazquez BG, Alikhan A, Weaver AL, Wetter DA, Davis MD. Incidence of hidradenitis suppurativa and associated factors: a population-based study of Olmsted County, Minnesota. J Invest Dermatol. 2013;133(1):97-103.
6. Sartorius K, Emtestam L, Jemec GB, Lapins J. Objective scoring of hidradenitis suppurativa reflecting the role of tobacco smoking and obesity. Br J Dermatol. 2009;161(4):831-9.
7. Revuz JE, Canoui-Poitrine F, Wolkenstein P, et al. Prevalence and factors associated with hidradenitis suppurativa: results from two case-control studies. J Am Acad Dermatol. 2008;59(4):596-601.
8. Canoui-Poitrine F, Le Thuaut A, Revuz JE, Viallette C, Gabison G, Poli F, et al. Identification of three hidradenitis suppurativa phenotypes: latent class analysis of a cross-sectional study. J Invest Dermatol. 2013;133(6):1506-11.
9. Nazary M, van der Zee HH, Prens EP, Folkerts G, Boer J. Pathogenesis and pharmacotherapy of Hidradenitis suppurativa. Eur J Pharmacol. 2011;672(1-3):1-8.
10. Danby FW, Jemec GB, Marsch WCh, von Laffert M. Preliminary findings suggest hidradenitis suppurativa may be due to defective follicular support. Br J Dermatol. 2013;168(5):1034-9.
11. Gniadecki R, Jemec GB. Lipid raft-enriched stem cell-like keratinocytes in the epidermis, hair follicles and sinus tracts in hidradenitis suppurativa. Exp Dermatol. 2004;13(6):361-3.
12. Kurek A, Peters EM, Chanwangpong A, Sabat R, Sterry W, Schneider-Burrus S. Profound disturbances of sexual health in patients with acne inversa. J Am Acad Dermatol. 2012;67(3):422-8.
13. Onderdijk AJ, van der Zee HH, Esmann S, Lophaven S, Dufour DN, Jemec GB, et al. Depression in patients with hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2013;27(4):473-8.
14. Wolkenstein P, Loundou A, Barrau K, Auquier P, Revuz J, Quality of Life Group of the French Society of Dermatology. Quality of life impairment in hidradenitis suppurativa: a study of 61 cases. J Am Acad Dermatol. 2007;56(4):621-3.
15. Sartorius K, Emtestam L, Jemec GB, Lapins J. Objective scoring of hidradenitis suppurativa reflecting the role of tobacco smoking and obesity. Br J Dermatol. 2009;161(4):831-9.
16. Simonart T. Hidradenitis suppurativa and smoking. J Am Acad Dermatol. 2010;62(1):149-50.
17. Danby FW, Margesson LJ. Hidradenitis suppurativa. Dermatol Clin. 2010;28(4):779-93.
18. van der Zee HH, van der Woude CJ, Florencia EF, Prens EP. Hidradenitis suppurativa and inflammatory bowel disease: are they associated? Results of a pilot study. Br J Dermatol. 2010;162(1):195-7.
19. Kathju S, Lasko LA, Stoodley P. Considering hidradenitis suppurativa as a bacterial biofilm disease. FEMS Immunol Med Microbiol. 2012;65(2):385-9.
20. Gener G, Canoui-Poitrine F, Revuz JE, Faye O, Poli F, Gabison G, et al. Combination therapy with clindamycin and rifampicin for hidradenitis suppurativa: a series of 116 consecutive patients. Dermatology. 2009;219(2):148-54.
21. van der Zee HH, Boer J, Prens EP, Jemec GB. The effect of combined treatment with oral clindamycin and oral rifampicin in patients with hidradenitis suppurativa. Dermatology. 2009;219(2):143-7.
22. Ward A, Brogden RN, Heel RC, Speight TM, Avery GS. Isotretinoin. A review of its pharmacological properties and therapeutic efficacy in acne and other skin disorders. Drugs. 1984;28(1):6-27.
