


Daniel Dal'Asta Coimbra1; Natalia Caballero Uribe2; Betina Stefanello de Oliveira2
Keywords: REJUVENATION; SKIN; FACIAL MUSCLES.
The perception of beauty is an experience or process based in the way that certain physical elements appeal uniquely to the individual beholder. Some believe that there is a strong connection between beauty and mathematics, as evenly proportioned, symmetrical faces with rounded contours, high cheekbones, and clearly-defined eyebrows appear to be more attractive. Alterations in the proportions of facial structures take place with the aging process, leading many individuals to seek aesthetic treatments aimed at reversing or maintaining their appearance from youth.
This beauty standard was set in ancient times in Egypt, and was based on records of Queen Nefertiti's facial appearance, which is perhaps the most beautiful facial image that the world has ever known. Her name was probably pronounced as "Naftaiyta" meaning "beauty has arrived." Her fame has overcome the barriers of time. Her perfectly symmetrical face, gently curved eyebrows, almond-colored and carefully defined eyes, prominent zygomatic bones, thin and proportional nose, full lips, absence of wrinkles or expression marks, and thin, elongated neck established an ideal of beauty that is pursued to the present day.1
The literature describes how, during youth, the human face is shaped like an inverted triangle, with the apex pointing downwards, translating into a well-defined facial middle third. Through the aging process, changes infacial structure leadto a loss of contours and volume, with the inversion of the triangle seen in youth. Other facial shapes can be described as oval, round, heart-shaped, and square, among others.
Not long ago, with the discovery of the facial fat compartments 2,3 and the introduction of higher viscosity hyaluronic acid in the treatment of volume replacement and improvement of facial contours, the approach to the treatment of facial aging with the use of cutaneous fillers saw the onset of a new age. This new approach focuses on the face as a whole, attributing importance to the maintenance of its three-dimensionality and not onlyto the treatment of wrinkles and furrows, which are often the result of a decrease in the volume of facial fat and bone resorption resulting from aging.
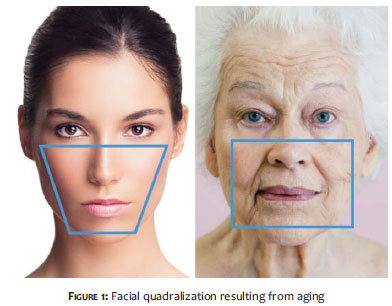
The authors call the changes in facial contours resulting from aging "quadralization" of the face: while in youth the face is shaped like an inverted trapezoid, it tends to become a square over time. (Figure 1)
Seeking a better understanding of the reasons related to facial "quadralization", the aging process will be approached in the present article based on four main pillars: sagging skin, muscle depressant action, volumetric decrease in fat compartments, and loss of the deep support due to bone remodeling.
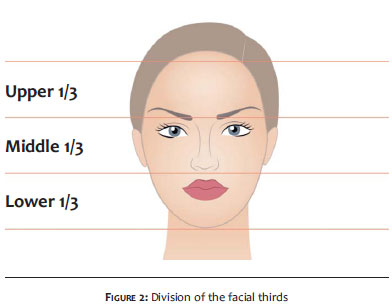
A very common practice consists of dividing the face horizontally into thirds, in order to assess its symmetry and balance. The upper third runs from the hairline to the glabella, the middle third runs from the glabella to the subnasal region, and the lower third runs from the subnasal region to the mentum.4 (Figure 2)
Different types of alterations occur in the face during the aging process. In the upper third, these alterations are related to chronic damage caused by ultraviolet light, to the intrinsic muscles of facial expression and its influences on the skin, and to gravitational changes linked to loss of tissue elasticity.5-7 In the middle third, they result from a combination of photoaging, loss of subcutaneous tissue, loss of skin elasticity and remodeling of bone and cartilaginous structures. The orbital septum can weaken over time, allowing protrusions of fat in the upper or lower eyelid. However, some people may experience loss of subcutaneous tissue in the eyelid, which causes a sunken appearance. The malar region can be affected by the loss of buccal fat volume, which is located between the masseter muscle (anteriorly) and the buccinator muscle (posteriorly). The support mechanisms of the nasal tip can become inelastic and stretch with age, resulting in the ptosis of the nasal tip and an apparent lengthening of the middle third of the face.5-9 In the lower third, the alterations result from the combination of chronic damage by ultraviolet light, loss of subcutaneous fat, changes linked to the muscles of facial expression and neck, gravitational changes due to loss of tissue elasticity and remodeling of the bone and cartilaginous structures. The structure of dentition and the resorption of the maxillary and mandibular bones can result in a widespread loss of size and volume. The chin rotates anteriorly and becomes thinner and more protruded. In addition to an intrinsic decrease in the volume of the lips, the tip of the nose's ptosis can also contribute to the appearance of a reduced upper lip.5-8
In this manner, the present study will cover the four main aesthetic pillars related to these alterations in order to achieve a better understanding of the aging process and of the of indication of treatment techniques for the recovery or maintenance of facial contours.
