


Ana Flávia Nogueira Saliba1; Nilton Di Chiacchio2; Gabriel Ângelo de Araújo Sampaio3; Natássia Pinheiro de Lavor Queiroz4
Keywords: NAILS; ONYCHOMYCOSIS; ONYCHOMYCOSIS/DIAGNOSIS; DIAGNOSIS.
Onychomycosis is a fungal infection that affects the nails, accounting for about 50% of all onychopathies. 1-4 It is estimated that the prevalence ranges from 2-13% in the general population, reaching 48% among those over 70 years old.5 Approximately 20% of the U.S. population, aged between 40 and 60 years, has onychomycosis.1
A recent Brazilian study showed a higher prevalence of onychomycosis in females in the age group above 46 years and in people who practice sports. The nails of the halluces were the most affected, and Trichophyton rubrum was the most frequently isolated fungus.6
In most cases there is involvement of the nails of the feet, probably due to the fact that the growth rate of these nails is 50-60% slower than those of the hands, facilitating infection. Studies show that the proportion of involvement of the fingernails and toenails was 1:4 in Spain and 1:19 in Canada.2
Onychomycosis can be caused by three different fungi types: dermatophytes, yeasts and non-dermatophytes. Dermatophytes are keratinophilic fungi and are considered the most common agents, being responsible for about 90% of cases. In this group, the Trichophyton rubrum, followed by the Trichophyton mentagrophytes stand out as the most frequent species. 2,7-9
Onychomycosis caused by yeast is rare and, in most cases, is present in the nail only as a colonizing fungus. It usually affects patients with several comorbidities or with some degree of immunosuppression and most often affects the fingernails.2,6 According to the literature data, yeasts are involved in 5-17% of cases of onychomycosis, the most common being Candida albicans.2,7,9 Studies show a high prevalence of the Candida species in northeastern Brazil.10-12
The non-dermatophyte fungi are agents that are rarely involved. Some articles have questioned the real pathogenicity of these fungi in the nail 4, 12,13 and support the idea that, in most cases where these fungi are isolated, they are not the real causal agent, but rather the contaminant agents. Thus, the diagnosis of onychomycosis caused by non-dermatophytes is difficult, since they are common contaminants of nails and in mycology laboratories. The most frequently isolated species is the Scopulariopsis brevicaulis. 2,4
Lately, an increase in reports of cases of onychomycosis caused by non-dermatophyte fungi has been observed, mainly in Europe, with prevalence rates ranging from 1.6-6%.5 Onychomycosis can be classified into four types, depending on their clinical presentation, i.e. the type of involvement of the nail plate. 1,6,7,14
The distal and lateral subungual onychomycosis (DLSO) is the most common form. The fungus invades the nail through the hyponychium and grows slowly and proximally. Hyperkeratosis of the nail plate and onycholysis can be observed, making it opaque. The white superficial onychomycosis (WSO) mainly affects the toenails and the main agent is the Trichophyton mentagrophytes. Hyphae parasitize the most superficial portion of the nail plate, causing a white, opaque, brittle fingernail appearance. In proximal subungual onychomycosis (PSO), the fungus invades the proximal portion of the nail through the proximal nail fold, forming a whitish area in the lunula region and progresses distally.
The total dystrophic onychomycosis (TO) is the clinical form that corresponds to the advanced stage of the disease. There is destruction of the plate, leaving only keratin debris and a thickening of the nail bed.
In a recent study, Hay and Baran proposed a new classification for onychomycosis, including the clinical forms already mentioned, the "endonyx" onychomycosis, the mixed pattern onychomycosis and the secondary onychomycosis.15 The "endonyx" onychomycosis is characterized by the invasion of the nail plate without involvement of the nail bed. It presents lamellar separation of the nail plate with discoloration, and absence of inflammation of the nail bed or subungual hyperkeratosis. The mixed pattern comprises cases that show the combination of different patterns of infection in the same nail, while the secondary onychomycosis corresponds to fungal infection of the nail and surrounding tissues secondary to other conditions such as psoriasis and trauma.
