


Jules Rimet Borges1; Luiz Fernando Fróes Fleury Júnior2; Ana Maria Quinteiro Ribeiro3
Keywords: PREOPERATIVE CARE; ANTIBIOTIC PROPHYLAXIS; ANTICOAGULANTS; ELECTROSURGERY.
The pre-operative consultation is intended to assess the patient's state of health, in addition to clarifying details about the surgery and treatment options.1-4 During this consultation, the physician must gather information on the patient's full medical history, perform a physical examination, and explain the procedure to the patient.1-5 Moreover, taking photographs of the area to be operated on, and obtaining informed consent are desirable.2 Although about two-thirds of patients prefer to undergo preoperative consultation on the same day as the surgery, those with little education or previous surgical complications require that the pre-operative consultation be carried out on a different day.6
It is important to assess the history of the present illness, current medication, allergies, clinical and surgical medical antecedents, family history, and lifestyle habits.2
It is also crucial to investigate prevalent illnesses or those with potential for surgical complications, such as diabetes mellitus, arterial systemic hypertension, coronary disease, heart failure, liver and kidney disease, and psychiatric disorders. It is necessary to evaluate and verify both the presence of and management of those conditions,2 staying in contact with the assistant physician when necessary. The patient must also be questioned on the use of heart valves or orthopedic prostheses in order to implement prophylaxis for infection when indicated. Likewise, the patient has to be questioned on the use of implantable electronic devices, with which electrosurgery can interact. Pregnancy, in turn, requires some special care, which will be discussed later on.
Diabetes mellitus (DM) must be well controlled. If decompensated, treatment before surgery should be optimized. Cardiovascular disease, autonomic neuropathy, and immune deficiency are responsible for major surgical risk factors related to diabetes,7 those being infection and hypoglycemia. Strict control of DM reduces peri-operative morbidity and mortality with major surgeries.7 However, more recent studies - randomized and with a great number of patients - have shown that intensive control of DM increases mortality due to increased risk of hypoglycemia.8 Comparisons of intensive control (glycemia levels near normal) with conventional treatment have suggested that the risk of hypoglycemia is greatest in the first.
Nevertheless, other outcomes assessed (mortality, cardiovascular disease, and renal failure) did not differ between the two groups according to a systematic review of the Cochrane database.9 Some authors consider reasonable levels of glycemia less than or equal to 200 mg/dL during and after surgery.10 If the patient uses long-acting insulin, it is recommended that 50% of the dose be administered the morning of the surgery, with a mixed solution of glucose 5% and saline 0.9% administered during the procedure,1 checking capilary glycemia every hour.8 During surgery, the goal is to maintain a glycemic level between 100 and 200 mg/dL.8 Hypoglycemic agents with a short half-life should be suspended on the day of surgery. On the other hand, those with a long half-life - such as clorpropramida - must be suspended 48 hours before in order to avoid hypoglycemia, toxicity, and drug interactions.11 Classically, delayed wound healing has been associated with diabetes mellitus decompensation.1,2
In a prospective study carried out by Dixon JA et al.,12 the risk of infection in patients with DM (4.2%, 23/551) was higher compared with those without the disease (2%, 235/6673). However, there was no difference in the incidence of non-infectious surgical complications - including suture dehiscence - between the two groups.12 The combination of intravenous and subcutaneous insulin decreases the incidence of post-operative infections as compared with the use of intravenous insulin alone.8
In most cases, regional anesthesia should be preferred to general anesthesia in diabetic patients due to the increased risk of neurological deficit associated with the latter.10 Anesthetics with epinephrine should be used with caution due to the high prevalence of microangiopathy.1
Uncontrolled systemic arterial hypertension (HTN) increases the risk of bleeding during and after surgery.1,2 However, in a study with 924 patients, Penington observed increased risk of infections in patients using antihypertensive drugs after cutaneous excisions (odds ratio = 2.5, p = 0.006), however there was no statistical significance of the increase of post-operative bleeding.13 If the patient uses antihypertensives, they must be taken even on the day of surgery. It is recommended that the procedure be postponed if blood pressure levels are above 180x110 mm Hg.2
In patients with coronary heart disease, epinephrine may cause concern due to its vasoconstrictor and cardio stimulating effect.2 The patient should be evaluated by a cardiologist pre-operatively, and the dermatologic surgeon must be capable of recognizing complications during ambulatorial procedures, providing initial care in cases of angina. However, as dermatologic surgeries are mostly carried out in ambulatorial settings, they are considered of low surgical risk.14
Pain and anxiety can cause exacerbations of the clinical picture in patients with heart insufficiency.2 The dermatologic surgeon should be aware of this possibility.