1. Sagging Skin
The skin's tension lines are the result of multiple interactions of extrinsic and intrinsic factors. Intrinsic factors are independent of one's will, reflecting genetic inheritance. They consist of inherent properties of extensibility, elasticity, and tension that are associated with the skin's biostructural components. These structural elements consist of dermal collagen and elastic tissues. With age, collagen begins to increase cross-linking, having reduced its volume and elasticity. The elastic fibers are more abundant in the facial dermis than in the scalp, and therefore are responsible for maintaining the skin's static tensionby restoring deformed collagen to its original state. With age, and especially with prolonged exposure to the sun, the elastic fibers are subject to structural and functional deterioration, gradually losing the ability to return to its original length, which results in the loss of skin firmness.9
Extrinsic aging is primarily caused by the exposure to the sun, but also by smoking, excessive alcohol consumption, and poor diet, among other factors.3 In addition to extrinsic factors, the muscles of facial expression insert directly into the skin, exerting continuous tension even at rest. Over time they causethe stretching of the collagen in the direction that the muscles move.
In childhood, the elastic tissue remains in its configuration, and those changes are not very apparent. With age, the skin loses elasticity, and elongation begins to be noticed, with redundant skin being directed to wrinkles and rhytids. Linear wrinkles result from the union of multiple fibers of the superficial musculoaponeurotic system (SMAS) with the dermis, stretching the skin and reducing its tension in the direction of the facial muscles' movement. The tension lines of the skin are perpendicular to the sum of the force vectors of the muscles' movement. The decrease in tension, the increase in the elongation of collagen fibers and the progressive reduction of the elastic tissue produce such lines, which exacerbate gradually with aging and/or solar damage.9
Thus, these factors together lead to anincrease in skin sagging and a"surplus" ofskin on the face and neck.
2. Muscular action
In youth, the muscles of facial mimicry have a curvilinear contour with anterior convexity on the surface, which makes them project outward. This manifests as a bend in the fat compartment underneath the deep face of these muscles, acting as a mechanical slide plane. The motion amplitude of the muscle is equally greater. Over time, the convex contour becomes flat and the underlying fat is expelled from behind the muscles, causing an increase in the superficial fat.3
The frontal muscle has little underlying fat. During contractions, maximum pressure is exerted on its central functional area, where the elevating and depressor forces converge, over time producing upper (frontal collisions) and lower (supercilliary arch) convexity due to resorption of the central horizontal bone.
The muscles of the glabellar region are responsible for the main evident alterations of aging in the upper third of the face, for they have a strong depressant action. The corrugator, procerus, depressor supercilii, and the upper portion of the orbicularis oculi muscles belong in this region. Their joint action contributes to the facial appearance of tiredness and boredom, as well as to the increase of skin in the upper palpebral region and to the displacement of fat pads in this region.
The contraction of the orbicularis oculi muscles are also responsible for facial aging, leading to the protrusion of the orbicular fat, resulting in palpebral bags, in addition to contributing to the fall of the eyebrow tail, to the onset of periocular rhytids (crow's feet), and to the increase in cutaneous ptosis in the palpebral region. Repeated contractions of the corrugator supercilii muscle expel the deep fat compartment, contributing to the erosion of the bone of the orbit.