The difficulty in establishing a clinical diagnosis of onychomycosis, coupled with the fact that the treatment of this condition often requires the use of systemic antifungal agents for long periods, causing potential side effects, justifies the need to establish the correct diagnosis, with the isolation of the causative agent. 3,4
There are several methods used in the diagnosis of onychomycosis: direct microscopy, fungal culture, histological examination of the nail plate stained by PAS, immunohistochemistry, plate dermoscopy, confocal microscopy, flow cytometry, scanning electron microscopy and polymerase chain reaction (PCR). 3,4,12,16,17
Currently, the most widely used diagnostic tests are direct microscopy with potassium hydroxide and cultures 3,16 These methods, however, require time and may present technical difficulties, even when performed by experienced professionals.16
The sample collection is the most critical phase in the diagnosis of onychomycosis. In general, samples should be collected in the most proximal part of the affected nail,12 but usually due to ignorance or technical difficulties, the collection of the most distal part of the nail is carried out, where the fungal viability is low.13 In direct mycological examination, the scales are bleached with 20-30% potassium hydroxide (KOH), which also acts by dissociating hyphae from the keratinocytes. The sensitivity of this test can be improved when using 40% DMSO (dimethyl sulfoxide). Stains such as Parker blue-black, and chlorazol Black E and calcofluor can also improve the visualization, staining the hyphae with various colors.1,4,12
In a direct mycological examination it is possible to visualize fungal elements, such as septate and hyaline hyphae or pseudohyphae, however it is not possible to establish the species and fungal viability. 4,12
A culture is needed to identify the etiologic agent. The collected material must be seeded in at least two culture media, the most common is Sabouraud agar. 1,7 The culture media may also contain antibiotics (chloramphenicol) and cycloheximide in order to inhibit the growth of contaminating bacteria and fungi, respectively. 12,18 The accuracy of both the mycological exam and the culture ranges from 50-70%, depending on the technique of collection and sample preparation.12 Due to the variable sensitivity of these methods, other diagnostic tests are being used.
Histological examination of the nail can be considered a supplementary test in cases where the direct mycological exam and the culture were not able to confirm the diagnosis, but a clinical suspicion remains. In this examination, the fragment of the nail is stained with PAS (Periodic Acid-Schiff), allowing visualization of fungal structures, as well as the extent of the infection.3,12
In recent studies, Borkowski et al. as well as Lawry et al. compared the efficacy of various methods for the diagnosis of onychomycosis.4 Both studies concluded that the histopathologic examination with PAS was more effective than the direct mycological examination and the culture. However, the histopathological examination has the disadvantage of being unable to establish the identity of the causative agent and does not provide information on the pathogen's viability.
More advanced diagnostic techniques such as immunohistochemistry, flow cytometry, confocal microscopy and PCR have been used successfully in the diagnosis of onychomycosis. However, large-scale implementation of these methods is very unlikely due to the need of cutting edge technology and high cost.
Thus, in daily clinical practice, especially regarding the sampling process, resources capable of increasing the accuracy of the mycological examination and culture are used. Onychoabrasion consists of sanding the nail plate using an electrical device and sandpaper of varying roughness.14 Abrasion is an old surgical technique in dermatology, first used in 1905 for the treatment of depressed scars.19 Over the years it has improved and had its indications expanded, including its use in the nail plate. Unlike the usual sample collection, which has limitations such as patient discomfort and difficulty in obtaining enough samples from the more proximal part of the lesion, this method helps in collecting scales, reducing those limitations.14,20
The present study was aimed at evaluating the use of onychoabrasion as an auxiliary method for the collection of material for the diagnosis of onychomycosis, and comparing results with those obtained using the traditional method.
A prospective study was carried out with 30 patientsfrom the Dermatology Ambulatory of the Hospital do Servidor Público Municipal de São Paulo, S.P., Brazil, who voluntarily sought care between the years of 2011 and 2012.
The study was approved by the Research Ethics Committee of the institution (Authorization No. 35/2011; Protocol 237/2011).