The presence of coagulopathy should be evaluated, as decompensated liver disease may extend the prothrombin time. In addition, portal hypertension and hypersplenism as well as chronic Hepatitis C can lead to thrombocytopenia. It is also important to avoid hepatotoxic drugs in these patients.
Adjustment of doses of antimicrobial agents according to the patient's renal function must be carried out if needed.
Although bleeding is the main complication in dermatologic surgery,15 its incidence is low, occurring in fewer than 3% of cases.16,17 The level of desirable hemoglobin pre-operatively varies according to the patient's clinical picture. Young patients without cardiopulmonary diseases tolerate lower hemoglobin levels.4 It is important to assess whether the anemia is symptomatic (asthenia, palpitations, and fatigue on exertion, for example), as well as whether it may have systemic effects (tachycardia, dyspnea, impairment of general conditions). It is prudent to estimate the expected blood loss in the procedure in order to decide on the need for a pre-operative red blood cells.. It is important to note that the cause of anemia should never be neglected by the physician, who must refer the patient to the general practitioner or hematologist, if necessary.
Patients with unrealistic expectations about the outcome of surgery, or those reluctant to accept explanations from the doctor, are not good candidates for elective procedures. Excessive concern with small benign lesions or even imagined defects in one's appearance, with compromise to social or occupational relationships, can characterize body dysmorphic disorder. On the other hand, it can be part of other psychiatric pictures2 and requires referral to a specialist.
There are peculiarities regarding the age group of the patient. With children, it is important to await until he or she is emotionally able to undergo elective procedures. On the other hand, the elderly should not be excluded based exclusively on age.3 Clinical evaluation is essential, as well as the functional capacity of elderly patients. It is important to analyze the surgery's impact on their quality of life. A patient with advanced age and dementia, for instance, bearing a bleeding neoplastic lesion that has to be frequently manipulated due to his or her low cognitive ability, will mostly enjoy a positive leap in his or her quality of life with the excision of the lesion - provided that the surgical risk does not surmount those benefits.
Elective procedures should be postponed to the postpartum stage.
Lidocaine is safe in low doses (Class B).
Epinephrine is a class C drug; Silva3 cautions that it can be used in the first trimester rat low doses, and after the fifth month, without risk of decreased placental flow.3
Penicillin and erythromycin stearate are acceptable, provided that there is no hypersensitivity to such drugs.
There is a risk of reactivation of the herpes simplex virus after resurfacing with CO2 laser, dermabrasion, medium and deep peels, genital and oral surgery, and is also sometimes reported following Mohs micrographic surgery.18,19 The occurrence of herpetic infection after surgical/cosmiatric procedures exposing the dermis in patients with a history of viral infection can reach 50% to 70%. However, it can be reduced with prophylactic measures.19 There can also be a primary herpetic infection, although it is less common.19 (Table 1) In cases where there is dermal injury, involvement is more extensive than usual and there is an increased risk of secondary bacterial infection and scarring.19
Therefore, in cases using fractional lasers, dermabrasion, medium and deep peels, or application of fillers to increase perioral volume, antiviral prophylaxis is recommended in patients with a history of herpes simplex. The same should be done in cutaneous reconstruction after excision of neoplasia with extensive flaps (particularly in regions innervated by the second and third branches of the trigeminal nerve). In cases of resurfacing and full face or deep perioral peels, even if the personal history is negative, prophylaxis is recommended.