The upper lip and nasal ala levator muscle is a combination of two other muscles: one superficial (levator of the nasal ala) and one deep (levator of the upper lip). Its repeated contractions expel the fat (inferior and deeply) from the canine fossa and (superficially) from the nasolabial fold, flattening the convexity of the anterior malar region. Over time, a depression that increases noticeably with the smile movement appears above the nasolabial fold, in the paranasal area. The deep fat, which in youth is located between the cutaneous insertion of the levator muscle of the nasal ala and the pyriform orifice, is also expelled to the nasolabial fold.
With aging, the zygomaticus major and minor muscles expel the deep underlying fat located in the lower region, leading to the emptying of the jugal area. The muscles of facial mimicry are particularly strong in the periorbital and perioral areas. Their repetitive contractions combined with the increase of tonus at rest not only expel the underlying fat, but also exert constant pressure on the bone, favoring its erosion. Repeated contractions of the orbicularis oris muscle lead to the appearance of perioral rhytids, in addition to aiding in the reduction of volume and the loss of lip contour.
Repeated contractions of the depressor anguli oris muscle, combined with the elevation produced by the mentalis muscles, expel the underlying fat towards the upper middle cervical region by increasing an excess of skin. Furthermore, the resting tonus of the depressor muscles of the mouth and of the angle of the mouth increases over time, depressing the commissure and deepening the labiomental fold.4 Below the mandible, contractions of the depressor anguli oris muscle stimulate the platysma muscle, expelling the deep fat anteriorly.
In youth, the platysma has a configuration in the shape of an hourglass, simulating a narrower "waist" between its inferior transversal origin and the upper transverse insertion that helps to define the cervicomandibular angle. With aging, its tonus at rest increases and its vertical length shortens, leading to the formation of anterior bands that delete the cervicomandibular angle. Over time, the platysma muscle's contractions expel the fat deep and anteriorly in the submental region.
3. Facial fat compartments
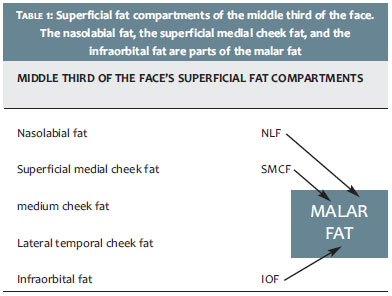
Facial fat is divided into separate compartments that are limited by distinct anatomical units and their own vasculature (Tables 1 and 2). Coleman et al. described different fat compartments, subdivided into regions: periorbicular, temporal, perioral, middle third of the face, cheeks, and mandibular.10
The fat compartment of the periorbicular region is distributed between the upper and lower eyelids. The orbit presents an almost uniform loss of volume, and is more important in the upper medial and upper lateral compartments. The loss of volume in the upper region of the orbit causes a deflation of tissues towards the cilliary margin, causing excess skin and a sunken appearance. 3,7,10
The volume in the temporal region is also influenced by the temporal muscle and the deep and superficial fat compartments. In aging, there is an atrophy of fat over the frontal process of the zygomatic bone and superior zygomatic arch, which can thus become visible. 3,7,10
In the perioral region-which is predominantly composed of the orbicularis oris muscle-a relative absence of fat occurs. During aging, the upper lip usually becomes thinner, and there is less protrusion of the maxillary bones and an inversion of the lip. The lower lip loses the fullness of its submucosa, and reverses. 3,7,10 The most significant loss of fat takes place in the middle third of the face, especially in the pre-auricular, buccal, and malar areas, leading to convexities. In more severe cases this can cause a skeletal appearance. 3,7,10
In the maxillary region, the angle and the mandibular body-with their overlying masseter and platysma muscles-define the inferior border of the lower portion of the face, delineating the mandible's contour. With aging, remaining fat deposits that descend and deform the mandible's border can occur, reducing facial fullness. 3,7,10
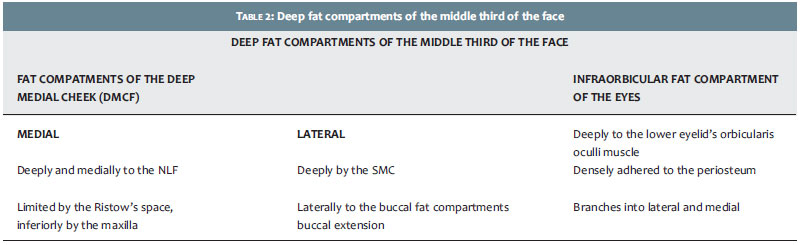
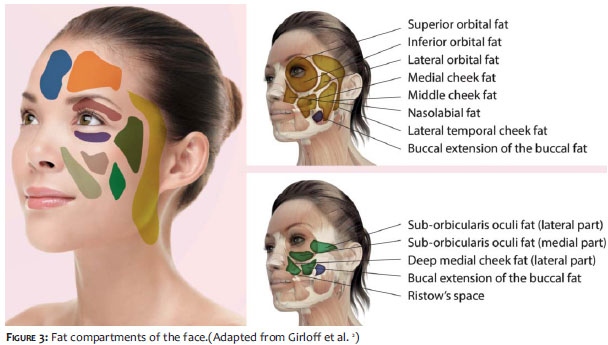