Patient selection
Thirty patients of both genders were selected, according to the following inclusion criteria: clinical suspicion of onychomycosis affecting any nail of the feet, with the following clinical forms: lateral and distal subungual onychomycosis, or total dystrophic onychomycosis. Absence of systemic or topical antifungal treatment within the previous six months. Agreement to participate in the study by signing the free and informed consent form. To be over 18 years old.
Sample collection
The patients selected were referred for the collection of material. Samples intended for diagnostic tests were collected in two ways. First, the affected nail was scraped on the free border according to the usual method, with a scalpel or curette.
Subsequently, the more proximal area of the lesion was identified in the same nail, and was then subjected to the onychoabrasion with the electric device Dremel-MultiPro® model 395, coupled to a disposable rotary sanding paper (Figure 1). The collection was then carried out in the abraded area (Figures 2 and 3). Before both samplings, the nail was cleansed with 70% alcohol. Each sample, regardless of the collection technique (distal or abrasion), was separated into two parts-one destined for the mycological examination and the other to the culture.
For the direct mycological examination, the samples were prepared with 20% potassium hydroxide, associated with 40% dimethyl sulfoxide, and then visualized under optical microscopy with 10-40x magnification.
Two culture media were used for the seeding of each material. The Sabouraud agar with chloramphenicol is a rich medium that allows the growth of dermatophytes, non-dermatophytes, and yeasts. The second medium used was the Sabouraud agar with chloramphenicol and cycloheximide (Mycosel), which is more selective, inhibiting the growth of yeast and non-dermatophyte fungi.
Statistical analysis
The result of the direct mycological examination provided three options: positive (when septate hyaline hyphae were visualized), and negative (in the absence of fungal structures). The third possibility corresponded to cases where such an examination could not be performed due to insufficient material.
Culture results were analyzed separately for Sabouraud agar and Mycosel. There were four possible results: positive, absence of growth, insufficient material, and contamination.
Positivity was achieved with the growth of dermatophyte fungi in the culture medium. In the absence of growth of any microorganism, the result was considered as absence of growth.
In cases where the material was insufficient, the culture could not be performed.
The growth in the bacteria culture medium, yeast and non-dermatophyte fungi, was deemed as a contamination. For performing certain calculations, the result of the culture result was classified into two major groups: those with positive results (corresponding to the cases where there was growth of dermatophytes), and those with negative results, which comprised the cases of absence of growth, insufficient material and contamination. For the data analysis, the McNemar test was used, assuming an alpha = 0.05. Results were considered significant if the calculated "p" was less than alpha = 0.05.
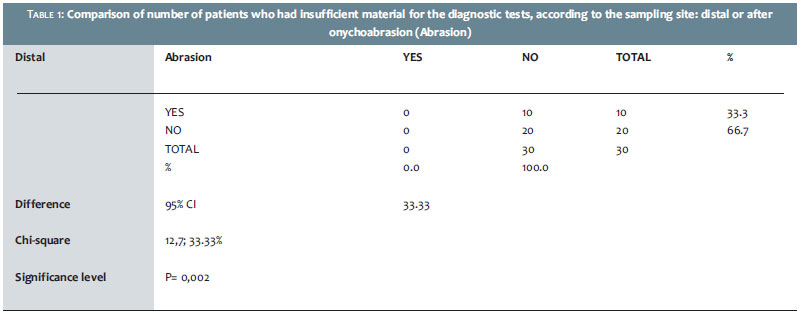
The collection of material from the distal part of the nail-the first step-provided positive direct mycological examination in 20 patients. In 10 cases, the examination could not be performed due to insufficient material (Table 1).
On the other hand, the sampling performed after onychoabrasion resulted in a positive direct mycological examination in 100% of cases (30 patients); there were no cases of insufficiency of material for analysis.
