


Flávia Alvim Sant'Anna Addor1; Patricia Camarano Pinto Bombarda2; Mario Sergio Bombarda Júnior3; Felipe Fernandes de Abreu4
Keywords: ALOPECIA; NUTRIENTS; HAIR.
Described in 1961 by Albert Kligman, Telogen Effluvium (TE) is one of the most frequent etiologies of non-scarring alopecia.1
It manifests as diffuse hair loss due to some stimulus that alters the hair cycle, causing the acceleration of the anagen phase into the telogen phase (telogenization). This phenomenon alters the ratio of hair present between the two phases, leading to significant losses in relatively short intervals, causing great aesthetic displeasure to the patient.2
Nutritional deficiencies - such as protein, iron,2 and biotin3 deficiencies, which are important elements in the synthesis and quality of the hair fiber - are among the most relevant factors in the genesis of TE. Nutritional supplementation can be promising in conditions where the presence of TE is linked to eating disorders, such as malabsorption, diets for weight loss, etc. Other etiological factors described, such as childbirth and systemic diseases, may produce a deficit of certain nutrients, leading to a worsening of the alopecic picture. The present study evaluated the use of nutritional supplements in monotherapy in the treatment of TE, independent of its etiology.
To investigate the effect of a nutritional supplement commercially known as Exímia Fortalize® (Laboratório Farmoquímica S/A - Rio de Janeiro, Brazil) in improving the signs and symptoms of TE through clinical assessment and phototrichogram (TrichoScan® PhotoFinder dermoscope - FotoFinder Systems GmbH, Bad Birnbach, Germany).
The present study was conducted after ethical approval (CAEE: 13216113.7.0000.5514 of 18 February 2013). Following recruitment, all volunteers received a detailed explanation of the study and were fully informed about the Free and Informed Term of Consent approved by the Research Ethics Committee.
A prospective, randomized, blinded study analyzed 60 female patients (aged 18-60 years), with complaints of hair loss for at least one month, according to the inclusion and exclusion criteria, during the year of 2013, at the Clinical Research Laboratory of the Dermatology Department - Medcin Instituto da Pele (Osasco, São Paulo, Brazil).
All patients underwent dermatological examination for the clinical verification of TE with at least a one-month history, however without having undergone any related treatment or medication for the 3 months prior to inclusion in the study.
Patients with diffuse alopecia, active endocrine diseases, systemic diseases, going through a post-surgery period, pregnant or lactating, were excluded. Those who were using drugs with a potential for interference in the hair cycle, such as antineoplastic and corticosteroids, were also excluded.
After verification of inclusion and exclusion criteria, all patients underwent the first phase of the digital phototrichogram examination. This examination was conducted in two steps:
- Initial: standardized shaving of hair in the frontoparietal region in preparation for photographic documentation with 20X magnification dermatoscopic lens. This photograph was appropriately archived.
A macro photographic record was carried out in the area being evaluated. This record allowed for the identification of the evaluated area on subsequent visits.
- 48 hours after: a new photograph of the same area was taken with previous dying of hairs with an appropriate substance for this purpose. An evaluation with the TrichoScan® PhotoFinder dermoscope® device (Tricholog GmbH & Datinf GmbH, Germany) was carried out.
This equipment employs imaging software that determines:
anagen hairs: indicates the percentage of hairs in the growth stage;
Next, the patients carried out a subjective evaluation of the intensity of the perceived hair loss, attributing scores from zero (meaning "absence of hair loss") to three ("presence of intense hair loss").
After the collection of the data, the product was provided and the patients were instructed to take 1 tablet a day for six months.
The evaluated product had the following composition: 5mg calcium pantothenate (vitamin B5), 130mg magnesium, 45mg ascorbic acid (vitamin C), 7mg iron, 10mg vitamin E, 16mg nicotinamide (vitamin B3), 3.5mg Zinc, 600mcgRE beta carotene (vitamin A), 2.4mcg cyanocobalamin (vitamin B12), 1.2mg thiamine (vitamin B1); 1.3mg pyridoxine (vitamin B6), 1.3mg riboflavin (Vitamin B2), 240mcg folic acid and 30mcg biotin.
Patients were evaluated after 90 and 180 days, with new images being taken with the TrichoScan® device. At the same intervals, the patients answered the questionnaire about the perceived intensity of hair loss - exactly as they had done in the initial visit.
The success of treatment was measured in the final evaluation through a subjective questionnaire with a scale that ranged from 1 (meaning a "very good" outcome) to 5 (meaning "very bad" outcome). Both the evaluator physician and the patient answered this questionnaire.
