


Felipe Bochnia Cerci1; Tri H Nguyen2
Keywords: MOHS SURGERY; SURGICAL FLAPS; NOSE NEOPLASMS.
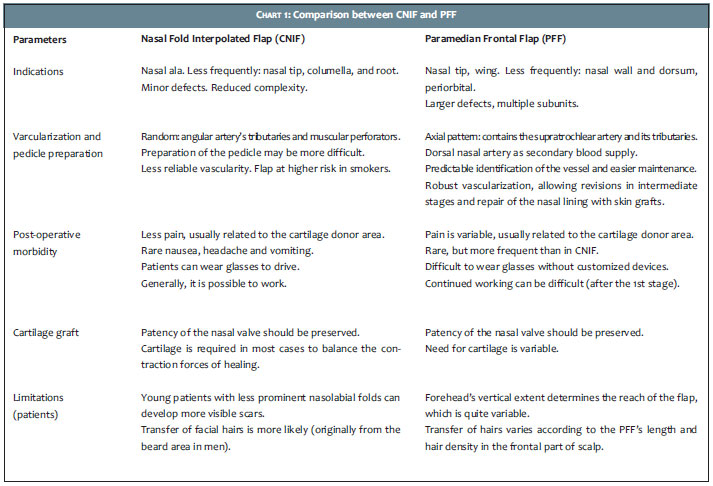
The nasolabial fold interpolated flap or cheek to nose interpolation flap (CNIF) is an instrumental flap in nasal reconstruction. The skin of the donor area (medial cheek) is very similar to that of the nasal ala.1 Its main indications are extensive and profound defects of the nasal ala and, less often, small defects of the lower portion of the nasal tip and columella.2 Proper training, good surgical technique, and careful planning are necessary to achieve optimal results.
The CNIF is classified as an interpolated flap done in stages due to the following characteristics: vascular pedicle based on a specific artery and/or on its tributaries, distant donor area and not contiguous to the defect, and more than one stage to complete implementation.3 Other interpolated flaps, such as the paramedian frontal flap (PFF), are capable of repairing distal nasal defects.4
Chart 1 compares CNIF's and PFF's characteristics in nasal reconstruction. One of the CNIF's advantages as compared to other flaps employed in alar reconstruction is the preservation of the alar groove, for which restoration is challenging when it is eliminated by single stage flaps (transposition of nasolabial fold), resulting in asymmetry of the alar grooves and an unfavorable outcome.5 The disadvantages are related to the fact that it needs two stages to be implemented, the post-operative care required for the exposed pedicle and, in men, the potential transfer of facial hairs to the nasal ala.2 The scar in the donor area is usually imperceptible. However, asymmetry of nasolabial folds may occur.6
The purpose of the present study is to evaluate CNIF's usefulness in alar reconstruction after Mohs micrographic surgery, especially in an outpatient setting under local anesthesia, as well as to discuss refinements in its design and implementation.
Patients
A retrospective study was carried out with 18 patients whose alar defects resulting from Mohs micrographic surgery were repaired with CNIF. The cases were selected from a private practice Mohs clinic in the period 2010-2013. Through the review and analysis of medical records and extensive photographic documentation, the following demographic and surgical data was evaluated: age, gender, tumor type, size of defect and involved subunits, number of Mohs stages, additional measures for the patient's comfort, cartilage grafts, pedicle design, post-operative complications, smoking habits, and follow-up and outcomes.
Prior to the surgery, all patients signed a Free and Informed Term of Consent allowing the publication of photographs in scientific journals. All procedures (Mohs surgery to remove the tumor and subsequent reconstruction) occurred in an outpatient setting. Nerve blocks (infraorbital) supplemented local anesthesia in some cases. Before the procedure, patients were given analgesics, benzodiazepines or oral antibiotics, as necessary. Most of the reconstructions occurred on the same day after Mohs surgery. Typically, the second stage was performed at three to four weeks after the first.