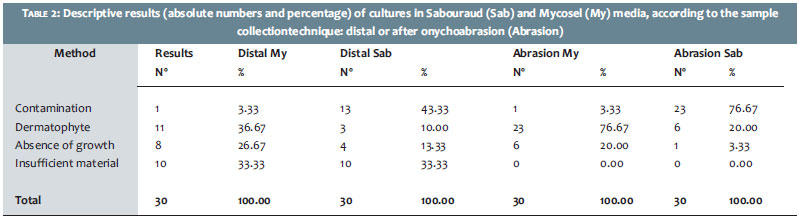
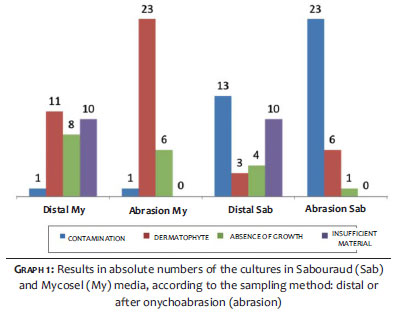
The culture in Sabouraud agar of the samples collected from the distal region of the nail showed contamination in 13 cases (43.33%), growth of dermatophyte fungi in 3 cases (10%), absence of growth in 4 (13.33%), and in 10 patients (33.33%) the culture was not performed due to insufficient material. The samples collected after the onychoabrasion and cultured in the same agar, showed contamination in 23 cases (76.67%), growth of dermatophytes in 6 cases (20%) and absence of growth in 1 case (3.33%).
The Mycosel agar culture of the samples collected from the distal region of the nail showed contamination in 1 case (3.33%), growth of dermatophytes in 11 (36.67%), absence of growth in 8 (26.67%), and in 10 patients (33.33%) culture was not carried out due to insufficient material. The samples collected after the onychoabrasion presented contamination in one case (3.33%), growth of dermatophytes in 23 (76.67%) and absence of growth in 6 (20.00%). (Table 2 and Graph 1)
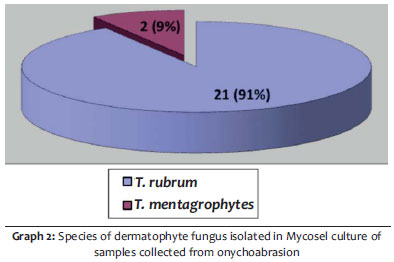
In these 23 cases where the results of the Mycosel culture was positive, Trichophyton rubrum was isolated in 21 patients, while Trichophyton mentagrophytes was found in only 2 cases. (Graph 2)
The results of the culture were then separated into two large groups. One with positive results, which corresponded to cases where there had been growth of dermatophyte fungi, and another with negative results, which comprised cases of contamination, absence of growth, and insufficient material.
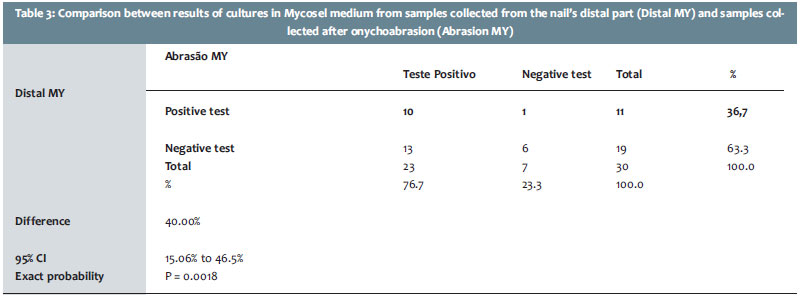
The results (positive and negative) of the agar culture with Mycosel of the distal collectionwere compared with the analogous culture, however with collection after onychoabrasion. The McNemar test was applied and revealed that the difference between the proportions in the results identified by the two methods were statistically significant (p = 0.0018). (Table 3)
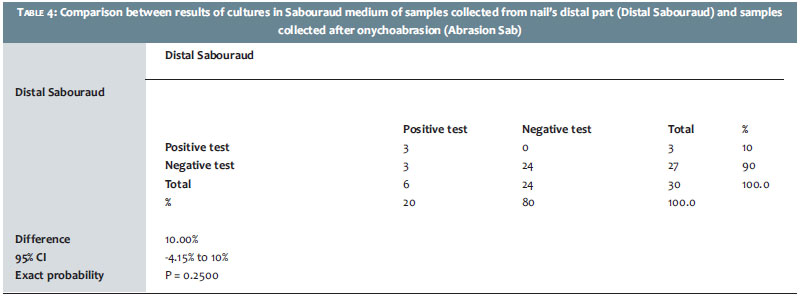
On the other hand, when performing the same comparison with Sabouraud culture, it was verified that the differences in results (positive and negative) between the distal collection and that carried out after onychoabrasion were not statistically significant (p = 0.25). (Table 4)
The study reveals a greater amount of positive results in samples collected after the onychoabrasion than that of the samples taken from the distal portion of the nail, with positivity ranging from 76.7% to 36.7% onychoabrasion. This difference was statistically significant (p = 0.0018).