There are no standardized doses. There are treatments with 200mg of acyclovir five times per day and 400-800mg three times a day; Famciclovir 250-500mg twice daily and valaciclovir 500mg twice or three times per day.2,18,19 Whether a patient starts to take the drug one day before or on the morning of the procedure does not show different outcomes, and the time of use should continue until reepithelialization. The latter time period varies among patients, however it can last roughly seven to ten days, or less.19 During this period, contact with relatives who have active lesions should be avoided.19
Bacteremia after manipulation of the skin occurs in 38% of cases where a skin infection is present, and in 3% of cases where it is absent.20 There are only four reported cases of infective endocarditis after cutaneous surgery.20
The following characterize a high risk for developing infective endocarditis, according to the American Heart Association, in 2007:21 bearing a prosthetic heart valve, bearing valvular heart disease corrected with prosthetic material, having a history of infective endocarditis, acquired valvular heart disease in heart transplant patients, uncorrected cyanotic congenital heart disease, cyanotic congenital heart disease corrected but progressing with residual lesion, or cyanotic congenital heart disease corrected with prosthetic material. Prophylaxis is recommended for high-risk patients in surgical procedures involving the oral mucosa, respiratory tract, infected skin, skin structures, and musculoskeletal tissue.21 Local injection of an anesthetic into the oral mucosa does not require prophylaxis.20-23 A 2005 consensus24 cited in several dermatology books recommends prophylaxis of infective endocarditis also in cases of Mohs micrographic surgery in high-risk patients and in cases of excision of eroded skin in patients with prosthetic heart valves. Nonetheless, such guidelines are not upheldin more recent articles.20-23
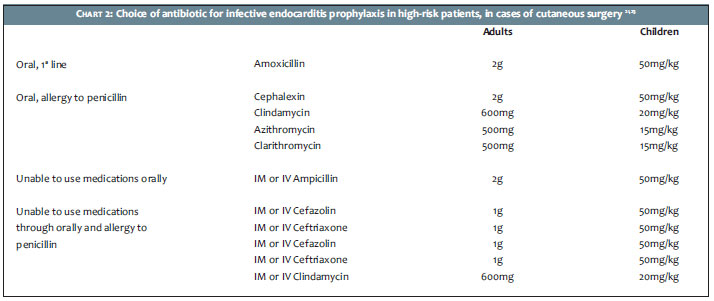
The antibiotic chosen in cases of dermatological surgery should cover Staphylococcus aureus, and beta hemolytic streptococci and, in the oral region, Streptococcus viridans.21 (Chart 2) In skin infected by Staphylococcus epidermidis, methicillin-resistant S. aureus (MRSA) or in cases of recently implanted prosthetic valves, there are recommendations in the literature for the use of 1g IV vancomycin for adults.23 The antibiotic should be administered 30-60 minutes prior to the procedure. In cases where it is not administered beforehand, it can be administered within two hours of the end of the procedure.23
Short duration procedures do not need a post-operative dose (the estimated time of bacteremia is only 15 minutes). If the surgery duration needs to be prolonged,half the initial dose is usually administered six hours after the procedure.23
It is important to highlight that amoxicillin, clindamycin, and azithromycin are classed as category B drugs for use during pregnancy, while clarithromycin and vancomycin are category C. The patient must be instructed on the fact that good oral hygiene is more important than antibiotic prophylaxis, given that bacteremia resulting from daily activities is more likely to cause infective endocarditis than the bacteremia associated with dental procedures, for example.21
In turn, the British Association of Dermatologists (BAD)20 states that antibiotic prophylaxis in cutaneous surgery is not routinely indicated, even in high-risk patients. Nonetheless, this guideline should be properly discussed with the patient's cardiologistpriorto the procedure.
The use of antibiotic prophylaxis is indicated in high-risk cases: prosthesis for less than two years (new or replacement), previous infection at the site of the prosthesis, hemophilia, immunosuppression (diabetes mellitus, AIDS, malnutrition, malignant neoplasias, use of immunosuppressive therapy), oral procedures involving bleeding, orpotentially contaminated orofacial procedures. The prevention of infection of the skin and soft tissues is important in patients who have already undergone total arthroplasty, since it represents the main sourceof delayed infectionatthe site of the prosthesis. The choice of the antibiotic is similar to that of the prevention of infective endocarditis.23
The rate of infection atthe surgical site in the presence of a clean surgical technique is very low (0.91%).25 Moreover, pre- and post-operative antibiotics increase both the cost and bacterial resistance in the community.26 Thus, the use of antibiotics for prophylaxis of infection atthe surgical site should be restricted. Bathing before surgery decreases the rate of infection.3
Trichotomy 24 hours before should be avoided (if necessary, trimming with scissors must be carried out in the operating room).3
The following are risk factors for the infection of the surgical site:3,22,23 location (below the kneeor on the lips, ears, or groin), smoking habits, immunosuppression (including diabetes mellitus), colonization.
