


Gabriela Casabona1; Carla Presti2; Merlei Manzini3; Carlos D'Apparecida Santos Machado Filho4
Keywords: PULSED RADIOFREQUENCY TREATMENT; REJUVENATION; SKIN AGING; ABLATION TECHNIQUES; LASER COAGULATION; LASERS.
Personal appearance is a human preoccupation dating back to ancient times, one that has led to the creation of numerous cosmetic practices.1 The skin, being the most evident organ of the human body, becomes a marker of chronological age and appearance, and is an important factor in self-esteem and a good quality of life. Patients increasingly seek treatments aimed at delaying the effects of aging, whether they are related to advancing age or caused by environmental affects.2
The palpebral region is one of the first body sites to suffer such effects, not only because the local dermis is thin (the total thickness of skin varies between 400 and 800 microns), but also because it is a small cosmetic area, where the action of the muscles promotes resorption of the deep fat and favors the breakdown of the periorbital collagen fibers.3 Rejuvenation of this area involves much more than just the improvement of the skin; local volumization, correction of muscle hypertrophy, and improvementof the tarsal support are also necessaryand can, in general, imply invasive techniques, such as blepharoplasty, botulinum toxin, and cutaneous filling.3
In order to be successful at rejuvenating this very important cosmetic area, an accurate examination of the eyelid and its supporting structure-which corresponds to the posterior lamella (septum, fat pads, and tarsal), and the anterior lamella (skin, subcutaneous tissue, and orbicularis muscle)-should be carried out.4 One of the major concerns when using any technique for rejuvenating the skin of the lower eyelid is not to cause retraction of the anterior lamella to the extent that it causes ectropion as a complication. Thus, the skin depth reached during the technique and density are of great importance.5 Other minor complications, such as hyperpigmentation, persistent erythema, and hypochromia, are also described. Chemical peels with trichloroacetic acid (TCA) and phenol (the formula described by Baker and Gordon) were the first techniques developed for the improvement of the skin of the lower eyelid.6 The 50% TCA or phenol peeling produces coagulation of proteins up until the papillary or reticular dermis, and its penetration is often not predictable, as in laser technologies.7 In most cases, complications are related to infection, focal hypopigmentation, postinflammatory hyperpigmentation, and persistent erythema, but not ectropion.8 Over time, some ablative technologies, such as radiofrequency ablation and non-fractional CO2 laser, have been widely used. These technologies have conferred greater precision to the treatment, reaching depths greater than 1mm, meaning thermal lesion of all the anterior lamella was achieved. However, they often cause ectropion.9 Major drawbacks of these techniques were also the recovery time after the procedure (seven to ten days) and complications that, according to Alster, in a survey conducted in 2003 with 500 cases of non-fractional CO2, amounted to 37%.10With the onset of fractional technologies, many of the above problems were solved.11 Complications of hyperpigmentation and rare cases of ectropion decreased from 40% to 9%. The recovery time decreased, however there was often a need for more than one session to achieve similar results.12 This is one of the factors that encouraged the authors to search for new therapeutic possibilities for facial rejuvenation, including ablative fractional radiofrequency (FARF).
The onset of high-frequency electrosurgery took place in 1978, when Maness et al.13 defined the ideal alternating current frequency to cut and promote coagulation, i.e. an electric current that alternatesits polarity in 4,000,000 cycles/second. This frequency is in therange of FM radio, what gave rise to its being called ‘radiofrequency'. High frequency alternating currents generate magnetic fields, which are released at the tip of the electrode that is attached to the device, in a way that the action of the system will take place through electromagnetic waves rather than through electrical current-which explains a very similar effect to that of the CO2 laser. It is, therefore, a cutting and/or coagulation process depending on the type of current selected. If the current is slowed, it will have a coagulation effect; if it is purely sinusoidal, it will have a cutting effect; if it is a slowed sinusoidal current, it will both cut and promote coagulation. The intensity of the "brakes" exerted on the current (low blend or high blend) determines the intensity of the coagulation or thermal effect. The high frequency causes the positive and negative charges within the cell to oscillate, raising the temperature rapidly to 100ºC, causing its vaporization. The type of tip used determines the concentration of energy on a specific-point; therefore, the smaller the area of contact (electrode's tip), the greater the ablation or evaporation power. There are three application models: Cut (20% coagulation and 80% cut), Low Blend (50% coagulation and 50% cut) and High Blend (80% coagulation and 20% cut).
