


Daniele Bani1; Laura Calosi2; Lara Faggioli3
Keywords: HIGH-INTENSITY FOCUSED ULTRASOUND ABLATION; SKIN AGING; HISTOLOGY; DERMIS.
In aesthetic medicine, surgical lifting has long been the treatment of choice for facial skin laxity and rejuvenation purposes. In recent years, there has been an increasing demand for alternative noninvasive treatments that can overcome the drawbacks of surgery (1). The most promising and effective treatments are based on the principle that tissue tightening can be achieved through the delivery of controlled dermal heating, which in turn activates a controlled wound healing/collagen remodeling process resulting in dermal tightening (2-4). Chiefly, radiofrequency and laser light have been used to this aim, although with different degrees of success (5,6). The major shortcomings are modest clinical results, poor patient compliance-e.g. slow post-operative recovery and dyspigmentation upon laser treatments (6)-and the need for multiple treatment sessions to consolidate the improvements.
More recently, ultrasound-emitting instruments have been used to deliver thermal energy to the deep dermal connective tissue in addition to the superficial dermis, thus inducing more complete collagen remodeling than the previous methods (1,7). At present, ultrasound methodology is supported by clinical evidence indicating that, if properly executed, it can result in an appreciable and durable reduction of skin wrinkles due to ageing. Moreover, ultrasound treatments have negligible side effects, chiefly consisting in transient erythema, edema, and moderate pain, and therefore have excellent compliance with the treated patients (8-14).
The exact mechanisms that may explain the beneficial effects of ultrasound treatment are still a matter of investigation. It appears that ultrasound waves penetrate into tissue and cause vibration of the molecules at the site of the beam focus. The friction between tissue molecules produces focal overheating and thermal injury (15). Moreover, penetration depth can be modulated by wave frequency: the higher the frequency, the shallower the thermal effect on the dermis (1). Information on the structural changes induced by ultrasound treatment in skin tissues is scarce because of obvious ethical limitations with biopsy. Only in one study was a histologic examination performed before and 2 months after ultrasound treatment: this study showed increased dermal collagen with thickening of the dermis and straightening of elastic fibers (11). In fact, a detailed knowledge of the tissue/cell events underlying the positive clinical effects of ultrasound treatment on the skin, as well as of the possible noxious effects on the different skin tissue components (epidermis, dermis, subcutaneous fat pad), is currently lacking.
The present study was designed to investigate these issues. Using ex vivo full-thickness human skin samples, we aimed at evaluating and quantifying the histological changes directly induced by transcutaneous ultrasounds, delivered with different settings, on the various skin tissues, namely the epidermis, the papillary and reticular dermis, and the subcutaneous fat. The histological study was paralleled by evaluation of clinical efficacy for facial wrinkle reduction on 4 volunteers.
Ex vivo experiments
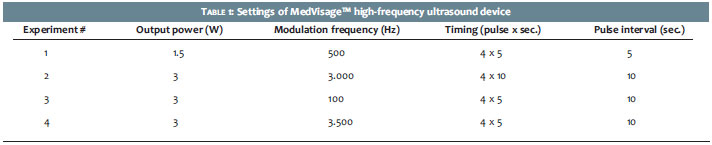
Tissue sampling and treatments-Abdominal full-thickness skin biopsies, approximately 10 mm thick and including the epidermis, dermis, and subcutaneous adipose tissue, were taken during surgical sessions for reductive abdominoplasty. The specimens were cut in two parts of similar size and weighed. Each specimen was placed in a Petri dish on ice, the subcutaneous tissue facing downwards, and combined with 2 ml of incubation medium (Dulbecco's modified Eagle medium, DMEM, Gibco Invitrogen, Milan, Italy). Treatments were performed using the MedVisageTM high-frequency ultrasound device (General Project Ltd., Montespertoli, Italy), which has been designed for skin-rejuvenating purposes. This instrument emits a main frequency of 5 MHz, which can be modulated between 10 Hz and 3.5 KHz. Multiple ultrasound pulses were delivered in continuous mode and were interspersed with pauses to prevent excessive tissue heating, considering the lack of intrinsic temperature homeostatic mechanisms in the blood flow-deprived tissue explants. Heating of the samples during the treatment was monitored and recorded using a thermocouple placed in contact with the bottom of the specimens. Four different instrument settings were used in 4 independent experiments, as described in Table 1. In a typical experiment, the emission plate of the MedVisageTM was placed in direct contact with the epidermis of a skin specimen through a thin layer of Aquasonic ClearTM ultrasound gel (Parker, Fairfield, USA). A parallel specimen was sham-treated (i.e. subjected to the same handling procedure but with no ultrasound emission) and used as control. After the treatments, fragments of skin tissue and subcutaneous fat from the treated and control specimens were cut, fixed in 4% glutaraldehyde in cacodylate buffer (0.1 M, pH 7.4), post-fixed in OsO4 in phosphate buffer (0.1 M, pH 7.4) dehydrated in graded acetone and embedded in epoxy resin (Epon 812, Fluka, Buchs, Switzerland) for light and electron microscopic studies. Others were fixed in 4% formaldehyde in a phosphate-buffer (0.1 M, pH 7.4), dehydrated in graded ethanol and embedded in paraffin for light microscopic analysis.