Design and implementation of the flap
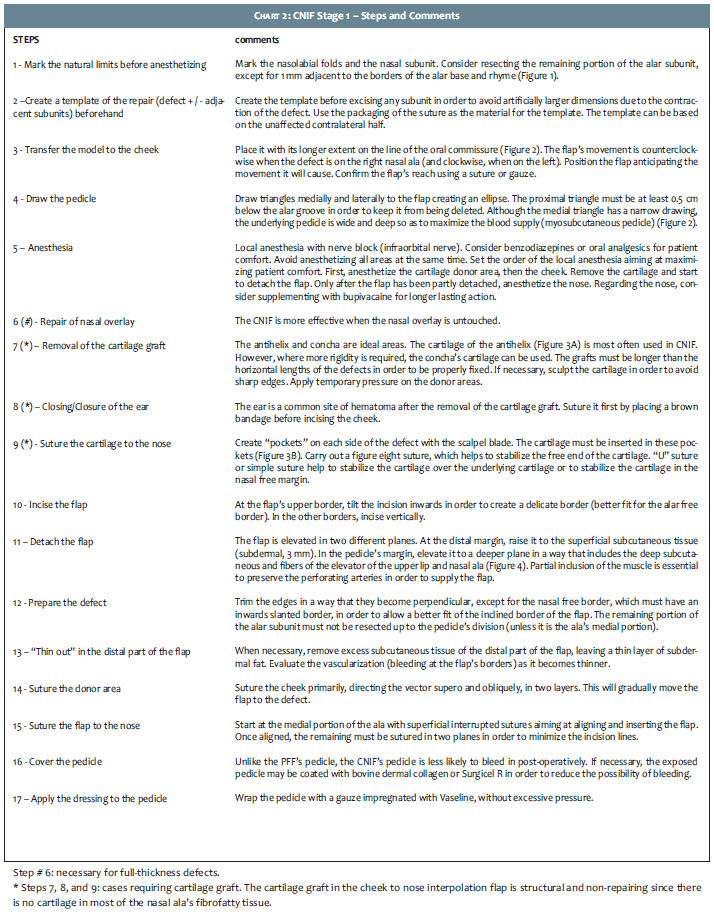
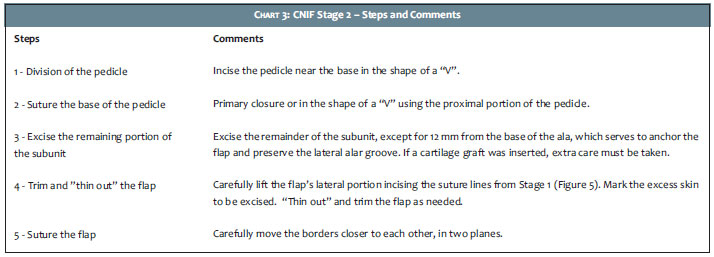
CNIF requires significant knowledge of anatomy, surgical planning, and surgical skills in order to achieve a correct design and successful implementation. The pedicle is marked close to the lateral portion of the alar groove. Unlike the pedicle of the PFF, which contains the supratrochlear artery, CNIF depends on the angular artery's myocutaneous perforators and tributaries for its viability, making it a random flap. As a result, its vascularization is lower than that of the PFF.2 Charts 2 and 3 describe the design and implementation of the flap step-by-step. (Figures 1-5) A variation of the traditional design is an option for patients whose terminal hairs might be transferred from the medial cheek. In this case, the pedicle is based inferiorly in order to recruit tissue from the upper and medial portions of the cheek, adjacent to the nasal wall.
Eighteen patients were included in the study. Demographic and surgical data is shown in Table 1. Patients ranged in age from 46 to 82 years (mean = 69 years), with no differences by gender (9 men X 9 women). Basal cell carcinoma was the most common cancer found (n = 16), followed by squamous cell carcinoma (n = 2). The number of Mohs stages required to obtain free margins ranged from 1 to 6 (average = 2.55). The size of the surgical defect ranged from 1.5 cm X 1.0 cm to 2.0 cm X 1.8 cm (average = 1.8 X 1.4 cm). Data concerning additional measures for greater patient comfort were available in 14 patients. Six (33%) patients received anxiolytics or oral analgesics as adjuvants to local anesthesia. Infraorbital block was performed in 8 (57%) patients. Only one participant was a smoker.