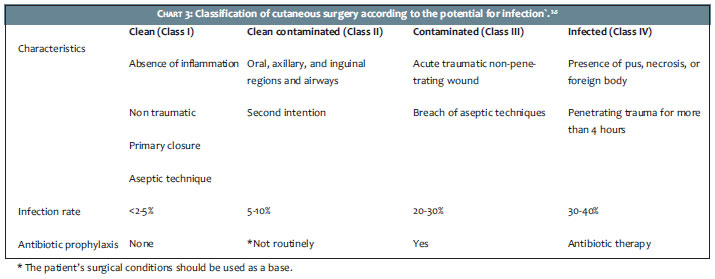
According to the likelihood of infection, cutaneous surgeries can be classified as: clean, clean-contaminated, contaminated, and infected. (Chart 3)3,5
The following are indications for antibiotic prophylaxis in dermatologic surgery:3
Flap or graft in the nose or ear;
Closure under tension;
Inflammation (class III) or infection (class IV) at the surgical site;
Multiple simultaneous procedures;
Procedures below the knee;
Surgery on the hands;
Decompensated diabetes mellitus;
Immunodeficiency
The choice of antibiotic is similar to that of endocarditis prevention. Oral 800/160 mg trimethoprim-sulfamethoxazole, 500mg ciprofloxacin and 500mg levofloxaxina 30-60 minutes before surgery are also options in cases of surgery on the ears, groin,or lower extremities (below the knee).23
Topical antibiotics are not more efficient in preventing wound infection27 than white petrolatum,24 besides increasing the risk of bacterial resistance in the community24,25 and that of contact dermatitis,24 and therefore should not be used for this purpose.24-27
Nonetheless, in a recent well-conducted study with 693 patients, topical decolonization with mupirocin in nasal carriers of S. aureus resulted in lower rates of surgical site infection than those caused by oral antibiotics after Mohs micrographic surgery.28
Implantable electronic devices include the following: heart pacemakers (PM), implantable cardioverter defibrillator (ICD), cochlear implants, deep brain stimulators, vagus nerve stimulators, sacral nerve stimulators, phrenic nerve stimulators, spinal cord stimulators, gastric pacemakers, and bone growth stimulators. Electrocautery is safe in patients with implantable electronic devices because the patient's body does not conduct electric current. Bipolar electrosurgery is safer than monopolar electrosurgery, because with the former the positive and the neutral electrodes are separated by a small space, limiting the flow of electric current.29,30 Electrosurgery should not be performed within 15cm of implantable cardiac devices.31Whenever possible it is important to connect the vessels.
In cochlear implant patients, monopolar electrosurgery is strictly forbidden as it may cause damage to the device, requiring its replacement, or necrosis of cells of the basilar membrane, thereby preventing reimplantation. Bipolar electrosurgery can be used while maintaining at least a 3cm distance between the electrodes and the implant; removing the external components.31
Deep brain, sacral nerve, and spinal cord stimulators, as well as gastric pacemakers, can be turned off prior to surgery. In the case of the vagus nerve stimulator, deactivation is not necessary. Regarding bone and phrenic nerve stimulators, there are no specific recommendations in the literature.31
Adrenaline
Among the contraindications to the use of adrenaline are: recent2 acute myocardial infarction, unstable angina, recent myocardial revascularization, refractory cardiac arrhythmia, uncontrolled hyperthyroidism. Drug interactions:2 monoamine oxidase inhibitors, tricyclic, phenothiazines, oxytocin, and beta-blockers.
Lidocaine
Among the medicaments that predispose toxicity to lidocaine are:2 amiodarone, cimetidine, and midazolam.
Immunosuppressants
Immunosuppressants predispose patients to infections and can lead to delayed healing.
The Brazilian Consensus on Psoriasis 201232 highlights that surgical reactions of patients using biological agents are not well established, however it recommends suspension for a period of at least two times the half life of the drug before elective procedures, since they could theoretically affect wound healing and hemostasis, thereby increasing the risk of post-operative infection. For patients with rheumatoid arthritis (RA) under treatment with anti-tumor necrosis factor (anti-TNF), an encompassing retrospective study33 noted that the continuation of biologicals was not a major risk factor for soft tissue infections postoperatively. On the other hand, a systematic review published in 201234 concluded that studies on the discontinuation of anti-TNF agents in RA patients undergoing elective orthopedic surgery are conflicting. Nevertheless, it is argued that because of the existence of records showing increased risk of infection with anti-TNF - especially in the skin and subcutaneous tissue - which may affect the healing process, current guidelines suggest such drugs be suspended before elective surgery and restarted in the immediate post-operative period in order to prevent the exacerbation of the basic disease.34
In patients with inflammatory bowel disease, anti-TNF agents do not increase the risk of post-operative complications, except when evaluating patients with Crohn's disease in isolation (excluding ulcerative colitis),35-39 in which there is an increased risk of post-operative infection,35-38 especially in sites distant from the operated area.36 Billioud et al. observed an increased risk of post-operative complications in patients with nonspecific inflammatory bowel disease.38
Regarding dermatological surgery, there isan absence of published data.