Morphometry of dermal collagen and elastic fibers-Histological sections, 6 mm thick, from formalin-fixed, paraffin-embedded specimens were stained with either anilin blue for collagen fibers, using a modified Azan staining method (16), or paraldehyde-fuchsin for elastic fibers. Digital photomicrographs of papillary and reticular dermis were separately taken under a light microscope equipped with x40 objective for papillary dermis (test area per microscopical field: 21,800 mm2) or x20 objective for reticular dermis (test area per microscopical field: 82,000 mm2) and an Eurekam 9 high-resolution video camera (BEL Engineering, Monza, Italy) interfaced with a PC by a dedicated software (BELview, BEL Engineering). From each specimen, 10 randomly chosen micrographs were collected. The overall surface area of collagen or elastic fibers per micrograph was measured using the free-share ImageJ 1.33 image analysis program (http://rsb.info.nih.gov/ij), upon setting an appropriate threshold to exclude the amorphous ground substance.
Morphometry of subcutaneous adipose cells-Digital photomicrographs of semi-thin sections, 2 mm thick, from glutaraldehyde/OsO4-fixed, Epon-embedded specimens were taken using the same light microscope, x20 objective and video camera as above. From each specimen, 5 randomly chosen micrographs (test area per microscopical field: 82,000 mm2) were collected. The cross-sectional surface area of adipocyte lipid vacuoles was measured using an ImageJ 1.33 program upon setting an appropriate threshold to include only the osmiophilic lipid vacuoles. Vacuolar profiles < 1,000 mm2, consistent with polar cross-sections, were discarded.
Ultrastructural analyses of skin tissues-Ultrathin sections, 800 nm thick, cut from glutaraldehyde/OsO4-fixed, Epon-embedded specimens were stained with aqueous uranyl acetate and alkaline bismuth subnitrate. They were viewed and photographed under a JEM 1010 transmission electron microscope (Jeol, Tokyo, Japan) equipped with a MegaView III high resolution digital camera and imaging software (Jeol). The different cell components of the epidermal and dermal tissue were examined in the control and ultrasound-treated samples (each group, n=3).
Clinical assay
Based on the data of the ex vivo experiments, we then aimed at testing the clinical efficacy of MedVisageTM for skin compaction using appropriate settings (ranges: 2-3 W, modulated frequency 2,000-3,000 Hz). The experiments complied with the guidelines of the Declaration of Helsinki, as amended in Edinburgh, 2008. Four healthy volunteers (3 males aged 45-51, 1 female aged 42), who gave written informed consent for their participation in the study, underwent a 5-minute session of facial rejuvenation. Prior to the treatment, macro photographs of details of the right periocular-zygomatic region were taken with a digital camera (Canon EOS) placed on a tripod. Distance from the target was measured with a laser meter. Fifteen minutes after the treatment, additional macro photographs from the same skin areas were taken under similar lighting and distance. The paired photographs were transformed with Adobe Photoshop CS4 using the filter sketch photocopy effect, which yielded a high contrast image of skin wrinkles and facilitated an examination of their length and thickness. The overall surface area of wrinkles before and after the treatment was then calculated using ImageJ 1.33 program after appropriate thresholding. Before performing morphometry, unwanted details that could have biased the measurements, such as hairs, eyelid profiles and nasolabial folds, were canceled from the images.