Seven patients (39%) had defects located only in the nasal wing, having been reconstructed with CNIF alone. However, 11 patients (61%), had defects involving the nasal wing and some adjacent anatomical subunit. Those patients underwent combined reconstruction, most commonly secondary intention (n = 7), due to the favorable location and small size of the nonalar defect. For the remaining patients, primary closure (n = 2), advancement of the cheek (n = 1), and bovine dermal collagen (n = 1) were combined with CNIF. The most frequently affected adjacent subunit was the nasal wall (n = 7), followed by the medial cheek (n = 3). Resection of the remaining portion of any subunit was performed in 14 (78%) of cases.
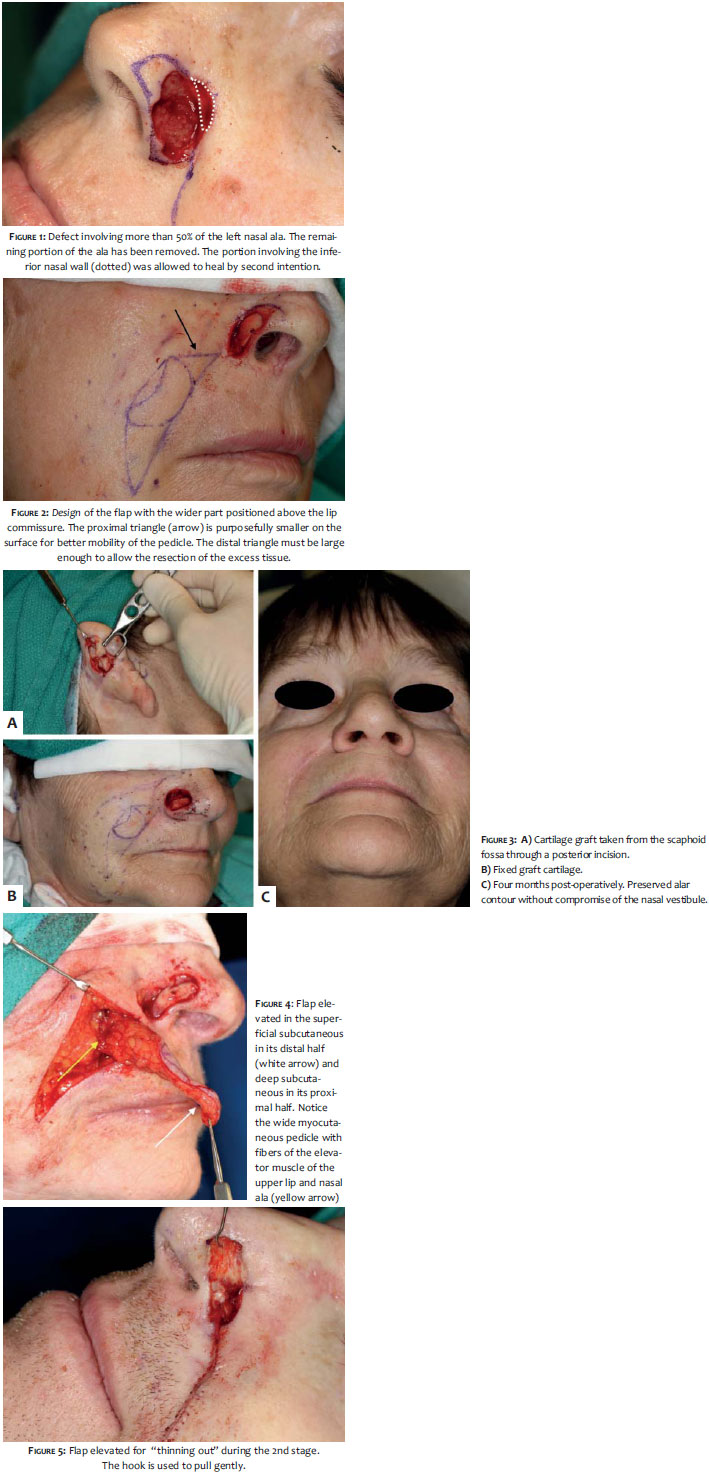
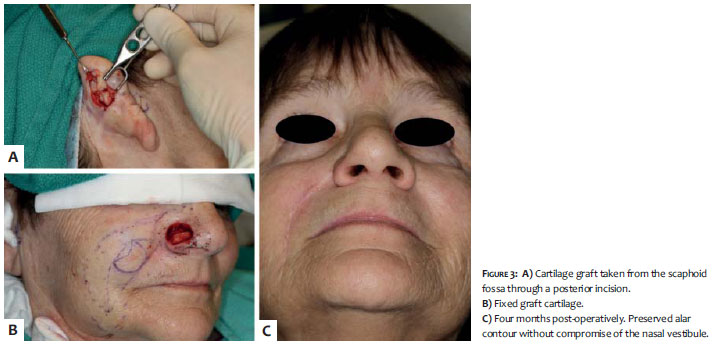
Structural support provided by auricular cartilage was necessary in 17 (94%) patients. The cartilage graft was removed from the scaphoid fossa/antihelix (n = 16) or concha (n = 1), through posterior incision in 15 (83%) patients. Bovine dermal collagen was used in three (17%) patients to cover the exposed surface of the pedicle.
There were no complications, such as post-operative bleeding, infection, or necrosis. No recurrence was observed after the follow-up, which ranged from 5 to 49 months (mean = 29 months). Optimal functional and aesthetic results were achieved in all patients.
The nasal ala is a common site for the occurrence of skin cancer and often presents challenging surgical defects following Mohs micrographic surgery.7 Repair options should be individualized according to each patient and surgical defect. For extensive and profound defects of the nasal wing, however, options that promote good functional and aesthetic results are limited. Although other options could be considered for such defects, CNIF has the advantage of preserving the alar groove and concealing the donor scar in the melolabial fold.5 The "soft" and fibrofatty