Beta Blockers
Malignant hypertension and bradycardia associated with adrenaline (alpha-adrenergic stimulation without beta-adrenergic stimulation) although uncommon, may occur.2
The indication for betablockers pre-operatively for the prevention of acute myocardial infarction is controversial, however it does not have major implications for dermatologic surgeries, since they have a low surgical risk due to the fact that they are mostly carried out in ambulatorial conditions. It is recommended that these drugs be continued in patients who have used it before the surgery.40
Isotretinoin
It imposes a risk of irregular healing, and it is preferable to postpone elective procedures for at least six months after discontinuing the use of this drug.2
Anticoagulants and antiplatelet agents
Although it occurs in a small portion of the procedures (0.89-3% of cases)16,17 and usually without long-term sequelae,16,41 bleeding is the most common complication in dermatologic surgery.
Bordeaux et al.16 observed that partial closures, flaps, warfarin, and clopidogrel are significantly associated with bleeding complications. A meta-analysis of articles from 1966 to 2005, published in 2008,17 found increased moderate to severe post-operative bleeding as compared to the control, associated with warfarin (OR = 6.69, CI = 95%, 3.03 - 14.7, p < 0.001) and acetylsalicylic acid - however without statistical significance regarding the latter.17 Nonetheless, despite the increased risk as compared to the control, the incidence of bleeding complications associated with warfarin in dermatologic surgery remained limited. Severe postoperative bleeding occurred in 5.7% of cases.17 This is due to the low rate of complications in cutaneous surgery in general.
Vitamin K antagonists (warfarin)
Despite the increased likelihood of peri-operative bleeding associated with this medicament,16,17 it is usually controlled with adequate hemostasis during surgery and does not require major post-operative care.16 The risk of thrombotic events with discontinuation of the drug varies from 1:278 to 1:11,500.20 Thus, the risk of cardiovascular events after discontinuation of the drug in the peri-operative outweighs the benefits of its suspension.16 It is considered safe to perform surgery if the INR is less than 315 - 3.5.16
Unfractionated heparin
Its interruption is not recommended in dermatological surgery.15
Acetylsalicylic acid (ASA)
Some factors increase the risk of peri-operative bleeding with ASA, among them are: age over 67 years, surgeries close to the ear region, and closure with flaps or grafts.15 The probability of bleeding is greater when combined with clopidogrel than with isolated ASA.42
It is recommended that the drug be suspended from 10 to 14 days before surgery and restarted 7 days after the procedure, in cases where the patient uses it for analgesic/anti-inflammatory purposes or primary prophylaxis of cardiovascular events.15,43 When ASA is indicated for secondary prevention, it should not be interrupted. This includes patients who have already had acute myocardial infarction or ischemic stroke.15,43
Thienopyridines
Thienopyridines are antiplatelet agent inhibitors of the adenosine diphosphate's receptor (ADP). This group is composed of: clopidogrel, ticlopidine, and prasugrel. The risk of bleeding with these drugs is greater when they are combined with other antithrombotics.16,41 The risk is higher with prasugrel.43
Some authors do not recommend suspending the drug pre-operatively.15 Others instruct patients to maintain it when under monotherapy. However, it is prudent not to undergo surgery before consulting with the prescriber physician in case there is an intention to combine it with other antithrombotics.43
Direct inhibitors of thrombin
