


Adilson Costa1; Mário Cézar Pires2; Lincoln Helder Zambaldi Fabrício3; Liliana Bechelli de Oliveira Torloni4; Stephanie Langen5; Erica Bruder Botero6
Keywords: HYDRATION, DESICCATION, AQUAPORINS.
The skin playsimportant roles, the complexity and soundness of which contribute to the maintenance of the body's homeostasis. Nevertheless, these properties only function at the highest level if the skin is in full, normal operating condition and receiving adequate care.1
Two basic processes act in concert when this care occurs: cutaneous cleaning and moisturizing. Cleaning contributes to the removal of the external debris, natural cutaneous secretions, and microorganisms. Cutaneous hydration, in turn, is responsible for maintaining the water content in the epidermis, keeping the skin barrier in good condition. 2, 3
The epidermal barrier is composed of the cellular protein matrix (a weft of interwoven keratinocytes arranged in layers, limited superficially by corneocytes) and the intercellular matrix (lipid bilayer), which are responsible for maintaining the normal water balance of the skin, while respecting its sectoral characteristics (the superficial epidermal cell layers repel water, while the deeper layers retain it), which are essential for the cutaneous balance.4
In addition to these structures, however, chemical particles (NMF - natural moisturizing factor, intercellular lipids, ion pumps and aquaporins) embedded in these two compartments are equally important and help to keep the cutaneous hydration balanced.5
The NMF is a keratinocytic component, being formed by a set of hygroscopic structures that interact to retain water in the integument.1, 4, 6
The intercellular lipids (originated from the nucleated keratinocytes and arranged in the stratum corneum) are bipolar structures, which control intercellular permeability and water movement. Such fatty structures seal the NMFs in the corneocytes, keeping the intercellular water content.4
The ion pumps establish the basic electrolyte balance. The ions play an active role in maintaining the water content of the intra-and extracellular medium. This fact is due to the existence of differences in their concentrations in these two media. Such differences are maintained thanks to the diffusion of these molecules facilitated through ionic channels present in all human cells. The Na+K+ pump is the best known of these channels, which along with the K + pump, helps to maintain the intracellular and extracellular concentrations of these ions.1, 6
Finally, the aquaporins are transmembrane proteins initially described in erythrocytes in 1991, and which currently include 13 types. In the human epithelium, aquaporin-3 (AQP3) stands out for being permeable to water and molecules such as glycerol and urea, important skin moisturizing agents, called aquaglyceroporin. It is present in the intestinal, respiratory, cutaneous, kidney, erythrocyte and chondrocyte cells. In the skin, it is located in the keratinocytes of the epidermis and represents a permeability channel, controlling the hydration.1, 7-9
The deletion of the AQP3 gene in mice resulted in decreased water in the stratum corneum, impairing cutaneous elasticity, and complicating the healing of wounds. This suggests a possible regulation of the differentiation and proliferation of keratinocytes by this protein. The AQP3 is also expressed in human skin fibroblasts, and epidermal growth factors increase their expression and cell migration. As a result, it seems to be a factor in the migration of fibroblasts that are involved in the wound repair process. 1, 10
In the case of disorder in one of these barrier components, there is an increase in transepidermal water loss (TEWL), causing cutaneous xerosis, with its classic signs and symptoms.1, 4-6
The frequent use of moisturizers is still the treatment of choice for this condition; the primary goal of the treatment is to relieve cutaneous xerosis and irritation, preventing the recurrence of such pictures. The formulation of the mosturizing product nevertheless must be carefully observed, since its effectiveness is directly related to it. 11-13
Moisturizers are classified according to the way their active ingredients work; these categories are: occlusive, humectants, emollients, and protein repairers.