Since Rox Anderson14 discovered the advantages of the fractionation of some forms of light for skin rejuvenation, several other studies have been performed, and today there are different types of laser, radio frequency, and infrared devices that use this property as a way to render the treatments safer and more effective. As a result, the development of fractionating FARF began. The first successful attempts to use non-fractional ablative radiofrequency for rejuvenation were used for the resurfacing of the lower eyelid. However, such procedures are very dependent on the operator and in these first attemptslead to complications due to the excessive thermal effect.
Radiofrequency is radiation between 30KHz and 300MHz, within the electromagnetic spectrum that generates heat. This type of heat reaches the deeper tissues, creating energy and strong heat in the deeper layers of the skin, keeping the surface cool and protected, causing the contraction of existing collagen fibers and stimulating the formation of new fibers, making them more efficient in supporting the skin. The thermal effects of radiofrequency cause denaturation of collagen, promoting the immediate and effective contraction of its fibers, activating fibroblasts and leading to neocollagenesis, to the reorganization of collagen fibers and to the subsequent remodeling of the tissue. 15, 16 FARF is a new procedure that uses a random energy fractionation system that observes the tissue thermal relaxation time, similar to that which occurs with fractional CO2 laser, however using a different energy source.17, 18
To demonstrate, through the treatment of the lower eyelid with FARF, the tightening effect, i.e.the contraction of the tissue with improvement in the texture and in the appearance of the skin, and the rejuvenation entailed.
To demonstrate through an anatomical pathological study, the thermal effect of FARF on the skin that underwent this procedure, attempting to describe it quantitatively.
A prospective study was carried out with 20 patients randomly selected from those who sought periorbital rejuvenation and presented with lower eyelid skin redundancy, at the Dermatology Ambulatory of the Faculdade de Medicina do ABC. FARF was indicated as the method to improve the lower eyelid skin. Cases of a protrusion of fat pads were treated with transconjunctival blepharoplasty in order for the skin to remain untouched. The included patients were female patients who had phototypes I - IV, with ages between 40 and 65 years. They patients were instructed to use SPF 50 sunscreen for at least 30 days before the procedure and suspend the use of topical retinoids a week before. The study was conducted according to the guidelines recommended by the Declaration of Helsinki 2000,which was updated in 2008. All patients signed a free and informed consent form for the procedure and a term authorizing that photographic records could be made. In one patient, who concomitantly underwent upper blepharoplasty, the authors took photographs of the skin to be removed with the same configuration used in the lower eyelid. The specimen was sent for histological study, carried out in vertical and horizontal sections stained with hematoxylin and eosin.
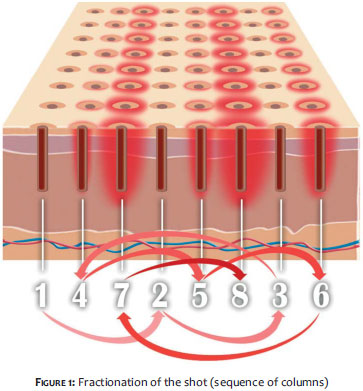
All procedures were performed under infiltrative local anesthesia with 30ml 0.9% saline solution associated with 10ml 2.0% lidocaine, 0.4 ml 1/10,000 epinephrine, and 1.0ml 8.4% sodium bicarbonate. The patients underwent a single session of fractional ablative radiofrequency with 3 passes in the lower eyelid, meaning that 80% of the region's skin was treated. The skin was humidified with sterile saline and gauze, carefully in order not to allow an excess of saline on the skin's surface (liquid film) thus avoiding possible burns in the site caused by the heating of this liquid film. The device, Wavetronic 5000 (Loktal Medical Electronics Industria e Comércio Ltda, São Paulo, SP, Brazil), was coupled with the megapulse system HF FRAXX (Loktal Medical Electronics Industria e Comércio Ltda.), which has an electronic circuit for fractioning energy. A pen with 64 microneedles 0.2mm thick and 0.8mm long, mounted on a teflon body, divided into eight columns of eight needles each, were in turn connected to the megapulse system. The laser parameters were then set as follows: 60% of power in the Wavetronic 5000's potentiometer (corresponding to 46watts) and on the ‘Cut'option. The pen was always kept perpendicular and touching the damp skin. The overlap between one shot and another was 2mm, aiming at a fairly uniform application. When the applicator compresses the shooting pedal, the 64 needles are not energized at the same time, but in columns of eight needles, according to a preset sequence (in the present study's case, the sequence number 2 was used). That selection is made through the ‘P' key (program), followed by the ‘E' key (enter). The delivery of energy is randomized, i.e. it alternates between columns in a predetermined way, such that two adjacent columns are not energized sequentially, allowing cooling between shots and less thermal damage (Figure 1).