The direct inhibitors of thrombin are: lepirudin, argatroban, and dabigatran. There are no data about lepirudin and argatroban in dermatologic surgery. And there are few reports of bleeding in dermatologic procedures in patients under the use of dabigatran.44,45 Although these are new drugs, it is recommended that their use be maintained before dermatological surgery.15,43,45 There should be heightened attention to bleeding complications in patients over 75 years of age, due to the increased risk of upper gastrointestinal hemorrhage in patients on dabigratan than with those on ASA.43
Indirect factor XA inhibitors (Fondaparinux)
Surgery should be postponed until the drug is discontinued or replaced by warfarin.43
Direct factor XA inhibitor (Rivaroxaban)
This drug requires further study. Surgery should be postponed until treatment is completed.43
Dipiradamol (phosphodiesterase inhibitor)
There is a lack of studies in minor surgeries. There is an absence of recommendation for discontinuation.15
Nonsteroidal antiinflammatory drugs (NSAIDs)
Should be suspended 3 to 5 days prior to surgery and reintroduced between 3 and 7 days after the procedure.15,16
Herbal medicines and other drugs with platelet antiaggregant action
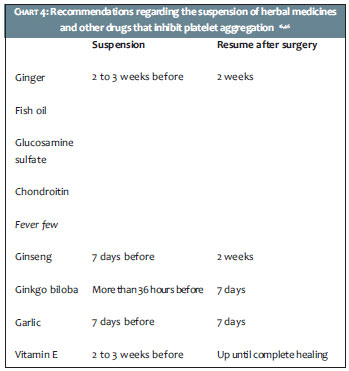
Ginger, fish oil (eicosapentaenoic acid), garlic, fever few, ginseng, ginkgo biloba, vitamin E, glucosamine sulfate and chondroitin have platelet anti-aggregant action and should be suspended before surgery.16,46 (Chart 4)
Capsaicin can decrease the concentration of factor VIII. Research on bleeding is inconsistent. The use of the drug should be suspended two weeks prior to surgery, and can be resumed two weeks after the procedure.46
Supplementary examinations should be requested pre-operatively according to the patient's clinical history and physical examination.40 There are numerous guidelines in the literature and many different protocols among dermatology services. A coagulogram is recommended in patients with a history of bleeding or with medical conditions that predispose to bleeding, as well as in patients taking anticoagulants.47 CBC is recommended for patients with diseases that increase the risk of anemia or who are at risk of peri-operative bleeding. Fasting glucose should be requested for patients at risk of undiagnosed diabetes mellitus. Renal function should be assessed in patients with chronic diseases or in use of medications that may alter or cause electrolyte disturbances. Chest radiography should be requested in patients who may have pulmonary complications during or after surgery. Patients with cardiovascular signs and symptoms should be evaluated with appropriate examinations.
The clinical history serves as a guide for a more appropriate pre-operative management, which does not need to be based on strict protocols, but rather on the overall assessment of the patient and the proposed surgery.
1. Pimentel E, Alves ACF, Alonso G. Avaliação clínica pré-operatória e indicação de antibióticos. In: Kadunc BV, Palermo E, Addor FAS, Metsavaht LO, Rabello L, Mattos R et al, editores. Tratado de Cirurgia Dermatológica, Cosmiatria e Laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2012.p.67-72.
2. Grandinetti LM, McGillis ST. Avaliação pré-operatória do paciente de cirurgia dermatológica. In: Vidimos AT, Ammirati CT, Poblete-Lopez C, editores. Requisitos em Dermatologia - Dermatologia Cirúrgica. Rio de Janeiro: Elsevier; 2010.p.73-80.
3. Silva SCMC. Avaliação pré-operatória. In: Silva SCMC. Cirurgia Dermatológica - Teoria e Prática. Rio de Janeiro: Di Livros; 2008.p.1-13.
4. Rocco JR, Fonseca ACC, Perez RM. Avaliação do risco cirúrgico e preparo pré-operatório. In: Vieira OM, Chaves CP, Manso JEF, Eulálio JMR, editores. Clínica cirúrgica: fundamentos teóricos e práticos. São Paulo: Atheneu; 2006.p.3-12.
5. Towsend CM, Beauchamp D, Evers M, Mattox KL. Princípios de pré-operatório e operatório. In: Towsend CM, Beauchamp D, Evers M, Mattox KL. Fundamentos de cirurgia. 17ª ed. Rio de Janeiro: Elsevier; 2005.p.123-31.
6. Sharon VR, Armstrong AW, Jim SC, Ibrahimi OA, Eisen DB. Separate- versus same-day preoperative consultation in dermatologic surgery: a patient-centered investigation in an academic practice. Dermatol Surg. 2013;39(2):240-7.