Most often, commercial products use raw materials of each of these classes in their formulations to increase effectiveness and therapeutic success. 6, 14, 15
Occlusive moisturizers delay evaporation and epidermal water loss by forming a hydrophobic film on the skin's surface and in the interstitium between the surface's keratinocytes. Humectant moisturizers retain water in the stratum corneum, either by pulling it from the dermis or pulling it from the environment (in conditions where the atmospheric humidity is greater than 70%). Emollient moisturizers are rich in substances capable of filling the intercorneocytic clefts,thus retaining water in that layer. 6
The protein repairing moisturizers help to repair damaged dermal protein structures or stimulate their production. They act as moisturizers, for they assume an osmotic role, soaking up water and retaining it in the epidermis and dermis. 1, 6
Finally, recent studies with substances capable of stimulating the expression of aquaporins have also shown considerably promising results regarding epidermal hydration, aggregating clinical benefits in the approach of cutaneous xerosis. 1, 7, 9
The product investigated in the present study contains raw materials of all moisturizing classes in its formula (occlusive, humectant, and emollients agents), including ceramides, omega 3, 5, 6, and 7, glycerine, Imperata cylindrica, and erythritol and homarine, all responsible for stimulating aquaporin channels, and generating a flow of water to the site with the greatest hydration need.
The present study was aimed at evaluatingthe efficacy and safety of using a moisturizing cosmetic product in patients bearing cutaneous xerosis, based on the clinical evaluation of the investigator physician and on the subjective evaluation of the volunteer, in addition to a research (through specific scores) and corneometry, pH and TEWL measurements.
A clinical, multicenter, phase IV, non-placebo controlled, prospective study was carried out with 100 volunteers, who evaluated the efficacy and safety of using the product both from the clinical perspective (through medical analysis) and the subjective standpoint (through the analyses of the volunteers themselves). From the 100 selected volunteers, 30 also underwent additional instrumental analyses: corneometry (assessment of skin hydration), pH metry (assessment of skin's pH) and TEWLmetry (assessment of the transepidermal water loss).
The inclusion criteria were: volunteers of both genders, 18 to 70 years old, with cases of simple xerosis, ichthyosis vulgaris, senile xerosis, and xerosis caused by endocrinopathies. The following variables were also used as inclusion criteria: photo-type I to IV (Fitzpatrick classification); contraceptive use in patients of child bearing age; capacity to adhere to the study's protocol and follow-up; absence of a history of allergic reactions to the product being tested; absence of underlying diseases that could impair the study's evaluation or follow-up; good understanding and respect of the instruction for not using concomitant products, and not to undergo intense exposure to the sun during the course of the study.
The study was conducted according to the patient's safety recommendations issued by the Declaration of Helsinki 2000.
Individuals who were deemed to have developed a personal risk or interference in the objectives of the study, individuals with skin lesions in the areas to be assessed, patients with signs of intense sun exposure or who were pregnant or lactating, were excluded at the discretion of the investigators.
Thus, the studied patients were instructed to use the product under investigation (Hydraporin,® Mantecorp IndústriaQuímica e Farmacêutica S/A, Rio de Janeiro/RJ, Brazil), for 90 days (once at night, after bathing, at least 30 minutes before bedtime).
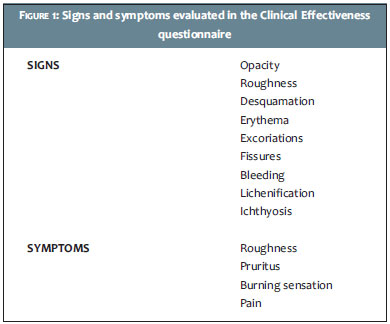
The results were evaluated through a clinical efficacy questionnaire (Figure 1) on days 0, 30, 60, and 90, with information on dryness, hydration, desquamation, itching and smoothness. At all visits the volunteers were also objectively evaluated on the inner side of the right arm (three measurements) and anterior face of the right leg (three measurements) with the assistance of corneometry, TEWL-metry and pH-metry.
Of the 100 volunteers previously selected, only 86 completed the study, with the following characteristics: phototype II (17.4%), phototype III (59.3%), phototype IV (23.3%), women (94.2%) and mean age = 44 years (range = 18-70 years old). Of the participants, 97% had relief of symptoms during the 90 days of product use (p < 0.0001).