The treatment was compared at each of the evaluation's experimental intervalsthrough the Student's t-test.
Of the 60 patients included in the study, 51 completed the evaluations and had their data analyzed. Withdrawals from the study occurred due to loss of follow-up or lack of adherence to the treatment - none were motivated by any reported or observed discomfort or adverse effects.
The product was well tolerated. Three patients reported adverse events: seborrheic dermatitis, anxiety, and migraine - which, however, were not deemed as serious correlated to the use of the product.
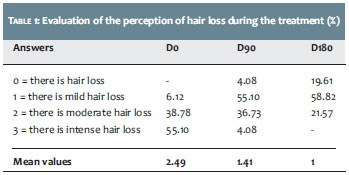
1. Subjective questionnaire on the perception of hair loss
At baseline, around 6% of the volunteers were considered to have mild hair loss, 39% with moderate hair loss, and 55% with intense hair loss. At the end of the study, 20% were considered not to suffer from hair loss, 59% had mild hair loss, 22% had moderate hair loss, and 0% intense hair loss. These results are depicted in Table 1.
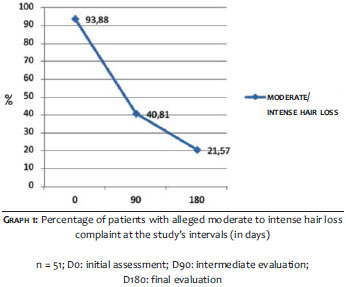
It is possible to observe a reduction to 21.57% from 93.88% of patients complaining of moderate to intense hair loss, suggesting there was an improvement of 72.31% regarding hair loss, as shown in Graph 1.
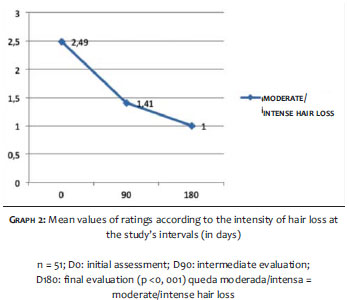
When analyzing the average performance of the product at the final visit as compared with the baseline, it was possible to verify that the mean ratings fell from 2.49 to 1.00, showing there was an improvement of 59.84% regarding hair loss, as shown in Graph 2. Such data were subjected to the Student's t-test, which indicated a statistical significance at both intervals, with p <0.001. There was a significant reduction in the moderate and intense hair loss ratings during the study period.
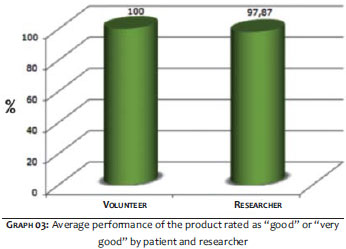
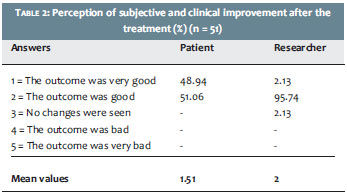
2. Subjective questionnaire on the perception of improvement
Regarding the perception of improvement evaluated 180 days after the treatment through a subjective questionnaire, the data showed clinical improvement, observed by 97.8% of researchers. In the subjective evaluation, 100% of volunteers noticed improvement, as shown in Graph 3. Table 2 shows in detail the levels of improvement observed.
3. Instrumental evaluation through the TrichoScan® device
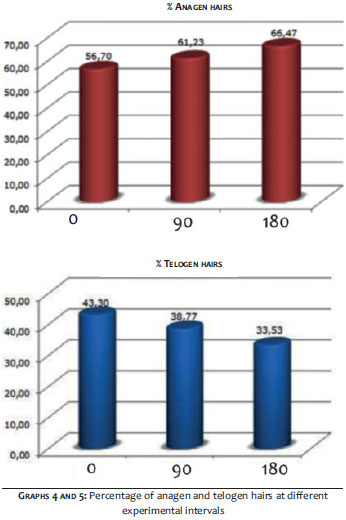
The percentage of hairs in the telogenic and anagenic stages was determined at each experimental interval, with their mean values evaluated statistically through the Student's t-test, as shown in Table 3.