7. Kadoi Y. Perioperative considerations in diabetic patients. Curr Diabetes Rev. 2010;6(4):236-46.
8. Kadoi Y. Anesthetic considerations in diabetic patients. Part II: intraoperative and postoperative management of patients with diabetes mellitus. J Anesth. 2010;24(5):748-56.
9. Buchleitner AM, Martínez-Alonso M, Hernández M, Solà I, Mauricio D. Perioperative glycaemic control for diabetic patients undergoing surgery. Cochrane Database Syst Rev. 2012;9:CD007315.
10. Carles M, Raucoules-Aimé M. Prise en charge anesthésique du patient diabétique. Presse Med. 2011;40(6):587-95.
11. Kadoi Y. Anesthetic considerations in diabetic patients. Part I: preoperative considerations of patients with diabetes mellitus. J Anesth. 2010;24(5):739-47.
12. Dixon AJ, Dixon MP, Dixon JB. Prospective study of skin surgery in patients with and without known diabetes. Dermatol Surg. 2009;35(7):1035-40.
13. Penington A. Ulceration and antihypertensive use are risk factors for infection after skin lesion excision. ANZ J Surg. 2010;80(9):642-5.
14. Holt NF. Perioperative cardiac risk reduction. Am Fam Phys. 2012;85(3):239-46.
15. Henley J, Brewer JD. Newer hemostatic agents used in the practice of dermatologic surgery. Dermatol Res Pract. 2013;2013:279289
16. Bordeaux JS, Martires KJ, Goldberg D, Pattee SF, Fu P, Maloney ME. Prospective evaluation of dermatologic surgery complications including patients on multiple antiplatelet and anticoagulant medications. J Am Acad Dermatol. 2011;65(3):576-83.
17. Lewis KG, Dufresne RG. A meta-analysis of complications attributed to anticoagulation among patients following cutaneous surgery. Dermatol Surg. 2008;34(2):160-5.
18. Haik J, Weissman O, Stavrou D, Bem-noon HI, Liran A, Tessone A et al. Is prophylactic acyclovir treatment warranted for prevention of Herpes Simplex virus infections in facial burns? A review of the literature. J Burn Care Res. 2011;32(3):358-62.
19. Onwudiwe OC, Marmur ES, Cohen JL. Are we too cavalier about antiviral prophylaxis?. J Drugs Dermatol. 2013;12(2):199-205.
20. Child N, Anjum N, Keohane SG, Cooper HL. A guide to anticoagulation and endocarditis prophylaxis during cutaneous surgery. Clin Exp Dermatol. 2010;35(8):817-22.
21. Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, Levison M, et al. Prevention of Infective Endocarditis: Guidelines From the American Heart Association: A Guideline From the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007;116(15):1736-54.
22. Shurman DL, Benedetto AV. Antimicrobials in dermatologic surgery: Facts and controversies. Clin Dermatol. 2010;28(5):505-10.
23. Rossi AM, Mariwalla K. Prophylactic and empiric use of antibiotics in dermatologic surgery: a review of the literature and practical considerations. Dermatol. 2012;38(12):1898-1921.
24. Maragh SL, Otley CC, Roenigk RK, Phillips PK. Antibiotic prophylaxis in dermatologic surgery: updated guidelines. Dermatol Surg. 2005;31(1):83-93.
25. Morales-Burgos A, Loosemore MP, Goldberg LH. Postoperative wond care after dermatologic procedures: a comparasion of 2 commonly used petrolatum-based ointments. J Drugs Dermatol. 2013;12(2):163-4.
26. Rosengren H, Dixon A. Antibacterial prophylaxis in dermatologic surgery: an evidence-based review. Am J Clin Dermatol. 2010;11(1):35-44.
27. Levender MM, Davis SA, Kwatra SG, Williford PM, Feldman SR. Use of topical antibiotics as prophylaxis in clean dermatologic procedures. J Am Acad Dermatol. 2012;66(3):445-51.
28. Cherian P, Gunson T, Borchard K, Tai Y, Smith H, Vinciullo C. Oral antibiotics versus topical decolonization to prevent surgical site infection after Mohs micrographic surgery--a randomized, controlled trial. Dermatol Surg. 2013;39(10):1486-93.
29. Trindade MRM, Grazziotin RU, Grazziotin RU. Eletrocirurgia: sistemas mono e bipolar em cirurgia videolaparoscópica. Acta Cir Bras. 1998;13(1):1-17.