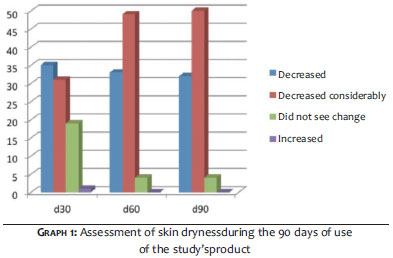
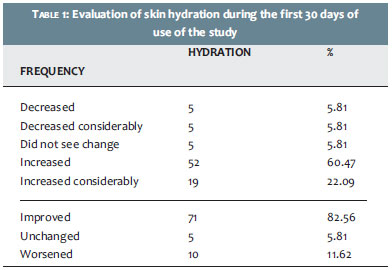
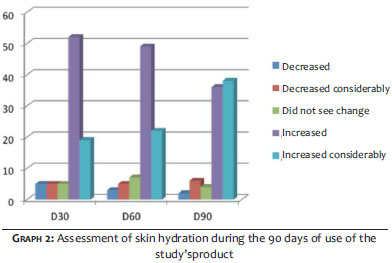
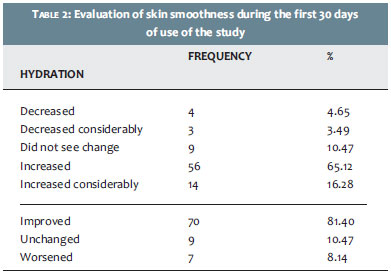
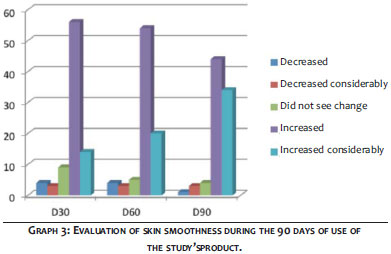
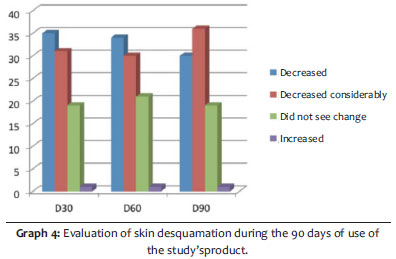
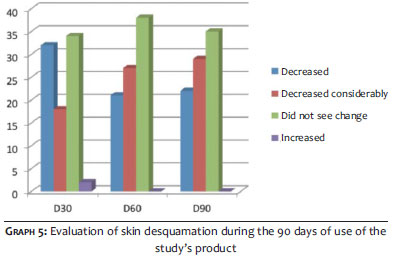
In the first 30 days of product use, 94%of patients showed improvement in dryness (Graph 1); 82.5% in hydration (Table 1 and Graph 2); 81.4% in smoothness (Table 2 and Graph 3); 76.75% in desquamation (40%did not present that symptom on D0) (Graph 4); and 58.14% in itching (60%did not have that symptom on D0) (Graph 5).
During the 90-day study, all subjective efficacy variables analyzed showed clinical improvement. The results described below were found in the analysis of objective variables.