In a study employing contrast tomography on the faces of cadavers, Gierloff et al. proposed a different classification for the fat compartments described above. The compartments were divided into the fat of the facial middle third-consisting of two layers (superficial and deep)-and the fat of the paranasal region-anatomically divided into three different layers.2 (Figure 3)
The facial middle third's fat superficial layer is composed of: nasolabial fat, medial and middlecheek fat, the temporofrontal compartment, and three orbital compartments. The deep layer fat is constituted by the infraorbicular fat and the medial and deep cheek fat. Three distinct layers of fat compartments are found in the pyriform aperture, where the compartment is located posteriorly to the medial portion of the deep medial cheek fat.2
The nasolabial compartment is subcutaneous and oval in shape. Its upper border is located in the lower contour of the orbit, and its inferior extension is adjacent to the fat of the superior mentum. It is limited laterally by the medium malar fat and infraorbicular fat. The medial border is composed by the maxilla and the lateral compartment of the upper lip. The fat compartment of the medial cheek is located laterally to the nasolabial compartment. The lower limit is set bythe mentum's fat and the buccal extension of the buccal fat. It is limited laterally by the fat of the medium cheek region and the lateral orbital compartment. Its posterior border is formed by: orbicularis oculi muscle, the deep medial cheek fat pad and the buccal fat pad.
The medium cheek's compartment is located anteriorly to the frontotemporal compartment and laterally to a line perpendicular to the lateral orbital rim. Its anterior limit is the fat of the malar regionand a small portion of the buccal fat pads. Its superior limit is the lateral orbital compartment. The deep medial cheek's fat compartment is subdivided into a medial and a lateral portion. The medial portion is located underneath the nasolabial compartment, but extends farther medially. It does not immediately rest on the maxilla's periosteum, being posteriorly limited by a small triangular compartment. Its lateral portion limits the superficial medial cheek's fat. It is superiorly limited by the infraorbital fat, and laterally by the buccal fat pad. The compartment rests medially on the deep medial cheek fat and laterally on the maxilla. The infraorbicular fat is divided into two: the medial portion is located above the maxilla's periosteum, and its lower portion, above the lateral portion of the deep medial cheek's fat; the medial portion of the infraorbicular fat is covered by the nasolabial fat and medial cheek. The lateral portion of the infraorbicular fat is located beneath the lateral orbital fat compartment and the medial cheek.2
The buccal fat compartment plays an important role for it runs from the deep paramaxillary space up to the lower superficial subcutaneous plane of the zygomatic bone. The buccal extension of the buccal fat compartment is deemed as a portion of the posterior lobe. However, Gierloff et al. observed in 29% of the cadavers studied that the buccal extension of the buccal fat pad can be considered a separate compartment for displaying a limited anatomical site-in this specific case, a third layer.2 This compartment is located inferiorly to the zygomatic bone and anteriorly to the mandible's branch, around the masseter muscle. Only a small portion of the compartment is located in the para-maxillary space. The subcutaneous portion of this fat compartment is composed of the medial cheek fat, deep medial and central fat, infraorbicular fat, mentonian fat, and premasseter space fat, possibly being related to the support of all these fat compartments.3 The orbital region is divided into superior, inferior and lateral compartments. The inferior orbital fat compartment is located in the subcutaneous plane, beneath the middle portion of the orbit's bone, with its inferior border running along this same inferior course. The compartment's inferior limit is the cheek's medial, central, infraorbicular, and nasolabial fat. The superior orbital fat compartment is located immediately beneath the skin of the upper eyelid. Its upper border follows the course of the orbital bone, and its lateral portionis located on the lateral of the orbital bone. The inferior border of the lateral orbital fat is the medial cheek's fat. The lateral orbital compartment, the superior border follows a virtual line that runs between the superior orbital contour and the temporomandibular joint. The compartment's lower portion overlaps the lateral portion of suborbicular fat. The lateral orbital fat is limited laterally by the temporal cheek's fat.2