Statistics
Data were reported as mean values (± SEM) of the control and treated groups. Significance of differences was assessed by Student's t-test using Graph Pad Prism 4.03 statistical software (GraphPad, San Diego, CA, USA). p<0.05 was considered significant.
Ex vivo experiments
In a first experiment, the MedVisageTM was set at 1.5 W Power, 500 Hz modulated frequency, 4 ultrasound pulses (5 sec./5 sec. intervals). Visual examination of the aniline blue-stained histological sections showed that ultrasound treatment caused a slight increase in the density of collagen fiber framework in both the papillary and reticular dermis (Figure 1). Similarly, the paraldehyde-fuchsin-stained sections showed a modest increase in the density of elastic fibers, especially in the reticular dermis (Figure 1). Morphometric analysis confirmed the visual observations and showed that the differences did not reach statistical significance. Thermometric analysis of the skin specimens performed during each ultrasound application showed that their temperature remained low (subsequent values in ºC were: 18.0, 20.5, 25.2, 25.9, 28.0).
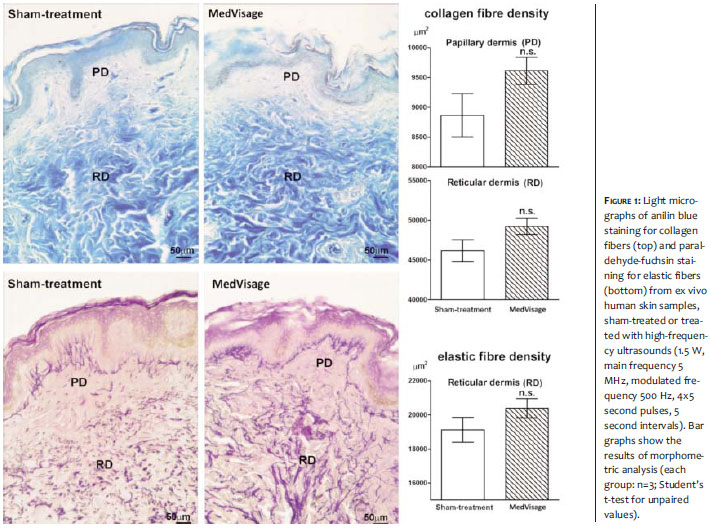
In a second experiment, the MedVisageTM was set at 3 W Power, 3,000 Hz modulated frequency, 4 ultrasound pulses (5 sec./10 sec. intervals). Visual examination of the aniline blue-stained sections showed that this treatment did not cause appreciable changes in collagen fiber density per microscopic field in the papillary dermis. Morphometric analysis confirmed that the differences were not statistically significant (Figure 2). On the other hand, a marked, statistically significant increase in the density of collagen fiber framework was found in the reticular dermis (Figure 2). Similarly, the paraldehyde-fuchsin-stained sections showed a statistically significant increase in the density of elastic fibers in the reticular dermis (Figure 2).
Robust clinical and histological evidence indicates that ultrasound delivery to the skin has liporeductive effects on the subcutaneous fat tissue, mainly ascribable to the induction of cavitation phenomena at the fat droplet/cytoplasmic interface of adipocytes (17-19). For this reason, we investigated whether the subcutaneous fat in the skin specimens was also affected by ultrasound treatment. Of note, no significant changes of the size of lipid vacuoles in the adipocytes were detected (Figure 2).
Thermometric analysis of the skin specimens performed during ultrasound delivery showed that the temperature remained below 50ºC, i.e. under the tissue damage threshold (subsequent values in ºC were: 18.9, 32.0, 41.0, 46.0, 50.9).