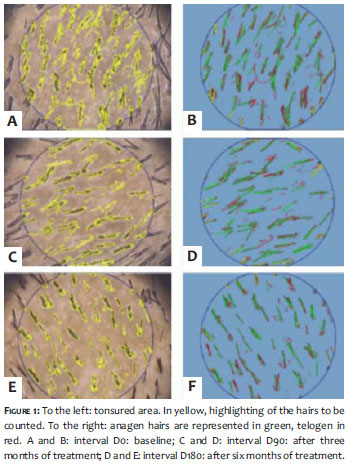
There was significant improvement, evidenced by a 10% reduction in telogenichairs (dormant stage) and an 8% increase in anagenic hairs (growth stage) in 90 days. This reduction in telogenic hairs and increase in anagenic hairs continued progressively for 180 days (22. 6% and 17.2% respectively). (Graphs 4 and 5) Figure 1 represent images collected by TrichoScan®, a reduction in telogenic hairs is perceived and is represented in red.
Telogen effluvium is one of the most frequent causes of alopecia seen in medical practice. Its occurrence is common at any age, and some factors, such as systemic disease, postpartum, emotional stress, and nutritional deficiency, as described in the literature, are strongly associated with its onset.4-6
However, about one third of cases remain without clear etiology.7
During the last decade, studies of the nutritional profile and specific nutritional deficiencies have demonstrated a higher than previously thought correlation with the condition's etiology and the worsening of dermatoses. The deficiency of trace elements, such as iron and zinc, has been demonstrated to cause or aggravate telogen effluvium. A recent study has demonstrated that zinc levels were significantly lower in a group of 320 patients with TE.8
Zinc is involved in the synthesis of proteins and nucleic acids, and has an important role in several metabolic routs and cellular functions. Specifically in the hair follicle, zinc is a powerful inhibitor of the hair follicle's regression in animal models.8,9 Likewise, iron plays a fundamental role in the nutrition of the hair follicle and women with iron deficiency are at risk of hair loss with telogenization.10
Vitamins such as ascorbic acid, folic acid, vitamin E and biotin also exert direct or indirect roles in the hair cycle for they act on metabolic processes involving protein synthesis or hormone expression, or are synergistic with other trace elements, such as zinc and vitamin C.11-13
Of the nutrients studied in alopecia, biotin has shown particular importance. The presence of a link between biotin deficiency and the loss of hair and body hair is a known fact.14
Biotin is a water-soluble vitamin that acts as an essential cofactor for carboxylases, being also responsible for catalyzing essential steps in cell metabolism, in addition to interfering in the differentiation of epidermal cells.15
Biotin supplementation improves the quality of keratin in the hair of animal models, even in the absence of apparent deficiency.16
In diffuse hair loss associated with telogen effluvium, the combination of biotin and zinc was studied with favorable results.17
Ironically, "modern" eating habits aimed at losing weight and at "detoxifying" can greatly reduce the intake of nutritious foods, with borderline deficiencies being capable of leading to pictures of progressive however slower developing alopecia.
From a practical point of view, it is important that the dermatologist remember to evaluate the patient's dietary profile, especially in cases that do not respond to traditional treatments.
Mild and occasional nutritional deficiencies, sometimes hardly detectable in routine laboratory tests, can be responsible for the low level of response to pharmacological therapy.18-20
Diagnosis and monitoring of TE are sometimes hampered, especially in chronic states, because the improvement is slow and often imperceptible in the early months. In the same way that the picture settles in insidiously, consistent results may require months to emerge. Although TE is self-limited, treatment or removal of the inducing factor leads to resolution within three to six months, while if left untreated, the prognosis is 3 to 10 years for a spontaneous resolution.17
For a more accurate and noninvasive quantitative assessment of this development, the phototrichogram rendered by the TrichoScan® device allows a hair count, while its morphological analysis recognizes anagen and telogen hairs through the combination of epiluminiscence microscopy and digital automatic image analysis.21, 22
As there is no specific treatment for TE, the empirical use of minoxidil has already been suggested in the literature, nevertheless there are no clinical studies to prove its effectiveness.23
Likewise, there are no studies on TE with nutrients at the recommended daily intake (RDI) and its combined use - in which the ingredients would act synergistically - have been poorly studied.24, 25
Data obtained in the present study demonstrate that, in idiopathic TE, the supplementation of a specific set of nutrients can lead to a significant improvement of the picture from the first quarter of use, at RDI doses, which makes them safer for prolonged use.
TE is a chronic alopecia disease, whose etiology is often difficult to establish. In such cases, micronutrient deficiencies at minimum levels should always be considered. The present study has demonstrated that in cases of TE with no apparent cause, nutrient replenishment related to the hair cycle shows significant benefit in the regression of the picture as early as after three months of treatment.