The confidence interval of the difference shows that the onychoabrasion out performed the distal collection by 68% in the identification of fungi in Mycoselculture.
Despite the fact that 100% of the samples (excluding cases of insufficient material), both proximal and distal (onychoabrasion) have yielded positive direct mycological examination, the Mycosel culture medium had growth of dermatophyte fungi in only 66.7% of distal samples and 76.7% of the samples collected after the abrasion.
Most likely, this finding is due to the fact that the fungi found in direct mycological exams do not present viability in culture. The superiority of positive results in the culture of samples collected after onychoabrasion suggests that the sanding of the most proximal part of the lesion favors the collection of fungi with greater viability.
A study by Shemer et al. evaluated 194 patients with clinical suspicion of onychomycosis.13 The samples were collected from three different locations of the nail: proximal, middle, and distal parts. These samples were obtained both by traditional curettage and by the drilling of the nail with an electric device. Regardless of collection technique, the results showed that the sensitivity of the culture increased as the location of the collection became increasingly more proximal, agreeing with the finding of the present study.
Furthermore, the technique of drilling resulted in cultures with higher sensitivity in the three sampling sites, probably due to the fact that it provided better quality and a greater quantity of material. The onychoabrasion would also have the function of providing better samples for examination.
In the present study, Trichophyton rubrum (TR) was the most frequently isolated fungus, regardless of the collection site. In the samples originated from the onychoabrasion, TR was isolated in 91% of cases, followed by Trichophyton mentagrophytes, found in 9% of patients. In the collections in the distal part, TR was isolated in 100% of cases. This information is consistent with the data presented in the international literature, highlighting Trichophyton rubrum as the main agent of onychomycosis.
The comparison of the results of the Sabouraud medium showed no statistically significant differences between the samples of the distal part and those from after onychoabrasion, as observed in a Mycosel medium. The contamination corresponded to 76.67% of the onychoabrasion cultures and to 43.34% of the distal partcultures.
In contrast, dermatophytes fungi were isolated in only 20% of the onychoabrasion cultures and in 10% of the distal part cultures.
These findings are probably due to the fact that the Sabouraud culture medium is rich and non-selective, favoring the growth of microorganisms in a minimally restricted way.
Yeasts, dermatophyte, and non-dermatophyte fungi find a medium conducive to their development, hindering the identification of the pathogen and the contaminant. The bacteria generally have their growth inhibited by the presence of antibiotics, such as chloramphenicol, in most of the culture media.
On the other hand, the culture medium Mycosel is more selective due to the presence of cyclohexemide, a substance cable of partially or totally inhibiting the growth of yeast and non-dermatophyte fungi.
One of the already mentioned limitations of the direct mycological examination of samples collected in the usual manner (distal) is running into only scarce material for the exam. In 10 of the 30 patients selected for the study, there was insufficient material in the distal partcollection.
With the abrasion of the nail, in all 30 cases it was possible to obtain material for the direct mycological examination and culture. Thus, onychoabrasion emerges as an important resource for collecting material, therefore reducing the technical limitations of the usual collection method.
The study proves that onychoabrasion is an effective auxiliary method in the diagnosis of onychomycosis, for it provides better quality samples for analysis, making it superior to the traditional technique in identifying the fungus in both direct mycological examination and culture.
1. Jaffe R. Onychomycosis. Recognition, Diagnosis, and Management. Arch Fam Med. 1998;7(6):587-92.
2. Effendy I, Lecha M, Chauvin MF, Di Chiacchio N, Baran R. Epidemiology and clinical classification of onychomycosis. J Eur Acad Dermatol Venereol.2005;19(Suppl. 1):8-12.