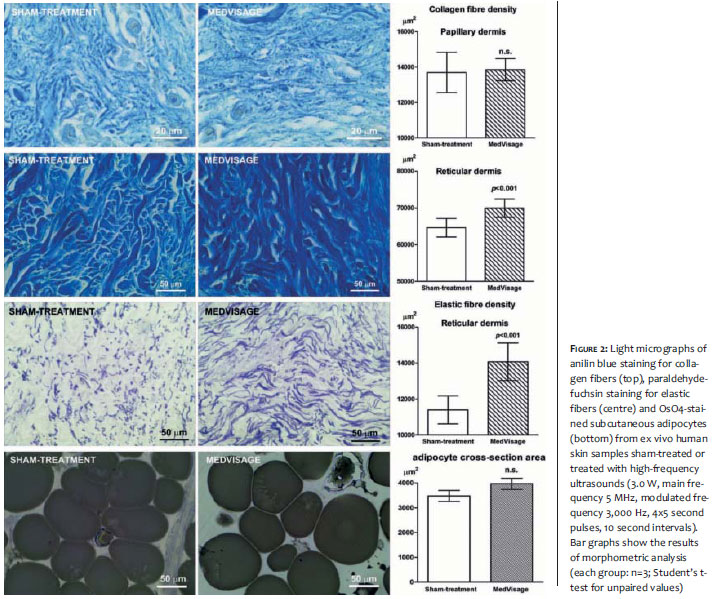
In a third experiment, the MedVisageTM was set at 3,0 W Power, 4 ultrasound pulses (5 sec./10 sec. intervals) and either 100 or 3,500 Hz modulated frequency. Examination of aniline blue-stained sections showed that the treatment with MedVisageTM set at 100 Hz caused a slight albeit significant increase in the density of the collagen fiber framework in both the papillary and reticular dermis (Figure 3). On the other hand, the treatment with the instrument set at 3,500 Hz caused a statistically significant increase in the collagen fiber density in the reticular but not the papillary dermis (Figure 3). At either modulated frequencies, no appreciable changes in the density of paraldehyde-fuchsin-stained elastic fibers were found in the papillary or reticular dermis (Figure 3), nor in the size of subcutaneous adipocytes (Figure 3).
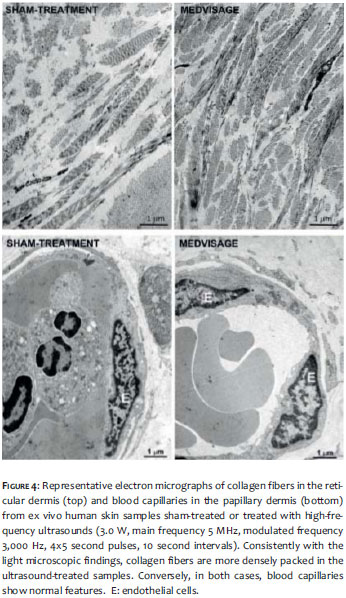
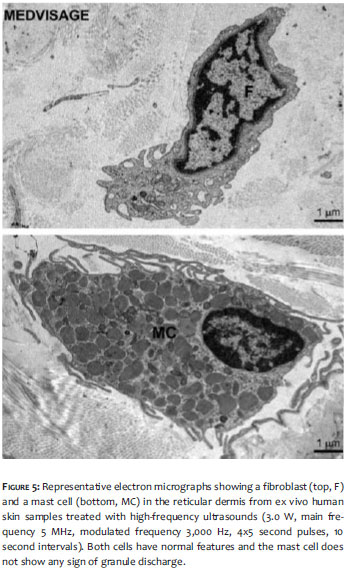
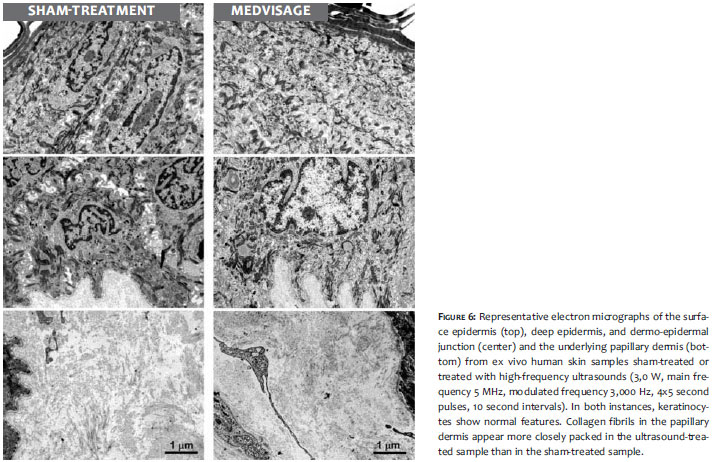
We next performed an ultrastructural analysis of sham-and MedVisageTM-treated skin specimens, using the instrumental setting that gave the most prominent effects, i.e. 3.0 W Power, 3,000 Hz modulated frequency, 4 ultrasound pulses (5 sec./10 sec. intervals). As expected from the light microscopical findings, the collagen framework in the reticular dermis appeared denser in the samples treated with MedVisageTM than in the sham-treated ones (Figure 4, upper panels). Conversely, no differences were observed in the morphology of dermal blood capillaries between the two experimental conditions (Figure 4, lower panels). In particular, endothelial cells show a normal organelle complement and no signs of cell damage. Dermal fibroblasts and perivascular mast cells in the treated samples also showed a normal ultrastructure, indicating that ultrasound treatment did not cause cell injury nor direct activation of mast cell granule release (Figure 5). Analysis of the epidermis and papillary dermis also indicated that MedVisageTM treatment did not induce any morphological abnormality that could be an index of cell injury (Figure 6). In particular, keratinocytes of the superficial and deep epidermal layers were similar in both groups, as was the overall appearance of the extracellular matrix and stromal cells in the papillary dermis.