Alterations related to the decrease in volume, atrophy, and migration to lower regions of the face of these fat compartments are probably the main factors of structural changes linked to the aging of the face.
More recently, Wan et al.11 studied 63 hemifacial cadaver dissections and observed three main alterations: 1) adipocytes of superficial fat compartments were larger when compared to adipocytes from deep fat compartments; 2) the adipocyte's size in nasolabial (NLF) and in deep medial cheek (GBMP) fat compartments in men is significantly smaller when compared to women's; 3) the adipocyte's size in the nasolabial compartment (NLF) in patients with normal body mass index (BMI) is significantly higher in women than in men. This corroborates to the clinical and anatomical observations that suggest that there are morphological differences between the superficial and deep compartments of fat, specifically selective atrophy in the deep fat compartments in the elderly. This finding can be clinically relevant for the purposes of volumetric facial rejuvenation.
4. Facial bone remodeling
The areas with a predisposition to bone remodeling correspond to the moving parts of the face, especially to the superomedial and inferolateral areas of the orbit, pyriform region of the nose, mentum, and particularly the maxilla, in which this process is more prominent.
The alterations occur with age, and therefore produce a protrusion of the glabella, expansion of the supraorbital wrinkles, lateral translation of the orbit, increasing depth, lateral expansion of the cheeks, and increasing size of the nose and mentum.
The orbit's medial fat pad also becomes more prominent with age, possibly resulting from the resorption of the upper border of the orbit.
The middle malar region manifests more complex alterations in soft tissue as a result of aging. The development of deformity in the nasojugal fold, malar fat, and prominent nasolabial fold can, to a significant degree, be attributed to some fat loss or ptosis, linked to aging.
The loss of the projection of the maxilla contributes to the increase in the pyriform aperture, due to the fact that there is a decrease in the support both of the nose and of the upper lip, resulting in the ptosis of the centrofacial region and entailed elongation of the nose up until the upper lip.
The maxilla is the bone that undergoes greater remodeling with aging, the consequences of which are noticed on the cheek. The maxillary bone gives rise to other bones-and respective function-that form the orbit. In youth it expands to accommodate the growth of secondary dentition, which develops within the bone, resulting in a great reduction in volume, especially in its inferior portion.12
With aging, the lower third of the face undergoes vertical maxillary shortening, affecting dental and skeletal structure. This negative combination also influences the patient's smiling function, thereby reducing the exposure of the upper and anterior teeth. Sometimes, the structural factors of aging are not easily detected due to the compensation offered by the soft tissues, which in a young individual plays an important camouflage role.13
Based on the observation of facial shapes, on the experience acquired with the use of cutaneous fillers for volume replacement, on studies of facial aging processes2,3,7 and on contour alterations resulting from aging, a new nomenclature and approach to the alterations in the facial contour resulting from aging is proposed: the "quadralization" of the face. Some authors believe that in adolescence the face has the shape of a heart or inverted triangle and that, with aging, the triangle's position reverses, changing its base to the line of the mandible. The authors however, believe that all faces have a unique shape, similar to that of an inverted trapezoid, with the superior limit being constituted by a line running along the most projected portions of the zygomatic bone and with the lower limit being defined by a line drawn laterally to the mentalis muscles, approximately in the junction of the depressor muscles of the lower lips with the mandible. What varies from one individual to another, both in men and in women are this trapezoid's internal angles, which can be more or less acute depending on the facial shape.