nature of the donor area of the cheek is an additional advantage of the CNIF. The tissue of the cheek tends to contract and trapdoor. While this might be unfavorable in other places, it can effectively recreate the alar lobule's convexity. PFF is thicker and more rigid, and less capable of simulating the smooth and convex contour of the wing.8
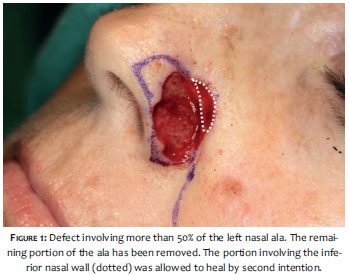
The principle of anatomical subunits is a key concept in reconstruction. If a defect involves more than half of the subunit, excising the remaining portion and repairing it as a whole can provide better results.9 (Figure 1) In the present study, 14 (78%) patients had their remaining alar subunit resected with excellent results. This principle, however, is not absolute.10 Through careful selection, some defects can be repaired without the complete resection of the subunit.
When different subunits are affected, independent closure options should be considered. This is especially true for subunits separated by concavities, such as the alar crease. The attempt to repair the nasal ala and medial cheek/nasal wall with CNIF can result in an enlarged nasal ala besides eliminating the alar groove. Small defects in these adjacent areas should be left to heal by secondary intention, which helps in recreating the alar groove's concavity. For medium to large defects, cheek advancement flaps are a sensible option. Following that principle, all patients with defects that extended into the medial cheek or nasal wall were reconstructed with combined options. (Figure 1)
The CNIF provides thickness of soft tissue, however it does not provide structural support. The nasal mucosa (nasal lining) and cartilage are the infrastructures that must be intact or be supplemented or repaired prior to the implementation of CNIF.11 Given that the CNIF is most often used for partial thickness alar defects, the repair of the nasal lining will not be discussed in the present article.