Clinical assay
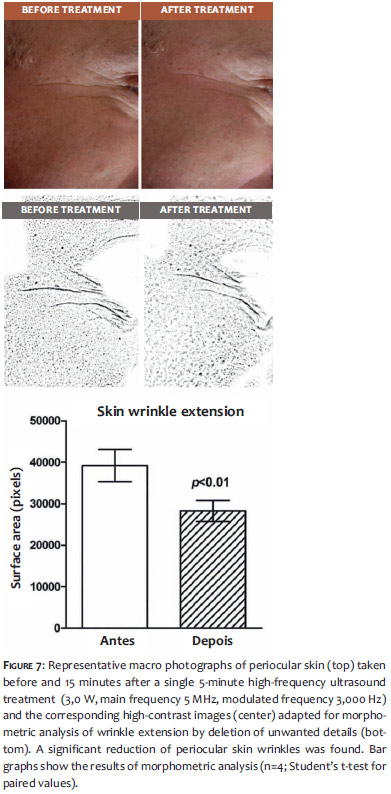
Finally, we evaluated the clinical efficacy on facial skin tightening of a single 5-minute ultrasound treatment, setting the MedVisageTM on a range of efficacy parameters deduced from the results of the ex-vivo experiments (2,0-3,0 W energy output, 500-3,500 Hz modulated frequency). Morphometric analysis of the same periocular skin areas performed before and after the treatment showed an appreciable, statistically significant reduction of skin wrinkles (Figure 7), ranging from 20.6-35.0% of the pre-treatment measurements. Moreover, the treated subjects reported no troublesome sensations during or after the treatment, especially with the higher modulation frequency settings.
In the present study we have evaluated the skin tightening efficacy of high frequency ultrasounds delivered by the MedVisageTM device, characterized by adjustable power output (set at 1.5-3.0 W), frequency modulation on a main frequency of 5 MHz (set at 100-3500 Hz), and pulse duration (set at 5-10 seconds for 4 repeated applications). With the tested instrument settings, an appreciable compaction of dermal connective tissue fibers was consistently observed, in keeping with previous reports (11). Of note, the overall effects varied depending on energy output and modulation frequency. In general, ultrasound energy transfer and biological effects seemed to be mainly exerted on the reticular dermis, in which the three-dimensional fiber framework showed the most evident increase in density, whereas less prominent changes occurred in the papillary dermis. When MedVisageTM was set at lower power output (1.5 W), the tightening effect on connective tissue fibers was slight and did not reach statistical significance, although it was evenly distributed in the papillary and reticular dermis. Instead, when MedVisageTM was set at a higher power output (3.0 W), a marked compaction of collagen and elastic fibers occurred, particularly in the reticular dermis.