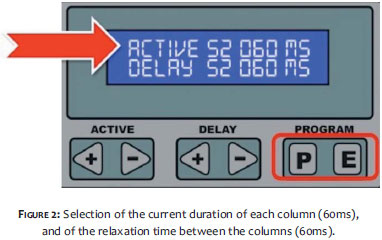
Through the ACTIVE key-which controls nothing more than the duration of the active current or the time during which the skin is exposed to heat-the megapulse system allows the selection of the duration of the current in milliseconds (ms), for each column formed by 8 needles. The possible range is 0 to 320ms (60ms was used in the present study). Moreover, the system also allows the variation of the resting time or thermal relaxation time of the eight columns through the DELAY key, which ranges between 60 and 320ms (60ms was used in the present study). Based on serial applications carried out earlier in pig skin, it was found that the optimal value for the ACTIVE and DELAY keys was of 60 ms in order for the thermal injury to resemble that of the fractional CO2 laser. The initial selection of those parameters was made considering an amount of energy sufficient (345mJ) for a safe treatment (Figure 2). Each of the pen's shots will cause 64 perforations in the skin (Figure 3). The post-treatment care was carried out using 5% dexpanthenol solution in the treatment site several times a day for five days, with the SPF 50 sunscreen being continued. 19
The clinical results were evaluated through the comparison of the pictures taken before and 30 days after the procedure; the patients also answered a questionnaire regarding their satisfaction, which could be classified into three categories: very satisfied, satisfied, dissatisfied.
The histologic evaluation was carried out by measuring the thermal effect on the skin, in millimeters (mm).
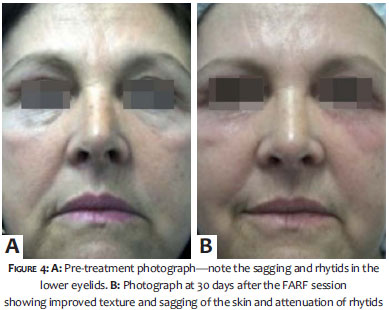
Assessing the photographs taken before and after the procedure with a single session of fractional radiofrequency, it was possible to observe the contraction effect in the skin of the lower eyelid, with the consequent improvement in skin texture and reduction of local rhytids (Figures 4 and 5).
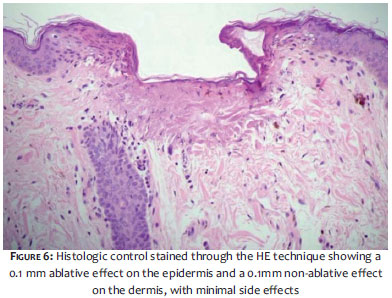
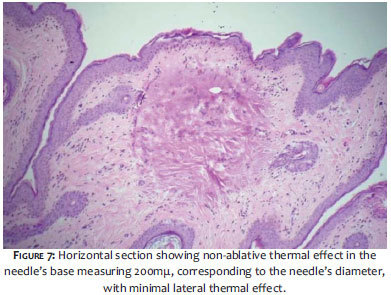
Of the 20 patients, 18 were very satisfied (90%) and only two (10%) indicated that they were only just satisfied with the results. Two (10%) had post-inflammatory hyperpigmentation in the treated area, which resolved after topical use of the combination hydroquinone/tretinoin for 15 days. In all cases, the crusts formed within two days after the procedure and took an average of 10 days to disappear. The erythema had a mean duration of 17 days, and the swelling lasted three days. Regarding the histologic study of the vertical sections, it was observed that the perforation of the needle in the epidermis, i.e. the ablative perforation, measured 0.1mm (100mµ), and the thermal effect on the dermis, or the destruction of the non-ablative effect was 0.1mm (100mµ) deep, with negligible lateral thermal effect (Figure 6). In the horizontal section, a thermal effect could be observed in the dermis underlying the needle's perforation and the 1mm spacing between the needles, with total preservation of tissue between the perforations (Figure 7).