23. Boer J, van Gemert MJ. Long-term results of isotretinoin in the treatment of 68 patients with hidradenitis suppurativa. J Am Acad Dermatol. 1999;40(1):73-6.
24. Soria A, Canoui-Poitrine F, Wolkenstein P, Poli F, Gabison G, Pouget F, et al. Absence of efficacy of oral isotretinoin in hidradenitis suppurativa: a retrospective study based on patients' outcome assessment. Dermatology. 2009;218(2):134-5.
25. Boer J, Weltevreden EF. Hidradenitis suppurativa or acne inversa: a clinicopathological study of early lesions. Br J Dermato.l 1996;135(5):721-5.
26. Yazdanyar S, Boer J, Ingvarsson G, Szepietowski JC, Jemec GB. Dapsone Therapy for Hidradenitis Suppurativa: A Series of 24 Patients. Dermatology. 2011;222(4):342-6.
27. Grant A, Gonzalez T, Montgomery MO, Cardenas V, Kerdel FA. Infliximab therapy for patientswith moderate to severe hidradenitis suppurativa: a randomized, doubleblind, placebo-controlled crossover trial. J Am Acad Dermatol. 2010;62(2):205-17.
28. Singh JA, Furst DE, Bharat A, Curtis JR, Kavanaugh AF, Kremer JM, et al. 2012 Update of the 2008 American College of Rheumatology Recommendations for the Use of Disease-Modifying Antirheumatic Drugs and Biologic Agents in the Treatment of Rheumatoid Arthritis. Arthritis Care Res (Hoboken). 2012;64(5):625-39.
29. Alhusayen R1, Shear NH. Pharmacologic interventions for hidradenites suppurativa: what does the evidence say?. Am J Clin Dermatol. 2012;13(5):283-91.
30. Adams DR, Yankura JA, Fogelberg AC, Anderson BE. Treatment of hidradenitis suppurativa with etanercept injection. Arch Dermatol. 2010;146(5):501-4.
31. Amano M, Grant A, Kerdel FA. A prospective open-label clinical trial of adalimumab for the treatment of hidradenitis suppurativa. Int J Dermatol. 2010;49(8):950-5.
32. Eicheler W, Dreher M, Hoffmann R, Happle R, Aumu¨ller G. Immunohistochemical evidence for differential distribution of 5 alpha-reductase isoenzymes in human skin. Br J Dermatol. 1995;133(3):371-36.
33. Joseph MA, Jayaseelan E, Ganapathi B, Stephen J. Hidradenitis suppurativa treated with finasteride. J Dermatolog Treat. 2005;16(2):75-8.
34. Randhawa HK, Hamilton J, Pope E. Finasteride for the Treatment of Hidradenitis Suppurativa in Children and Adolescents. JAMA Dermatol. 2013;149(6):732-5.
35. Lapins J, Marcusson JA, Emtestam L. Surgical treatment of chronic hidradenitis suppurativa: CO2 laser stripping-secondary intention technique. Br J Dermatol. 1994;131(4):551-6.
36. Hazen PG, Hazen BP. Hidradenitis suppurativa: successful treatment using carbon dioxide laser excision and marsupialization. Dermatol Surg. 2010;36(2):208-13.
37. Tierney E, Mahmoud BH, Hexsel C, Ozog D, Hamzavi I. Randomized control trial for the treatment of hidradenitis suppurativa with a neodymium-doped yttrium aluminium garnet laser. Dermatol Surg. 2009;35(8):1188-98.
38. Kirpichnikov D, McFarlane SI, Sowers JR. Metformin: an update. Ann Intern Med. 2002;137(1):25-33.
39. Grant PJ. Beneficial effects of metformin on haemostasis and vascular function in man. Diabetes Metab. 2003;29(4 PT 2): 6S44-52.
The present study was carried out at the Faculty of Ciências Médicas of Santa Casa de São Paulo – São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}