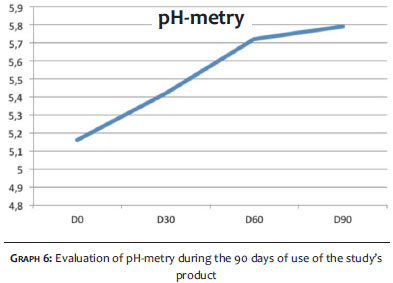
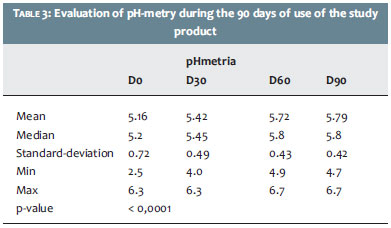
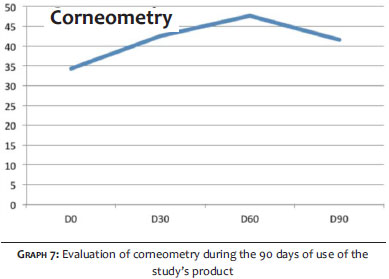
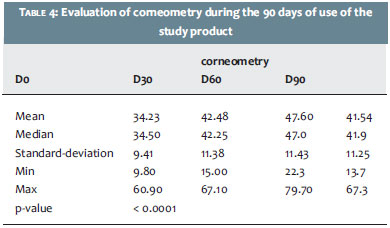
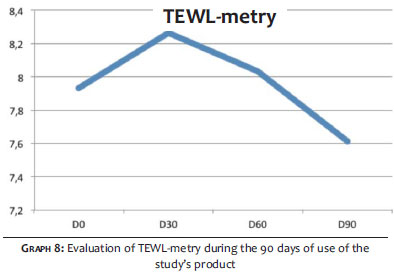
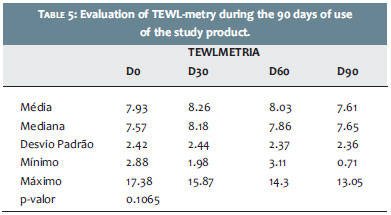
The pH (Graph 6 and Table 3) remained at physiological standards (D0: 5.16, D30: 5.42, D60: 5.72, D90: 5.79). The corneometry analysis (Graph 7 and Table 4) evidenced significant increase in the level of skin hydration (D0: 34.93, D30: 42.48, D60: 47.60, D60: 47.60). Both the pH-metry and the corneometry presented a statistically significant difference (p-value < 0.001). The TEWL-metry (Graph 8 and Table 5) ranged from D0: 7.93 to D90: 7.61, although without statistical significance (p-value = 0.1065).
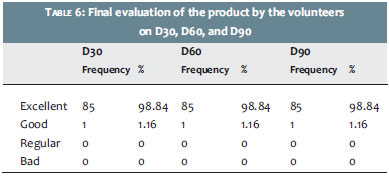
In the final evaluation, 100% of participants rated the product as excellent (98.84%) and good (1.16%) (p-value < 0.001) (Table 6).
The role of the stratum corneum isas part of the epidermal barrier, protecting not only against chemical agents, but also against microorganisms. A healthy stratum corneum has 20-35% water in its composition. If this amount is less than required, the skin surface will present fissures, thereby fulfilling the barrier's function insufficiently and inadequately. Dry skin can therefore be defined as a state where there is water loss from the stratum corneum, clinically compromising it.16
Cutaneous xerosis, however, is not a static mechanism. There are several intrinsic and extrinsic conditions that contribute to its manifestation, including changes in environmental humidity, skin degreasing (hot baths, excessive soap), solar radiation, emotional stress, physical trauma, and use of retinoids.17
In addition to these conditions, xerosis can also be secondary to skin diseases and physiological conditions typical of human beings, such as psoriasis, atopic dermatitis, senility,menopause, diabetes mellitus, hypothyroidism, and leprosy.18-20
Under normal physiological conditions, the stratum corneum has a capacity for recovery. The stimulus of the removal of lipids increases the desquamation of corneocytes, triggering a series of phenomena, among which are the increased secretion of lamellar bodies (which in turn stimulates lipid synthesis), and the stimulation of the maturation of corneocytes (with the conversion of profilaggrin into filaggrin, aggregating keratin filaments). The skin remains dry when these normal compensatory mechanisms do not outweigh the stimuli that induce the loss of water. 17, 21
Cutaneous xerosis becomes clinically evident when the water content in the stratum corneum is less than 10%. It manifests as cutaneous roughness, desquamation, fissures, tension, redness, and occasionally bleeding. It often causes significant discomfort and important cosmetic alterations, which demand appropriate treatment. 17
The use of body moisturizers is undoubtedly the first step for the relief of signs and symptoms of this condition. The present paper offers the clinical outcome of approaching xerosis with the use for 90 days of an innovative moisturizing formula-especially due to the presence of substances in its formulation that stimulate the sound functioning of aquaporins.22 Using Hydraporin,® there was complete or marked clinical improvement in 89.54% of volunteers, according to the medical evaluation. There was an average reduction from 3.83 to 0.55 in the clinical signs and symptoms ratings during the 90 days of the study (p-value < 0.0001). This assessment was based on a clinical questionnaire, in which the signs and symptoms considered by the physicians were: opacity, roughness, desquamation, erythema, excoriation, fissure, bleeding, lichenification, ichthyosis,pruritus, burning sensation,and pain. For each item (when it occurred) a rating was assigned. Therefore, the final sum of the ratings was directly related to the severity of the xerosis.