Cartilage grafts can be structural (native cartilage is present however there is need for additional cartilage for support) or restorative (replacement of removed cartilage). Cartilage grafts for CNIF are usually structural and not restorative, since there is no cartilage in most of the nasal ala, but only adipose and fibrous tissue. The structural functions of cartilage include: 1) preventing tissue contraction and distortion, 2) supporting "heavy" flaps, 3) maintaining nasal patency and widening the internal nasal valve, and 4) providing support for the contour.3 Donor areas of cartilage include the scaphoid fossa/anti-helix and auricular concha.12, 13
The incisions for the harvesting of cartilage can be either anterior or posterior. Anterior incisions are easier to access, however result in more visible scars. Cartilage of the anti-helix is ideal for long, flexible, and straight segments (Figure 3), while that of the concha is ideal for grafts that require more curvature, substance, and rigidity. Concha's grafts are more suitable for avoiding the collapse of the nasal valve and lobe. Anti-helix's grafts are more suitable for preventing the contraction of the free nasal border.12, 13 It is often necessary to sculpt the graft in order to obtain the desired thickness, shape, borders, and contour. This must be done carefully as the cartilage is a fragile structure and may fracture during the process.
Traditionally, a scalpel blade n. 15 is used to sculpt, however a shaving blade allows a more gentle sculpting of the graft's contours. Cartilage grafts can be removed safely under local anesthesia and with a low complication rate.14, 15 Post-operative pain is variable. Nonetheless, if cartilage grafts were performed, the auricular donor region is likely to be more painful than that of the cheek. For patient comfort, injection of a long duration anesthetic (bupivacaine) is recommended, after suturing the auricular donor area, in addition to administering post-operative analgesia (combined anti-inflammatory/narcotic combination).
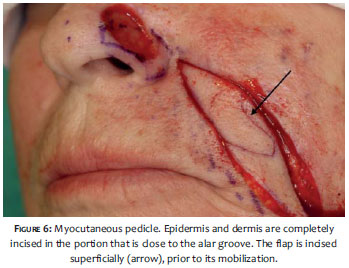
The pedicle of the CNIF can be myocutaneous (skin portion of the pedicle connected) or myosubcutaneous (epidermis and dermis are completely incised proximally and released).3 (Figure 6) myosubcutaneous design is preferable since it makes the flap island flap release the restriction of the epidermis and dermis, and reduces tension and twists the pedicle. Furthermore, the design in the shape of an "island", allows dissection of a wider pedicle, with a smaller proximal triangle, increasing mobility.
Regardless of design, both pedicles should contain muscle fibers of the elevator of the upper lip and nasal ala. In this study, all pedicles were myosubcutaneous. Potential complications include CNIF post-operative bleeding, improper healing, infection, dehiscence, distortion-free margins, and necrosis.16 In a recent study by Newlove and Cook,17 the CNIF complication rate when performed by dermatologic surgeons in an outpatient setting under local anesthesia, was equal to or lower than in studies of other surgical specialties. In this study there were no complications, possibly due to the smaller number of patients.