Frequency modulation and pulse duration also appear to influence the results, especially the skin depth at which the effects are fully manifested. Taken together, the light microscopic findings from the different experiments suggest that MedVisageTM can be properly tuned to exert selective effects at different skin levels. The ultrastructural analysis confirmed that MedVisageTM could induce a compaction of dermal collagen fibers. Moreover, it offered evidence that high-frequency ultrasound treatment is safe and well tolerated by the skin tissues. In particular, epidermal keratinocytes, dermal fibroblasts, mast cells and endothelial cells of blood capillaries showed normal features, similarly to the sham-treated specimens, with no signs of cell injury such as mitochondrial swelling or plasma membrane rupture. Of note, perivascular mast cells did not appear to undergo cell activation and granule release, accounting for the absence of direct pro-inflammatory effects of ultrasound treatment. Measurement of tissue temperature by a probe placed at the bottom of the specimens, corresponding to the subcutaneous layer, indicated that, even upon repeated ultrasound applications lasting up to 10 seconds, the temperature did not exceed 50ºC, thus remaining below the thermal damage threshold. Of note, these values were reached in ex vivo explants, where the intrinsic thermoregulatory effect of blood circulation was not operating. Therefore, it can be assumed that actual skin warming in subjects undergoing MedVisageTM treatment may be substantially lower than in our experimental conditions.
Our findings provide new mechanistic insight into the clinical efficacy of high-frequency ultrasounds for skin tightening and rejuvenation purposes (1,8-14). In fact, dermal compaction was immediately achieved upon ultrasound delivery, i.e. before the occurrence of putative heat-induced focal wound healing/collagen remodeling processes that have been postulated to underlie the observed clinical effects (2-4). It can be postulated that this immediate effect of an ultrasound may result from the squeezing of interstitial fluids and the three-dimensional reorganization of the connective fiber meshwork. Conceivably, in the subjects treated for skin rejuvenation, focal wound healing and collagen remodeling may occur in a later phase, thereby providing an explanation for the reported long-lasting beneficial effects of ultrasound treatment (1,7).
Clinically, we observed that a single 5-minute treatment with MedVisageTM at similar energy output and frequency modulation as those used in the ex vivo experiments induced a rapid, objective reduction of the overall extension of facial skin wrinkles. The subjects perceived the treatment as comfortable and no side effects occurred. However, as this assay has been performed soon after ultrasound delivery, we cannot rule out that skin edema may have contributed to at least part of the noted wrinkle-reductive effects.
The present histo-morphometrical findings also indicate that the treatment of full-thickness skin explants with MedVisageTM at settings, which can induce dermal connective fiber compaction, did not cause appreciable changes of subcutaneous adipocytes. In fact, ultrasound-induced adipocyte cavitation has been demonstrated to cause destabilization of the adipocyte plasma membrane, focal ruptures of the adipocyte cytoplasm, and extracellular leakage of triglycerides (19,20). These effects account for the liporeductive properties of ultrasound-induced cavitation reported clinically. Conversely, MedVisageTM appears to be suited only for skin-tightening effects on the superficial skin layers, mainly the reticular dermis, with no risk of undesired liporeductive effects on the underlying subcutaneous fat pad. This is particularly important in view of the possible use of MedVisageTM on the skin of the face because, in this anatomical site, integrity of the subcutaneous fat tissue is mandatory for the best aesthetic results.
In conclusion, this study provides additional experimental and clinical evidence that high frequency ultrasounds are an effective and safe noninvasive technique for skin-tightening purposes in aesthetic medicine.
The authors gratefully acknowledge Professor Giancarlo Freschi and Dr. Giulia Lo Russo for kindly providing human skin samples.
1. McGregor JL, Tanzi EL. Microfocused ultrasound for skin tightening. Semin Cutan Med Surg. 2013;32(1):18-25.
2. Arnoczky SP, Aksan A. Thermal modification of connective tissues: Basic science considerations and clinical implications. J Am Acad Orthop Surg 2000;8(5):305-13.