According to the corneometry evaluation, the objective method for assessing skin hydration, there was a statistically significant increase after 90 days of use, with average ratings ranging from 34.23 in D0 to 41.54 in D90.
Regarding the assessment of transepidermal water loss, measured through TEWL-metry, there was an increase in the first 30 days. This occurred due to the fact that the moisturizer in question had a proportionally smaller amount of occlusive substances than emollients and humectants, in its formulation. Thus, due to dryness of the volunteers' skin, with the start of the use of Hydraporin® there was a recruitment of water from the dermis to the epidermis by the moisturizing substances, slightly increasing the transepidermal water loss (D0: 7.93 and D30: 8.26). However, shortly after, when the skin was already hydrated, there was a progressive reduction of the TEWL. On D60 it rated 7.86 while at the end of the study it reached a rating lower than the initial (D90: 7.65).
The pH indices remained at physiological standards throughout the study, with the mean value ranging from 5.16 to in D0 to 5.79 in D90. It is important to note that the pH of a normal epidermis is slightly acidic, due primarily to sebum and sweat secretions, and that it is of the utmost importance for the properties of the stratum corneum and the flora ecosystem. 23
Regarding the perceived effectiveness from the perspective of the volunteers, at the end of the study (D90), 95.35% of them reported improvement in dryness; 91.7% in smoothness; 86.05% in hydration; and 76.74% in desquamation. On D30, there was a statistically significant improvement (p-value < 0.0001) of signs and symptoms: 94.19% of participants noticed improvement in dryness; 81.40% in the smoothness; 82.56% in hydration; and 76.75% in desquamation. These can be deemed considerable amounts, especially in light of the discomfort caused by dryness and desquamation.
Regarding pruritus, as most of the volunteers (60%) did not refer to it on D0, the change in the score during the study was not statistically significant. There was a balance between the reduction in the itching and an absence of alterations.
When a medical treatment is established, the objective is that its effectiveness be clearly perceived by the prescriber, and also by the patient. At the end of the present study, the improvement in xerosis was perceived in similar ways and with excellent results both by researchers and volunteers. Based on the questionnaire of the volunteers' opinions, the product proved to have a good scent and was considered easy to spread, had good consistency and absorption, and was considered good or very good by 97.6% of participants.
Regarding the tolerability of the Hydraporin®, 100% of the volunteers rated the product as excellent (98.84%) and good (1.16%). Only one product-related adverse event took place: a slight increase in cutaneous oiliness was referred by only one volunteer on D60, which was normalized with the continued use of the product.
Cutaneous hydration is a subject of great importance, as xerosis, both of primary or secondary origin, is a very common condition confronted by dermatologists.
Cosmetics companies are increasingly investing in this field, where research is increasingly specialized and detailed. The entailed scientific and technological advancement contributes providing a base for the medical choice of moisturizers. After the clinical outcomes of the present study, it was shown that Hydraporin® is effective in significantly increasing skin hydration (according to corneometry) and extremely efficient in treating signs and symptoms of skin xerosis, according to the assessment of physicians and volunteer patients.
These results therefore validate the product as an effective therapeutic option in cases of cutaneous xerosis, irrespective of the clinical condition, associated or precipitating.
1. Costa A. Tratado Internacional de Cosmecêuticos. Rio de Janeiro: Guanabara Koogan; 2012. p. 376.
2. Draelos ZD. Cosmecêuticos. Elsevier: Rio de Janeiro 2005. p. 264.
3. Heald P, Burton CS, Callaway L. Moisturizing the Skin. N C Med.1983;44(4):234.
4. Costa A, Pires MC, Gonçalves HS, Gontijo B, Bechelli L. Estudo clínico observacional de eficácia e segurança do uso de extratos de Imperatacylindrica e de Triticum vulgare; ceramidas; vitaminas A, C, E e F; silanol (Epidrat® Ultra) em voluntários com xerose secundária a condições dermatológicas específicas - estudo Eudermia. RBM Rev Bras Med. 2009;66(8):249-53.