FARF constitutes a further possibility for the treatment of aging skin. It is a procedure that emits waves that reach the deeper layers of the skin, generating energy and strong heat over them, nevertheless keeping the surface cool and protected. It was possible to observe that the procedure can achieve the depth of 100 microns, i.e. it reaches the papillary dermis, where it causes ablation and coagulation of surrounding proteins due to the residual thermal damage. This leads to both the contraction of existing collagen fibers and stimulates the formation of new fibers, making them more efficient in supporting the skin. The present study's result shows that this procedure can be considered a useful treatment for periorbital rejuvenation, a fact that has motivated several ongoing studies in an attempt to demonstrate these effects not only on the eyelids, but across the face, acne scars, unaesthetic scars, and recent and old atrophic striae. The side effects were easily resolved with expectant conduct, adequate hydration, sun protection, and topical post-operative whitening therapy. 20 This technique has allowed a considerably interesting rejuvenation effect at low cost and with low complication rates. Due to the fact that the device has no consumables and does not necessarily need coolers and even a light source, it is more affordable and easier to maintain as compared to laser devices, offering very similar results. 21, 22 The treatment of periocular aging skin is challenging, and new technologies have been emerging for a long time, most of them with poor results. CO2 laser has been standing out recently due to both the cosmetic results and the low incidence of post-operative side effects, as well as for the quick recovery time. However, it is an expensive treatment, which limits its use. 23-27
Some of the limitations of the present study reside in the fact that only one radiofrequency session was carried out, which may affect the actual final result. There are ongoing studies showing significant clinical results with the number of sessions ranging from 3 to 5. We cannot say, therefore, that the results obtained in the present study were the best possible. Furthermore there is no consensus yet about the ideal number of passes nor the minimum or maximum number of sessions needed for a result that could be considered excellent.
There is still much to be studied regarding this new therapeutic resource, such as the analysis of the treated area in the long run with anatomical pathology, definition of standards for the energy applied, new therapeutic possibilities, and even comparisons with the parameters used in CO2 laser, for the same scope.
As in other already published studies, FARF proved to be safe, efficacious, and cost-effective in the present study, and among the tools available in the periorbital rejuvenation armamentarium. 6 Further studies should be carried out in order to determine the best parameters and optimal number of sessions to achieve the best result with the lowest rate of side effects.
We would like to thank Dr. Gilles Landmann (pathologist) for carrying out the histologic tests.
1. Tierney EP1, Hanke CW. Recent trends in cosmetic and surgical procedure volumes in dermatologic surgery. Dermatol Surg. 2009;35(9):1324-33.
2. Louarn C. Midface region: functional anatomy, ageing process, indications and concentric malar lift. Ann Chir Plast Esthet. 2009;54(5):411-20.
3. McKinney P, Zukowski ML, Mossie R. The fourth option: a novel approach to lower-lid blepharoplasty. Aesthetic Plast Surg. 1991;15(4):293-6.
4. Roberts TL 3rd. Laser blepharoplasty and laser resurfacing of the periorbital area. Clin Plast Surg. 1998;25(1):95-108
5. Nanni CA1, Alster TS. Complications of carbon dioxide laser resurfacing. An evaluation of 500 patients. Dermatol Surg. 1998;24(3):315-20.
6. Glogau RG1, Matarasso SL. Chemical peels. Trichloroacetic acid and phenol. Dermatol Clin. 1995;13(2):263-76.
7. Stuzin JM. Phenol peeling and the history of phenol peeling. Clin Plast Surg. 1998;25(1):1-19.
8. Dailey RA, Gray JF, Rubin MG, Hildebrand PL, Swanson NA, Wobig JL, et al. Histopathologic changes of the eyelid skin following trichloroacetic acid chemical peel. Ophthal Plast Reconstr Surg. 1998;14(1):9-12.
9. Haina D, Landthaler M, Braun-Falco O, Waidelich W. Comparison of the maximumcoagulation depth in human skin for different types of medical lasers. Lasers Surg Med. 1987;7(4):355-62.
10. Tanzi EL, Alster TS. Single-pass carbon dioxide versus multiple-pass Er:YAG laserskin resurfacing: a comparison of postoperative wound healing and side-effect rates Dermatol Surg. 2003 Jan;29(1):80-4.