30. Martinez JC. Electrosurgery and implantable electronic devices. Dermatol Surg. 2011;37(7):900.
31. Voutsalath MA, Bichakjian CK, Pelosi F, Blum D, Johson TM, Farrehi PM. Electrosurgery and implantable electronic devices: review and implications for office-based procedures. Dermatol Surg. 2011;37(7):889-99.
32. Azulay-Abulafia L, Gripp A, Cursi IB, Felix PAO. Imunobiológicos. In: Maia CPA, Takahashi MDF, Romiti R, editores. Consenso Brasileiro de Psoríase 2012 - Guias de avaliação e tratamento - Sociedade Brasileira de Dermatologia. Rio de Janeiro: Sociedade Brasileira de Dermatologia; 2012. p.106.
33. den Broder AA, Creemers MC, Fransen J, de Jong E, de Rooii DJ, Wymenga A et al. Risk factors for surgical site infections and other complications in elective surgery in patients with special attention for antitumor necrosis fator: a large retrospective study. J Rheumatol. 2007;34(4):689-95.
34. Goh L, Jewell T, Laversuch C, Samanta A. Should anti-TNF therapy be discontinued in rheumatoid arthritis patients undergoing elective orthopaedic surgery? A systematic review of the evidence. Rheumatol Int. 2012;32(1):5-13.
35. Yang ZP, Hong L, Wu Q, Wu KC, Fan DM. Preoperative infliximab use and postoperative complications in Crohn's disease. A systematic review and meta-analysis. Int J Surg. 2011;12(3):224-30.
36. Kopylov V, Ben-Horin S, Zmora O, Eliakim R, Katz LH. Anti-tumor necrosis factor and postoperative complications in Crohn's disease: systematic review and meta-analysis. Inflamm Bowel Dis. 2012;18(2):2404-13.
37. Narula N, Charleton D, Marshall JK. Meta-analysis: peri-operative anti-TNFα treatment and post-operative complications in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2013;37(11):1057-64.
38. Billioud V, Ford AC, Tedesco ED, Colombel JF, Roblin X, Peyrin-Biroulet L. Preoperative use of anti-TNF therapy and postoperative complications in inflammatory bowel diseases: a meta-analysis. J Crohns Colitis. 2013;7(11):853-67.
39. Waterman M, Xu W, Dinani A, Steinhart AH, Croitoru K, Nguyen GC, et al. Preoperative biological therapy and short-term outcomes of abdominal surgery in patients with inflammatory bowel disease. Gut. 2013;62(3):387-94.
40. Feely MA, Collins CS, Daniels PR, Kebede EB, Jatoi A, Mauck KF. Preoperative testing before noncardiac surgery: guidelines and recommendations. Am Fam Physician. 2013;87(6):414-8.
41. Cook-Norris RH, Michaels JD, Weaver AL, Phillips PK, Brewer JD, Roenigk RK, et al. Complications of cutaneous surgery in patients taking clopidogrel-containing anticoagulation. J Am Acad Dermatol. 2011;65(3):584-91.
42. Shimizu I, Jellinek NJ, Dufresne RG, Li T, Devarajan K, Perlis C. Multiple antithrombotic agents increase the risk of postoperative hemorrhage in dermatologic surgery. J Am Acad Dermatol. 2008;58(5):810-6.
43. Callahan S, Goldsberry A, Kim G, Yoo S. The management of antithrombotic medication in skin surgery. Dermatol Surg. 2012;38(9):1417-26.
44. Fakhouri TM, Harmon CB. Hemorrhagic complications of direct thrombin inhibitors-subarachnoid hemorrhage during dermabrasion for scar revision. Dermatol Surg. 2013;39(9):1410-2.
45. Schmitt AR, Zender CA, Bordeaux JS. A new oral anticoagulant in the setting of dermatologic surgery. J Am Acad Dermatol. 2013;68(5):869-70.
46. Wong WW, Gabriel A, Maxwell GP, Gupta SC. Bleeding risks of herbal, homeopathic, and dietary supplements: a hidden nightmare for plastic surgeons?. Aesthet Surg J. 2012;32(3):332-46.
47. McGillicuddy EA, Maxfield MW, Salameh B, Stein LH, Ahmad U, Longo WE. Bleeding diatheses and preoperative screening. J Surg Educ. 2013;70(3)423-31.
The present study was carried out at the Universidade Federal de Goiás - Goiânia (GO), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}