5. Elias PM. The stratum corneum revisited. J Dermatol. 1996:23(11):756-8.
6. Costa A. Hidratação cutânea. RBM Rev Bras Med. (Ed. Esp. Dermatologia). 2009;66:15-21.
7. Hara M, Ma T, Verkman AS. Selectively reduced glycerol in skin of aquaporin-3-deficient mice may account for impaired skin hydration, elasticity, and barrier recovery. J Biol Chem. 2002;277(48):46616-21.
8. Hara-Chimuka M, Verkman AS. Aquaporin-3 functions as a glycerol-transporter in mammalian skin. Biol Cell. 2005;97(7):479-86.
9. Hara-Chimuka M, Verkman AS. Roles of aquaporin-3 in epidermis. J Invest Dermatol. 2008;128(9):2145-51.
10. Cao C, Sun Y, Healey S, Bi Z, Hu G, Wan S, et al. EGFR-mediated expression of aquapori-3 is involved in human skin fibroblast migration. Biochem J. 2006;400(2):225-34.
11. Proksch E, Lachapelle JM. The management of dry skin with topical emollients-recent perspectives. J Dtsch Dermatol Ges. 2005;3(10):768-74.
12. Simion FA, Abrutyn ES, Draelos ZD. Ability of moisturizers to reduce dry skin and irritation and to prevent their return. J Cosmet Sci. 2005;56(6):427-44.
13. Rawlings AV, Canestrari DA, Dobrowski B. Moisturizer technology versus clinical performance. Dermatol Ther. 2004;17(Suppl 1):49-56.
14. Wu MS, Yee DJ, Sullivan ME. Effect of a skin moisturizer on the water distribution in human stratum corneum. J Invest Dermatol 1983;81(5):446-8.
15. Draelos ZD. Cosmecêuticos. 2ª ed. Elsevier: Rio de Janeiro; 2009. p. 117-24.
16. Elias PM, LaDonna CW, Feingold KR. Epidermal Pathogenesis of inflammatory dermatoses. Am J Contact Dermat. 1999;10(3):119-26.
17. Lupi O, Belo J, Cunha PC. Rotinas de diagnóstico e tratamento da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Guanabara Koogan; 2010. p. 265-7.
18. Kiken DA, Silverberg NB. Atopic dermatitis in children, part 1: epidemiology, clinical features, and complications. Cutis. 2006;78(4):241-7.
19. Ward S. Eczema and dry skin in older people: identification and management. Br J Community Nurs. 2005;10(10):453-6.
20. Jansson C, Johansson S, Lindh-Astrand L, Hoffmann M, Hammar M. The prevalence of symptoms possibly related to the climacteric in pre- and postmenopausal women in Linkoping, Sweden. Maturitas. 2003;3045(2):129-35.
21. Wood LC, Elias PM, Calhoun C, Tsai JC, Grunfeld C, Feingold KR. Barrier disruption stimulates interleukin-1 alpha expression and release from a pre-formed pool in murine epidermis. J Invest Dermatolol. 1996;106(3):397-403.
22. Loden M. Role of topical emollients and moisturizers in the treatment of dry skin disorders. Am J Clin Dermatol. 2003;4(11):771-84.
23. Wilhelm KP, Cua AB, Maibach HI. Skin aging. Effect on transepidermal water loss, stratum corneum hydration, skin surface pH and causl sebum content. Arch Dermatol. 1991;127(12):1806-9.
This study was performed at the Kolderma Instituto de Pesquisa Clínica - Campinas (SP); Complexo Hospitalar Padre Bento de Guarulhos (CHPBG) - São Paulo (SP) e no Hospital Universitário Evangélico de Curitiba (HUEC) - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}