3. Weinberg JM, Koestenblatt EK, Tutrone WD, Tishler HR, Najarian L. Comparison of diagnostic methods in the evaluation of onychomycosis. J Am Acad Dermatol. 2003;49(2):193-7.
4. Gupta AK, Ricci MJ. Diagnosing Onychomycosis. Dermatol Clin. 2006;24(3):365-9.
5. Lilly KK, Koshnick RL, Grill JP, Khalil ZM, Nelson DB, Warshaw EM. Cost-effectiveness of diagnostic tests for toenail onychomycosis: a repeated-measure, single-blinded, cross-sectional evaluation of 7 diagnostic tests. J Am Acad Dermatol. 2006;55(4):620-6.
6. Di Chiacchio N, Loureiro WR. Atlas de Onicomicoses: Diagnóstico, Principais Diferenciais e Tratamento.Rio de Janeiro: Elsevier;2011.
7. Zanardi D, Nunes DH, Pacheco AS, Tubone MQ, Filho JJS. Evaluation of the diagnostic methods of onychomycosis. An Bras Dermatol. 2008;83(2):119-24.
8. Karimzadegan-Nia M, Mir-Amin-Mohammadi A, Bouzari N, Firooz A. Comparison of direct smear, culture and histology for the diagnosis of onychomycosis. Australas J Dermatol. 2007;48(1):18-21.
9. Araújo AJG, Bastos OMP, Souza MAJ, Oliveira JC. Onychomycosis caused by emergent fungi: clinical analysis, diagnosis and revision. An Bras Dermatol. 2003;78(4):445-55.
10. Meireles TEF, Rocha MFG, Brilhante RSN, Cordeiro RA, Sidrim JJC. Successive Mycological Nail Tests for Onychomycosis: A Strategy to Improve Diagnosis Efficiency. Braz J Infect Dis. 2008;12(4):333-7.
11. Brilhante RS, Cordeiro RA, Medrano DJ, Rocha MF, Monteiro AJ, Cavalcante CS, et al. Onychomycosis in Ceará (Northeast Brazil): epidemiological and laboratory aspects. Mem Inst Oswaldo Cruz. 2005;100(2):131-5.
12. de Chauvin MF. New diagnostic techniques. J Eur Acad Dermatol Venereol. 2005;19(Suppl. 1):20-24.
13. Shemer A1, Trau H, Davidovici B, Grunwald MH, Amichai B. Collection of fungi samples from nails: comparative study of curettage and drilling techniques. J European Academy of Dermatology and Venereology 2007;22(2):182-5.
14. Tosti A, Piraccini BM, Di Chiacchio N. Doenças das Unhas. São Paulo: Luana Livraria Editora; 2007.
15. Hay RJ, Baran R. Onychomycosis: A proposed revision of the clinical classification. J Am Acad Dermatol. 2011;65(6):1219-27.
16. Lawry MA, Haneke E, Strobeck K, Martin S, Zimmer B, Romano PS. Methods for diagnosing onychomycosis: a comparative study and review of the literature. Arch Dermatol 2000;136(9):1112-6.
17. Olive JCI, Araújo AJG. Avaliação de novas técnicas diagnósticas em onicomicose. Periódico de Dermatologia - Volta Redonda. 2004;I(1):15-24.
18. Raymond R, Pihet M. Conventional Methods for the Diagnosis of Dermatophytosis. Mycopathologia. 2008;166(5-6):295-306.
19. Costa IMC, Igreja ACSM, Costa MC. Dermoabrasão, Microdermoabrasão e Microagulhamento. In: Kadunc B, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, et al, editores. Tratado de Cirurgia Dermatológica, Cosmiatria e Laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier;2012.p.441.
20. Di Chiacchio N, Kadunc BV, Almeida ART, Madeira CL. Nail Abrasion. J Cosmet Dermatology. 2004;2(3-4):150-2.
This study was performed at the Hospital do Servidor Público Municipal de São Paulo (HSPM-SP) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}