11. Manstein D, Herron GS, Sink RK, Tanner H, Anderson RR. Fractional photothermolysis: a new concept for cutaneous remodeling using microscopic patterns of thermal injury. Lasers Surg Med. 2004;34(5):426-38.
12. Neumann KC, Baca ME, Piazza RC 3rd, VanderWoude DL, Renucci JD. Outcomes of fractional CO2 laser application in aesthetic surgery: a retrospective review. Aesthet Surg J. 2010;30(6):845-52.
13. Maness WL, Rober FW, Clark RE, Cataldo E, Haddad AW. Tissue damage from electrosurgical power output variations in hamster tongues .J Prosthet Dent. 1979;42(4):456-60
14. Alexiades-Armenakas MR, Dover JS, Arndt KA. Fractional laser skin resurfacing. J Drugs Dermatol. 2012;11(11):1274-87.
15. Maness WL, Roeber FW, Clark RE, Cataldo E, Riis D, Haddad AW . Histologic evaluation of electrosurgery with varying frequency and waveform. J Prosthet Dent. 1978;40(3):304-8.
16. Bloom BS, Emer J, Goldberg DJ. Assessment of safety and efficacy of a bipolar fractionated radiofrequency device in the treatment of photo-damaged skin. J Cosmet Laser Ther. 2012;14(5):208-11
17. Tierney EP, Hanke CW, Petersen J. Ablative fractionated CO2 laser treatment of photoaging: a clinical and histologic study.Dermatol Surg. 2012;38(11):1777-89.
18. Kohl E1, Meierhöfer J, Koller M, Zeman F, Klein A, Hohenleutner U, et al. Fractional carbon dioxide laser resurfacing of rhytides and photoaging: a prospective study using profilometric analysis. Br J Dermatol. 2013 Dec 26. doi: 10.1111/bjd.12807. [Epub ahead of print].
19. Wanitphakdeedecha R1, Phuardchantuk R, Manuskiatti W. The use of sunscreen starting on the first day after ablative fractional skin resurfacing. J Eur Acad Dermatol Venereol. 2013 Dec 10. doi: 10.1111/jdv.12332. [Epub ahead of print]
20. Hruza G, Taub AF, Collier SL, Mulholland SR. Skin rejuvenation and wrinkle reduction using a fractional radiofrequency system. J Drugs Dermatol. 2009;8(3):259-65.
21. Cho SI, Chung BY, Choi MG, Baek JH, Cho HJ, Park CW, Lee CH, Kim HO. Evaluation of the clinical efficacy of fractional radiofrequency microneedle treatment in acne scars and large facial pores.Dermatol Surg. 2012;38(7 Pt 1):1017-24.
22. Ancona D, Katz BE. A prospective study of the improvement in periorbital wrinkles and eyebrow elevation with a novel fractional CO2 laser-the fractional eyelift. J Drugs Dermatol. 2010;9(1):16-21.
23. Luo YJ, Xu XG, Wu Y, Xu TH, Chen JZ, Gao XH, et al. Split-face comparison of ultrapulse-mode and superpulse-mode fractionated carbon dioxide lasers on photoaged skin.J Drugs Dermatol. 2012;11(11):1310-4.
24. Passeron T. Lasers. Ann Dermatol Venereol. 2012;139 (Suppl 4):S159-65.
25. Tierney EP, Hanke CW. Ablative fractionated CO2, laser resurfacing for the neck: prospective study and review of the literature. J Drugs Dermatol. 2009;8(8):723-31.
26. Hunzeker CM, Weiss ET, Geronemus RG. Fractionated CO2 laser resurfacing: our experience with more than 2000 treatments. Aesthet Chan HH, Manstein D, Yu CS, Shek S, Kono T, Wei WI. The prevalence and risk factors of post-inflammatory hyperpigmentation after fractional resurfacing in Asians. Lasers Surg Med. 2007;39(5):381-5.
27. Chan HH, Manstein D, Yu CS, Shek S, Kono T, Wei WI. The prevalence and risk factors of post-inflammatory hyperpigmentation after fractional resurfacing in Asians. Lasers Surg Med. 2007;39(5):381-5.
This study was performed at the Faculdade de Medicina da Universidade de São Paulo (FMUSP) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}