3. Woolery-Lloyd H, Kammer JN. Skin tightening. Curr Probl Dermatol 2011;42:147-52.
4. Dobke MK, Hitchcock T, Misell L, Sasaki GH. Tissue restructuring by energy-based surgical tools. Clin Plast Surg. 2012;39(4)399-408.
5. Fitzpatrick RE, Rostan EF, Marchell N. Collagen tightening induced by carbon dioxide laser versus erbium:YAG laser. Lasers Surg Med. 2000;27(5):395-403.
6. Tanzi EL, Lupton JR, Alster TS. Lasers in dermatology: Four decades of progress. J Am Acad Dermatol. 2003;49(1):1-31.
7. Wilkinson TS. New perspectives in facial contouring using external ultrasonography. Clin Plast Surg. 2001;28(4):703-18.
8. Alster TS, Tanzi E. Improvement of neck and cheek laxity with a nonablative radiofrequency device: A lifting experience. Dermatol Surg. 2004;30(4pt 1):503-7.
9. Alam M, White LE, Martin N, Witherspoon J, Yoo S, West DP. Ultrasound tightening of facial and neck skin: a rater-blinded prospective cohort study. J Am Acad Dermatol. 2010;62(2):262-9.
10. Chan NP, Shek SY, Yu CS, Ho SG, Yeung CK, Chan HH. Safety study of transcutaneous focused ultrasound for non-invasive skin tightening in Asians. Lasers Surg Med. 2011;43(5):366-75.
11. Suh DH, Shin MK, Lee SJ, Rho JH, Lee MH, Kim NI, et al. Intense focused ultrasound tightening in Asian skin: clinical and pathologic results. Dermatol Surg. 2011;37(11):1595-602.
12. Lee HS, Jang WS, Cha YJ, Choi YH, Tak Y, Hwang E, et al. Multiple pass ultrasound tightening of skin laxity of the lower face and neck. Dermatol Surg. 2012;38(1):20-7.
13. Suh DH, Oh YJ, Lee SJ, Rho JH, Song KY, Kim NI, et al. A intense-focused ultrasound tightening for the treatment of infraorbital laxity. J Cosmet Laser Ther. 2012;14(6):290-5.
14. Fabi SG, Massaki A, Eimpunth S, Pogoda J, Goldman MP. Evaluation of micro-focused ultrasound with visualization for lifting, tightening, and wrinkle reduction of the décolletage. J Am Acad Dermatol. 2013;69(3):965-71.
15. White WM, Makin IR, Barthe PG, Slayton MH, Gliklich RE. Selective creation of thermal injury zones in the superficial musculoaponeurotic system using intense ultrasound therapy: A new target for noninvasive åfacial rejuvenation. Arch Facial Plast Surg. 2007;9(1):22-9.
16. Pini A, Shemesh R, Samuel CS, Bathgate RA, Zauberman A, Hermesh C, et al. Prevention of bleomycin induced pulmonary fibrosis by a novel anti-fibrotic peptide with relaxin like activity. J Pharmacol Exp Ther. 2010;335(3):589-99.
17. Zocchi ML. Clinical aspects of ultrasonic liposculpture. Perspect Plast Surg. 1993;7:153-74.
18. Brown SA, Greenbaum L, Shtukmaster S, Zadok Y, Ben-Ezra S, Kushkuley L. Characterization of nonthermal focused ultrasound for noninvasive selective fat cell disruption (lysis): Technical and preclinical assessment. Plast Reconstr Surg. 2009;124(1):92-101.
19. Bani D, Quattrini Li A, Freschi G, Lo Russo G. Histological and ultrastructural effects of ultrasound-induced cavitation on human skin adipose tissue. Plast Reconstr Surg Glob Open. 2013;1:e41;.
20. Garcia O Jr, Schafer M. The effects of nonfocused external ultrasound on tissue temperature and adipocyte morphology. Aesthetic Surg J. 2012;33(1):117-27.
The present study was carried out at the Department of Clinical and Experimental Medicine, Anatomy and Histology Sector, University of Florence - Florence, Italy; and at the Department of Research and Development, General Project Ltd., Montespertoli (Florence), Italy.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}