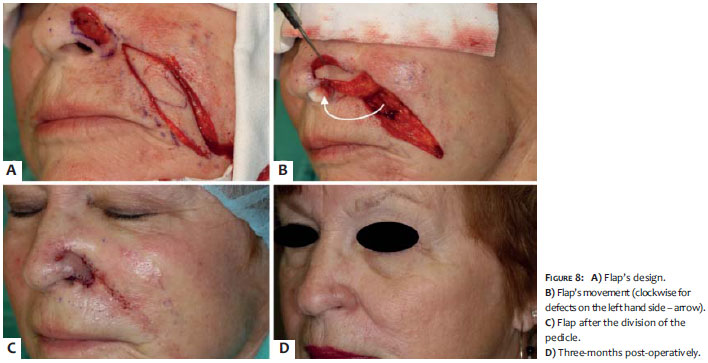
The CNIF is crucial in reconstructing alar defects after Mohs micrographic surgery. If adjacent subunits such as the medial cheek or nasal wall are involved, the CNIF must be combined with another repair method for best results. With proper planning and meticulous surgical technique, the CNIF can be safely performed in an outpatient setting. (Figures 7 and 8)
1. Arden RL, Nawroz-Danish M, Yoo GH, Meleca RJ, Burgio DL. Nasal alar reconstruction: a critical analysis using melolabial island and paramedian forehead flaps. Laryngoscope. 1999;109(3):376-82.
2. Nguyen TH. Staged cheek-to-nose and auricular interpolation flaps. Dermatol Surg. 2005;31(8 Pt 2):1034-45.
3. Nguyen TH. Staged interpolation flaps. In: Roher TE, Cook JL, Nguyen TH, Mellete Jr, JR, editors. Flaps and grafts in dermatologic surgery. New York: Elsevier; 2007. p. 91-105.
4. Cerci FB, Nguyen TH. Paramedian forehead flap for complex nasal defects after Mohs micrographic surgery. Surg Cosmetic Dermatol 2014;6(1):17-24.
5. Fader DJ, Baker SR, Johnson TM. The staged cheek-to-nose interpolation flap for reconstruction of the nasal alar rim/lobule. J Am Acad Dermatol. 1997;37(4):614-9.
6. Cook JL. The undesirable influence of reconstructive procedures on the symmetry of the nasolabial folds. Dermatol Surg. 2005;31(11 Pt 1):1409-16.
7. Cook JL. The lateral ala's volume and position are critical determinants of aesthetically successful nasal reconstruction: a photographic case series. Dermatol Surg. 2009;35(4):667-73.
8. Burget GC, Menick, FJ. Aesthetic Reconstruction of the Nose. St Louis: Mosby-Year Book; 1994. p. 57-91.
9. Burget GC, Menick FJ. The subunit principle in nasal reconstruction. Plast Reconstr Surg. 1985;76(2):239-47.
10. Rohrich RJ, Griffin JR, Ansari M, Beran SJ, Potter JK. Nasal reconstruction beyond aesthetic subunits: a 15-year review of 1334 cases. Plast Reconstr Surg. 2004;114(6):1405-16; discussion 1417-9.
11. Burget GC. Aesthetic restoration of the nose. Clin Plast Surg. 1985;12(3):463-80.
12. Ratner D, Skouge JW. Surgical pearl: the use of free cartilage grafts in nasal alar reconstruction. J Am Acad Dermatol. 1997;36(4):622-4.
13. Byrd DR, Otley CC, Nguyen TH. Alar batten cartilage grafting in nasal reconstruction: functional and cosmetic results. J Am Acad Dermatol. 2000;43(5 Pt 1):833-6.
14. Sage RJ, Leach BC, Cook J. Antihelical cartilage grafts for reconstruction of mohs micrographic surgery defects. Dermatol Surg. 2012;38(12):1930-7.
15. Kaplan AL, Cook JL. The incidences of chondritis and perichondritis associated with the surgical manipulation of auricular cartilage. Dermatol Surg. 2004;30(1):58-62; discussion 62.
16. Arden RL, Miguel GS. The subcutaneous melolabial island flap for nasal alar reconstruction: a clinical review with nuances in technique. Laryngoscope. 2012;122(8):1685-9.
17. Newlove T, Cook J. Safety of Staged Interpolation Flaps After Mohs Micrographic Surgery in an Outpatient Setting: A Single-Center Experience. Dermatol Surg. 2013;39(11):1671-82.
The present study was carried out at Mohs & Dermatology Associates - Northwest Diagnostic Clinic - Houston (TX), USA
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}