In this manner, rather than approaching the facial alterations occurring from aging as the reversion of the triangle from youth, the authors observed an increase in the upper angles of the trapezoid, accompanied by a minor shortening of the superior line (zygomatic bone resorption) and a decreasein the inferior angles accompanied by an evident increase in the trapezoid's inferior line (displacement of facial structures towards the lower third of the face), so that this inverted trapezoid will tend to become a square over the years, regardless of gender, race, and facial shape. The changes in facial contours that characterize this process are related to the four aesthetic pillars associated with aging. Therefore, healthy lifestyle habits associated with aesthetic treatments targeted at each of these pillars can possibly preserve the beauty of the face for longer, mainly due to the maintenance or improvement of its tridimensionality.
Based on the literature descriptions of structural changes of the face and clinical experience, a new nomenclature, defined as facial "quadralization" is proposed for the alterations of facial contours resulting from aging. This approach can possibly assist in directing and developing new forms of aesthetic treatments aimed at maintaining and/or restoring the three-dimensional shape of the face, altered by the passage of years.
1. Seganfredo C, Franchini AS. Akhenaton e Nefertiti- uma história amarniana. Porto Alegre: L± 2011.
2. Gierloff M, Stöhring C, Buder T, Gassling V, Açil Y, Wiltfang J. Aging changes of the midfacial fat compartments: a computed tomographic study. Plast Reconstr Surg. 2012 129(1):263-273.
3. Pessa JE, Rohrich RJ. Discussion: Aging changes of the midfacial fat compartments: a computed tomographic study. Plast Reconstr Surg. 2011;129(1):274-5.
4. Louran CL, Buthiau D, Buis J. Structural aging: the facial recurve concept. Aesth Plast Surg. 2007;31(3):213-218.
5. Carruthers J, Carruthers A. Técnicas de preenchimento. Rio de Janeiro: Elservier;2005.
6. Bartlett SP, Grossman R, Whitaker LA. Age-related changes of the craniofacial skeleton: an anthropometric and histologic analysis. Plast Reconstr Surg. 1992;90(4):592-600.
7. Coleman SR, Grover R. The anatomy of the aging face: volume loss and changes in 3-dimensional topography. Aesthet Surg J. 2006;26(1S):S4-9.
8. Mendelson B, Wong CH. Changes in the Facial Skeleton With Aging: Implications and Clinical Applications in Facial Rejuvenation Age-related changes of the orbit and midcheek and the implications for facial rejuvenation. Aesthet Plast Surg.2012;36(4):753-60.
9. Salasche S, Bernstein G, Senkarik M, surgical anatomy of the skin. Michigan: Appleton & Lange; 1988.
10. Coleman SR, Saboeiro A, Sengelmann R. Comparison of lipoatrophy and aging: volume deficits in the face. Aesthet Plast Surg. 2009;33(1):14-21.
11. Wan D1, Amirlak B, Giessler P, Rasko Y, Rohrich R, Yuan C, et al. The differing adipocye morphologies of deep versus superficial midfacial fat compartiments: A cadavery study. Plast Reconstr Surg. 2014 Jan 17. [Epub ahead of print].
12. Mendelson B, Wong CH. Changes in the facial skeleton with aging: Implications and clinical applications in facial rejuvenation. Aesthetic Plast Surg. 2012;36(4):753-60.
13. Meneghini F, Biondi P. Clinical facial analysis: elements, principles, and techiniques. Berlin: Springer; 2012. p.157-174.
This study was performed at the Instituto de Dermatologia Rubem David Azulay da Santa Casa de Misericórdia do Rio de Janeiro - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}