1. Verma SB. Albert Kligman, also a hair man. Int J Trichology. 2010;2(1):69
2. Whiting DA. Disorders of hair. ACP Medicine. 2006;1-8.
3. Pawlowski A, Wojciech P, Kostanecki W. Effect of biotin on hair roots and sebum excretion in females with diffuse alopecia]. Przegl Dermatol. 1965;52(3):265-9.
4. Mulinari-Brenner F, Bergfeld W. Entendendo o Eflúvio Telógeno. An Bras Dermatol. 2002;77(1):87-94.
5. Shapiro J, Wiseman M, Lui H. Practical management of hair loss. Can Fam Physician. 2000;46:1469-77.
6. Grover C, Khurana A. Telogen effluvium. Indian J Dermatol Venereol Leprol. 2013;79(5):591-603.
7. Harrison S, Sinclair R. Telogen effluvium. Clin Exp Dermatol. 2002;27(5):389-95.
8. Kil MS, Kim CW, Kim SS. Analysis of serum zinc and copper concentrations in hair loss. Ann Dermatol. 2013;25(4):405-9.
9. Plonka PM, Handjiski B, Popik M, Michalczyk D, Paus R. Zinc as an ambivalent but potent modulator of murine hair growth in vivo-preliminary observations. Exp Dermatol. 2005;14(11):844-53.
10. Moeinvaziri M, Mansoori P, Holakooee K, Safaee Naraghi Z, Abbasi A. Iron status in diffuse telogen hair loss among women. Acta Dermatovenerol Croat. 2009;17(4):279-84.
11. Kwack MH, Ahn JS, Kim MK, Kim JC, Sung YK. Preventable effect of L-threonate, an ascorbate metabolite, on androgen-driven balding via repression of dihydrotestosterone-induced dickkopf-1 expression in human hair dermal papilla cells. BMB Rep. 2010;43(10):688-92.
12. Daniells S, Hardy G. Hair loss in long-term or home parenteral nutrition: are micronutrient deficiencies to blame? Curr Opin Clin Nutr Metab Care. 2010;13(6):690-7.
13. Finner AM. Nutrition and hair: deficiencies and supplements. Dermatol Clin. 2013;31(1):167-72.
14. Yazbeck N, Muwakkit S, Abboud M, Saab R. Zinc and biotin deficiencies after pancreaticoduodenectomy. Acta Gastroenterol Belg. 2010;73(2):283-6.
15. Mock DM. Skin manifestations of biotin deficiency. Semin Dermatol. 1991;10(4):296-302.
16. Fritsche A, Mathis GA, Althaus FR. [Pharmacologic effects of biotin on epidermal cells]. Schweiz Arch Tierheilkd. 1991;133(6):277-83.
17. Shrivastava SB. Diffuse hair loss in an adult female: Approach to diagnosis and management. Indian J Dermatol Venereol Leprol. 2009;75(1):20-8
18. Kaimal S, Thappa DM. Diet in dermatology: revisited. Indian J Dermatol Venereol Leprol. 2010;76(2):103-15.
19. Rushton DH. Nutritional factors and hair loss. Clin Exp Dermatol. 2002;27(5):396-404.
20. Rasheed H, Mahgoub D, Hegazy R, El-Komy M, Abdel Hay R, Hamid MA, et al. Serum ferritin and vitamin d in female hair loss: do they play a role? Skin Pharmacol Physiol. 2013;26(2):101-7.
21. Riedel-Baima B, Riedel A. Use of the TrichoScan to assess female pattern hair loss. Dermatol Surg 2009;35(4):651-5.
22. Hoffman R. Trichoscan: Combining epiluminiscence microscopy with digital image analyses for measurement of hair growth in vivo. Eur J Dermatol. 2001;11(4):362-8.
23. Arck PC, Handjiski B, Peters EM, Hagen E, Klapp BF, Paus R. Topical minoxidil counteracts stress-induced hair growth inhibition in mice. Exp Dermatol. 2003; 12(5):580-90.
24. Budde J, Tronnier H, Rahlfs VW, Frei-Kleiner S. [Systemic therapy of diffuse effluvium and hair structure damage]. Hautarzt. 1993;44(6):380-4
25. Brzezińska-Wcisło L. [Evaluation of vitamin B6 and calcium pantothenateeffectiveness on hair growth from clinical and trichographic aspects for treatment of diffuse alopecia in women]. Wiad Lek. 2001;54(1-2):11-8.
The present study was carried out at Medcin Instituto da Pele - Osasco (SP), Brazil.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}